
Abstract
To study the production of anti-platelet factor 4 (anti-PF4)/heparin complex antibodies of Ig (immunoglobulin) G/IgA/IgM using enzyme-linked immunosorbent assay (ELISA; heparin-induced thrombocytopenia [HIT] antibodies) in 79 patients undergoing cardiovascular surgery, we employed Δoptical density (OD) as a marker of HIT-antibody production. The ΔODs were calculated from the differences in the ODs using ELISA. Patient were classified into 3 ΔOD ranges: ΔOD ≥ 1.0, ΔOD ≥ 0.4 to <1.0, and ΔOD < 0.4. The underlying disease, time course of the postoperative platelet count,
Keywords
Introduction
Heparin-induced thrombocytopenia (HIT) is an antibody-mediated reaction caused by exposure to heparin, and it usually occurs 5 to 10 days from the start of heparin therapy. It can occur more rapidly in patients who are reexposed to heparin within 100 days if the antibodies remain in circulation. It has been reported that 20% to 50% of the patients within 10 days after cardiovascular surgery, many of whom have not previously been exposed to heparin, develop anti-platelet factor 4 (anti-PF4)/heparin complex antibodies of Ig (immunoglobulin) G/IgA/IgM which can be detected using enzyme-linked immunosorbent assay (ELISA; HIT antibodies) after heparin exposure. The high frequency of HIT-antibody formation among patients with cardiac disease could involve a high dose of intraoperative heparin and the active release of PF4 during the interaction between blood flow and surface material on coronary artery bypass surgery (CABG). 1
Patients with cardiac surgery who have received heparin during the operation often show seroconversion and rarely develop HIT. 2,3 Primary thrombocytopenia caused by platelet-activating HIT antibodies is exclusively required for HIT diagnosis. However, the risk of HIT development is 1% to 3% when heparin is continued for 1 week after cardiac surgery. Postoperative thrombocytopenia is generally considered to be due to bleeding, sepsis, drugs, or a ventricular assist system, so the presence of thrombocytopenia in patients postcardiac surgery makes it challenging to diagnose HIT. Therefore, a minority of patients with HIT-antibody formation develop HIT and thrombosis, although HIT antibodies detectable by ELISA distinctly increase in complex formation with the accelerated release of PF4 and a large volume of heparin infusion during cardiac surgery. Although the production of HIT antibodies occurs as early as at 5 days and gradually disappears after heparin withdrawal, the relationship between the level of HIT-antibody production and HIT-related clinical variables including thrombocytopenia is not well known. Also, primary thrombocytopenia triggered by platelet-activating HIT antibodies, which include ELISA-detectable HIT antibodies, is regarded as a crucial sign to diagnose HIT. The high prevalence of HIT antibodies and low rate of HIT development after cardiac surgery are yet to be clarified in the context of the production of HIT antibodies and development of HIT. 4–7
To clarify the effect of the new production of HIT antibodies on the development of thrombocytopenia in cardiovascular surgery, we studied changes in Δoptical density (OD) based on differences in the OD using ELISA for 2 weeks. We investigated whether or not the ΔOD is linked to clinical HIT-related variables following cardiovascular surgery.
Materials and Methods
A total of 79 patients undergoing elective cardiovascular surgery were enrolled, including 26 patients receiving aortic vascular surgery, 33 receiving CABG, 14 receiving valvular replacement surgery, and 3 receiving other cardiac surgeries. Of 79 patients, 3 patients were excluded due to other causes of thrombocytopenia, 2 were positive for antihuman leukocyte antigen–antibodies and 1 for dilution thrombocytopenia. Heparin (unfractionated heparin) anticoagulation was applied only during their cardiovascular operations. An initial dose of 300 U/kg of heparin, followed by continuous infusion, with monitoring of the activated clotting time (ACT), was given for the on-pump procedure and a bolus of 3000 U followed with ACT monitoring for the procedure. No patients underwent heparin administration for the prevention or treatment of thrombosis or heparin flush for 14 days postoperatively.
Brain magnetic resonance imaging (MRI) was performed to investigate how HIT-antibody production contributes to the development of stroke after cardiac surgery in 34 patients with each risk factor for smoking, hypertension, diabetes, hyperlipidemia, and chronic renal failure with hemodialysis. 8
Three blood samples were collected from all patients preoperatively, on postoperative days 7 and 14 (±2). Measurements of the platelet count,
To clarify the level of newly produced HIT antibodies that would be induced by a single dose of heparin during a cardiac operation, ΔOD, expressed as the difference between pre- and postoperative OD levels, was applied as a marker of HIT antibody production. Based on the ΔOD calculation, ΔOD = OD ([7 or 14 postoperative days] − [preoperative]), patients were classified into 3 groups: (1) high responder, ≥1.0 ΔOD; (2) moderate responder, from ≥0.4 to <1.0 ΔOD; and (3) low responder, <0.4 ΔOD.
