
Abstract
Quality control of the platelet activation assays to diagnose heparin-induced thrombocytopenia (HIT), 14C-serotonin release assay (SRA) and platelet aggregation test (PAT) has yet to be established due to lack of reference standards and the difficulty of obtaining significant amounts of HIT antibodies from patients with HIT. We prepared a murine monoclonal antibody to human platelet factor 4 (hPF4)/heparin complexes (HIT-MoAb) and investigated the platelet activating action of HIT-MoAb by using SRA and PAT. The HIT-MoAb activated human platelets at low heparin concentration and the platelet activations were inhibited at high heparin concentration in both SRA and PAT. The HIT-MoAb produced a concentration-dependent effect. Moreover, the platelet activation at low heparin concentration was inhibited by anti-FcγRIIa antibody. These results indicated that HIT-MoAb has characteristics similar to human HIT antibodies regarding heparin-dependent platelet activation. Therefore, it is suggested that HIT-MoAb has the potential to be a positive control or reference standard in platelet activation assays.
Keywords
Introduction
Heparin-induced thrombocytopenia (HIT) is a serious side effect of heparin treatment that is characterized by thrombocytopenia and venous or arterial thrombosis. 1 The HIT is caused by the generation of antibodies (HIT antibodies) against platelet factor 4 (PF4)/heparin complexes that have strong platelet-activating properties. 2 The immune complex formed by HIT antibodies causes platelet activation when the Fc portion binds to the Fc receptors (FcγRIIa) on platelet membranes. 3 Microparticles are released from the activated platelet leading to the activation of coagulation pathways. 4 The immune complex also activates vascular endothelial cells 5 and monocytes, 6,7 and tissue factor is expressed on those cells, finally producing thrombin, which leads to thrombocytopenia and thrombosis.
There are 2 methods for detecting HIT antibodies—immunoassays and functional assays. 8 –10 Immunoassays include several enzyme-linked immunosorbent assays (ELISAs) and particle agglutination assays. 10 Functional assays typically include the 14 C-serotonin release assay (SRA) 11 and the heparin-induced platelet aggregation test (PAT). 12 Specimens from previously diagnosed HIT antibody-positive patients are used as the positive control in these tests. However, quality control and standardization have not been established 8,13 because there is no positive control common to different laboratories and there are no patient-derived HIT antibodies abundant enough to be distributed for use as reference standards. We have produced a murine monoclonal antibody to human PF4 (hPF4)/heparin complexes (HIT-MoAb). Here, we investigated whether HIT-MoAb exhibited the same reaction as HIT antibodies in SRA and PAT.
Materials and Methods
Preparation of a monoclonal antibody to hPF4/heparin (HIT-MoAb)
Recombinant human PF4 (r-PF4) was expressed in the Bacillus subtilis system as soluble protein and purified from culture medium using heparin sepharose column. Porcine sodium heparin (molecular weight: 13 500-15 000) was obtained from Calbiochem (Darmstadt, Germany).
Two 6-week-old female BALB/C mice were first injected intraperitoneally and subcutaneously with a 0.5 mL mixture of 60 μg of r-hPF4 and heparin (1.8 U/mL) combined with an equal amount of Freund complete adjuvant. The second and third time the mice were given half that amount by intraperitoneal injection. And the fourth time, they were given the same amount as the first time. Spleen cells were obtained 4 days after a final injection and fused with the P3X63-Arg8-U1 murine myeloma cells in the presence of 50% polyethylene glycol 1450 14,15 . The fused cells were selected in RPMI-1640 medium containing 10% fetal calf serum, 0.1 mmol/L hypoxanthine, 0.4 μmol/L aminopterin, and 16 mmol/L thymidine The hybridoma, after screening for anti-PF4/heparin antibodies by ELISA, was cloned. The cloned hybridoma was cultured and then injected into the mice’s abdominal cavities in order to generate ascites. The monoclonal antibody immunoglobulin (Ig)G was purified from ascitic fluid using protein G column. The subclass of these IgG antibodies was IgG1κ.