To avoid the influence of preexisting HIT antibodies, 9 patients with ELISA-positive results were excluded: 1 of the 9 patients was positive for both the tests before surgery. 12 Therefore, a total of 67 patients underwent analysis.
The study protocol was approved by the local ethics committee of Yamanashi University. Fisher exact test and the Mann-Whitney U test were used to evaluate categorical data regarding the platelet counts and continuous variables. The Kruskal-Wallis test was used to evaluate differences among the 3 groups, classified by anti-heparin/PF4 antibody production.
Results
No differences in the ΔOD titer as a marker of HIT-antibody production were detected among the groups of underlying diseases. Also, cardiopulmonary bypass procedures did not affect the level of ΔOD among the 3 groups. In brain MRI for detecting postoperative cerebral thrombosis, asymptomatic cerebral infarction (<1 cm2 in size) was detected in 5 of the 34 patients. Three patients were high responders. Of the 3 patients, 1 was both ELISA- and SRA-positive. However, HIT was not noted from days 5 to 10.
The ΔOD, expressed as a weekly change, was used to classify patients into 3 groups: high responder: ≥1.0, moderate responder: 0.40 to <1.0, and low responder: <0.40. In the high and moderate responders, new production of HIT antibodies increased within a week after heparin cessation. The new production between 7 and 14 days became undetectable in 2 responders. Antibody production peaked 7 days following heparin withdrawal, and then all production ceased in the next 7 days. Of the 13 high responders, 6 retained SRA-positivity in the absence of newly produced HIT antibodies. Despite the patients having platelet-activating HIT antibodies, they showed no HIT-associated platelet count fall for 5 to 10 postoperative days (Table 1).
Classification into 3 Responder Groups According to ΔOD Titers as a Marker of HIT-Antibody Production.a,b
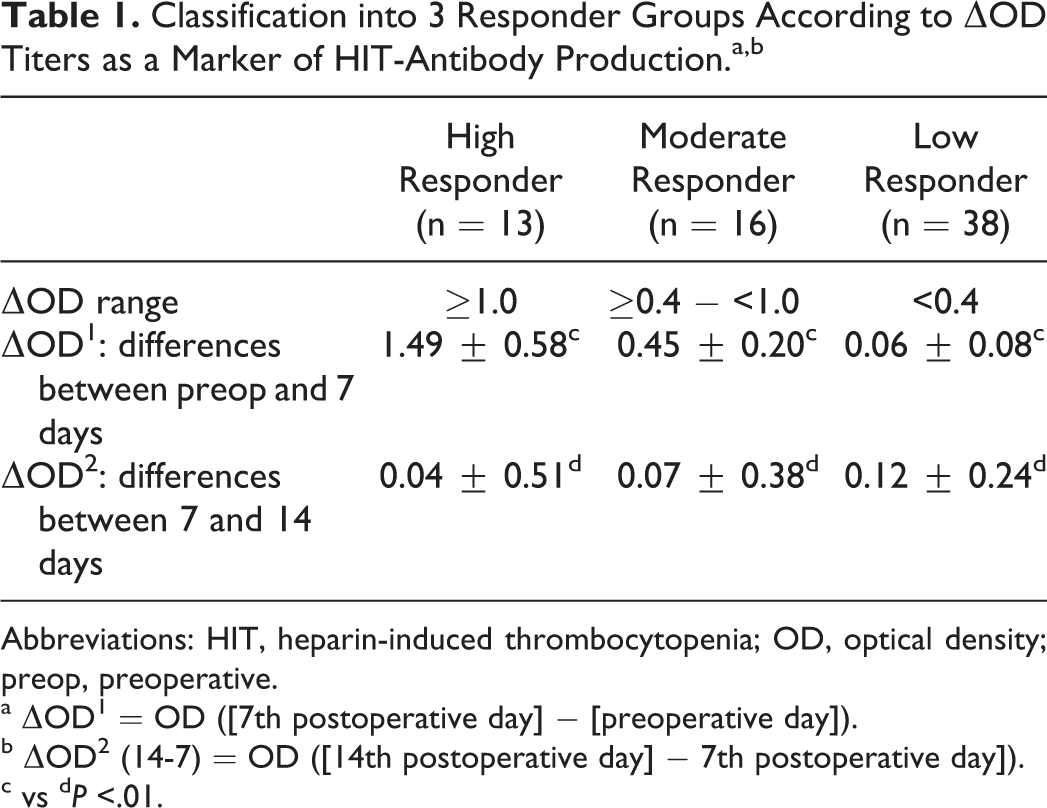
Abbreviations: HIT, heparin-induced thrombocytopenia; OD, optical density; preop, preoperative.
a ΔOD 1 = OD ([7th postoperative day] − [preoperative day]).
b ΔOD 2 (14-7) = OD ([14th postoperative day] − 7th postoperative day]).
c vs d P <.01.
Postoperative platelet counts were significantly increased on day 14 compared with the preoperative level in each of the 3 groups. No differences in the platelet counts by the 3 tests preoperatively and on postoperative days 7 and 14 were found among the 3 groups. The postoperative platelet counts were not influenced by the postoperative ΔOD titers (Table 2).
Perioperative Platelet Counts for the 3 Responder Groups (×109/L).
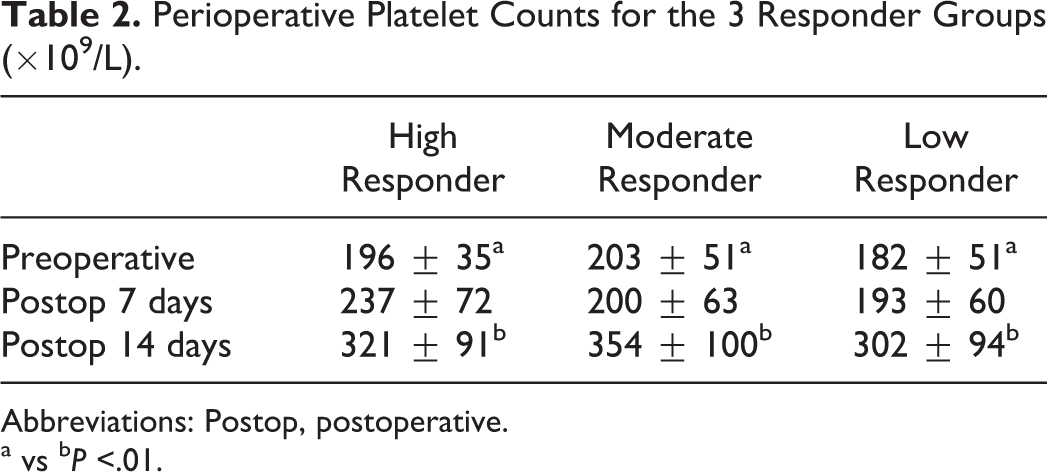
Abbreviations: Postop, postoperative.
a vs b P <.01.
Furthermore, to evaluate the differences in the platelet count fall rate between SRA-positive and SRA-negative high responders, 3 indices of the fall rate were introduced: percentage of the fall rate = (day 7) − (preoperative), percentage of the increase rate = (day 14) − (day 7), and percentage of the total change rate = (increase rate) − (fall rate). No differences in the platelet fall rate and increased rate were noted on day 7 and day 14, respectively, between SRA-positive and -negative patients.
In the 13 high responders with ≥1.00 ΔOD, 6 patients were SRA-positive and had no HIT-related platelet count fall. Their nadirs of thrombocytopenia were noted until the third postoperative day. They did not have definite HIT due to the lack of a corresponding fall in platelet counts during days 5 to 10.
When reactive thrombocytosis was defined as a platelet count of ≥400 × 109/L on day 14, the development of reactive thrombocytosis was identified in 14 (20.8%) of the total patients. Although 3 of the 14 patients with reactive thrombocytosis had a positive SRA, no relationship between the presence of platelet-activating HIT-antibodies and occurrence of reactive thrombocytosis was noted.
The
Discussion
We introduced the ΔOD to clarify the new production of HIT antibodies after cardiovascular surgery and whether changes in ΔOD titers were linked to clinical HIT-related variables.
The 3 groups, consisting of high, moderate, and low responders, showed no differences in postoperative platelet counts. The platelet counts among the groups were not influenced by the level of HIT-antibody production in the context of postoperative thrombocytopenia and postoperatively reactive thrombocytosis. All patients showing postoperative platelet recovery by day 14 were identified. In the high responders, a peak titer of ΔOD appeared 7 days after heparin withdrawal, and the titers decreased to nonproduction levels under ΔOD of 0.4 on day 14, although the absolute OD levels were maintained with a positive ELISA. Patients with cardiovascular surgery have a high risk of generating HIT antibodies, but the increased production of HIT antibodies would be insufficient to develop HIT and pathologic platelet falls unlikely to be masked with the progression of reactive thrombocytosis. However, the presence of primary thrombocytopenia after cardiac surgery is a crucial diagnostic indicator of HIT, although other causes of thrombocytopenia, such as hemodilution, platelet consumption, sepsis, and DIC, often coexist in a critical condition. 13
Reactive thrombocytosis is characterized by accelerated platelet production in response to thrombocytopenia owing to surgical procedures, tissue damage, and blood loss. As reactive thrombocytosis caused by cardiac surgery takes 1.5 days or more for a significant marrow response to thrombocytopenia, the platelet count begins to increase from days 2 to 3 and rises on days 7 to 12 (Table 3). 14,15 The occurrence of reactive thrombocytosis was observed to be independent of the level of HIT-antibody production, shown as ΔOD titers. When reactive thrombocytosis postoperatively occurs coincidentally with the onset of immune-mediated thrombocytopenia, the platelet count profile displays a biphasic pattern characterized by an abrupt decline between days 5 and 10. 16 Therefore, it is not difficult to determine that a patient following cardiovascular surgery without HIT does not have HIT.
Rate of RT Defined as a Platelet Count ≥400 × 109/L on Postoperative Day 14.
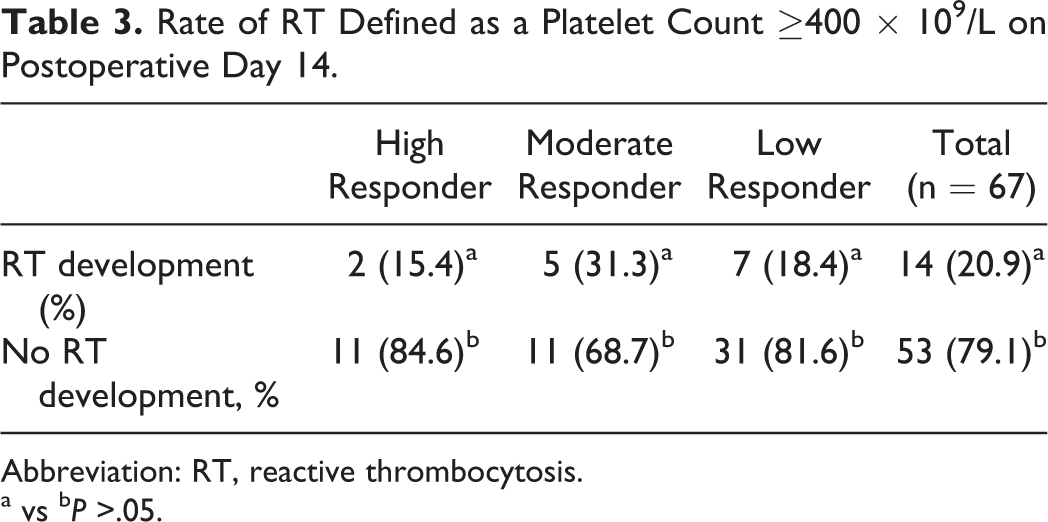
Abbreviation: RT, reactive thrombocytosis.
a vs b P >.05.
However, in 2 patients showing heparin-induced thrombosis without thrombocytopenia after CABG, immune-mediated thrombocytopenia was presumed to be masked by reactive thrombocytosis. 17,18 As no relationship between the presence of platelet-activating HIT antibodies and occurrence of reactive thrombocytosis was detected in the study, the development of HIT-derived thrombocytopenia is suggested to have no influence on coexistence with postoperative thrombocytosis. As ELISA- and SRA-positive conditions lacking HIT platelet criteria were considered as HIT unlikely, none of the 6 high responders with a titer of ΔOD ≥ 1.0 could be diagnosed with HIT during the second week postsurgery. 19
In moderate responders, an ELISA- and SRA-positive patient with CABG showed a platelet count fall suggestive of HIT on day 5, and the platelet count fall from the preoperative level was 76% on day 2, 69% on day 5, and 48% on day 7. On day 14, his platelet count of ≥ 400 × 109/L was defined as reactive thrombocytosis. The profile of platelet count was not compatible with the HIT pattern of monophasic, persistent thrombocytopenia because of the normal postoperative thrombocytopenia that started by day 5. 16 The platelet count profiles of falls by platelet-activating HIT antibodies in 3 patients with HIT were not overwhelmed by the increasing platelet production due to postoperative thrombocytosis, so the results indicate that the occurrence of immune-mediated thrombocytopenia is highly predictive of HIT following cardiac surgery. 19
Despite the fact that reactive thrombocytosis in the postoperative stage seems to be predominant over HIT-derived thrombocytopenia, the platelet count profile of HIT is characterized by an abrupt decrease within 1 to 2 days in the course of postoperative thrombocytosis. Therefore, it is reasonable to assume that the diagnosis of HIT can be carried out independent of the presence of postoperative thrombocytosis.
In conclusion, ΔOD was evaluated as a marker for the production of HIT antibodies. The level of ΔOD did not affect clinical variables including thrombocytopenia that were likely to contribute to the development of HIT. The production of HIT antibodies after heparin withdrawal increased on day 7 and then reached a trace level on day 14. It was demonstrated that HIT-antibody production is in remission unless there is evidence of a further increase during the second week postsurgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.