14 C-Serotonin Release Assay
Acid citrate dextrose (ACD) tubes (solution A: 22.0 g/L trisodium citrate, 8.0 g/L citric acid, and 24.5 g/L dextrose; BD Diagnostics, Franklin Lakes, New Jersey) were used for donor blood collection. Apyrase (Grade III), Triton-X, EDTA and buffer reagents were from Sigma Chemicals (St Louis, Missouri). Unfractionated porcine sodium heparin (UFH) was obtained from American Pharmaceutical Partners, Inc (Los Angeles, California). Radiolabeled serotonin was [ 14 C] 5-hydroxytryptamine creatinine sulfate (GE Healthcare, Arlington Heights, Illinois).
SRA-positive specimens from patients with HIT archived at Loyola University Medical Center’s SRA Clinical Laboratory were used, with approval of the University Institutional Review Board, as positive controls in these studies.
The HIT-MoAb was evaluated at concentrations of 62.5, 125, 250, and 500 μg/mL (final concentrations were 12.5, 25, 50, and 100 μg/mL). The dose–response assays were replicated with 3 individual platelet donors. In addition, the 62.5 µg/mL HIT-MoAb concentration was studied in another 15 SRA runs.
The SRA was adapted from that described by Sheridan et al. 11 Blood from a normal donor, known to be reactive in the assay, was collected in ACD, then platelet-rich plasma (PRP) was prepared (135g, 15 minutes) and incubated with 50 nCi/mL 14 C-serotonin at 37°C for 45 minutes. The platelets were centrifuged (600g, 10 minutes), washed with calcium and albumin-free Tyrode (137.5 mmol/L NaCl, 2.7 mmol/L KCl, 12 mmol/L NaHCO3, 0.4 mmol/L NaH2PO4, 2 mmol/L MgCl2, 4.4 mmol/L 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid [HEPES], 5.5 mmol/L dextrose, pH 6.2), containing 1.5 U/mL apyrase, spun again and then suspended in albumin-free Tyrode (137.5 mmol/L NaCl, 2.7 mmol/L KCl, 12 mmol/L NaHCO3, 0.4 mmol/L NaH2PO4, 1 mmol/L MgCl2, 2 mmol/L CaCl2, 4.4 mmol/L HEPES, 5.5 mmol/L dextrose, pH 7.4). In 1 assay, the final buffer contained the FcγIIa receptor-blocking antibody IV.3 at a final concentration of 10 µg/mL.
The
14
C-labeled platelets were incubated in a V-bottom polypropylene 96-well plate with HIT-MoAb or with control sera and UFH at final concentrations of 0.1 or 100 U/mL. To neutralize possible residual thrombin or other enzymes, sera were heat inactivated (56°C, 45 minutes) and then centrifuged (800g, 10 minutes) prior to assay. After 60 minutes of incubation at room temperature on a rotating shaker, 100 µL of EDTA (4% in saline) was added to stop the reaction. The assay plates were centrifuged (1800g, 5 minutes) and radioactivity in the supernatant was counted (RackBeta Liquid Scintillation Counter, Perkin Elmer, Shelton, Connecticut) in test wells and also in wells of untreated, labeled platelets (background) and platelets lysed with 10% Triton-X (total release). Platelet response was quantified as percent serotonin release, according to the following formula:

An SRA-positive specimen is one that causes greater than 20% serotonin release in response to a low concentration of heparin, together with inhibition of that response in the presence of excess heparin. Known SRA-positive and -negative sera are included as controls in every assay run.
Platelet Aggregation Test
Unfractionated porcine calcium heparin (Caprocin) was obtained from Sawai Seiyaku, (Osaka, Japan). IV.3, the anti-FcγRIIa antibody, was provided by Dr Kaneo Satoh (University of Yamanashi, Japan).
Blood from 4 volunteer donors known to be reactive to HIT plasma was collected into 3.2% sodium citrate tubes and then centrifuged at 120g for 5 minutes at room temperature. This supernatant was used as donor PRP. Donor PRP and HIT-MoAb were mixed together at a ratio of 1 volume:1 volume and incubated for 10 minutes at 37°C. Then platelet aggregation was measured with an aggregometer (PA200, Kowa, Tokyo) for 30 minutes with heparin at a final concentration of 1 or 100 U/mL. The HIT-MoAb was adjusted to concentrations of 60, 120, and 200 μg/mL (final concentrations were 27, 54, and 90 μg/mL). IV.3 was used at a final concentration of 10 μg/mL. A maximum aggregation rate (the rate of maximum light transmittance: LTmax %) of 20% or more was considered to be aggregation positive.
Results
14 C-Serotonin Release Assay
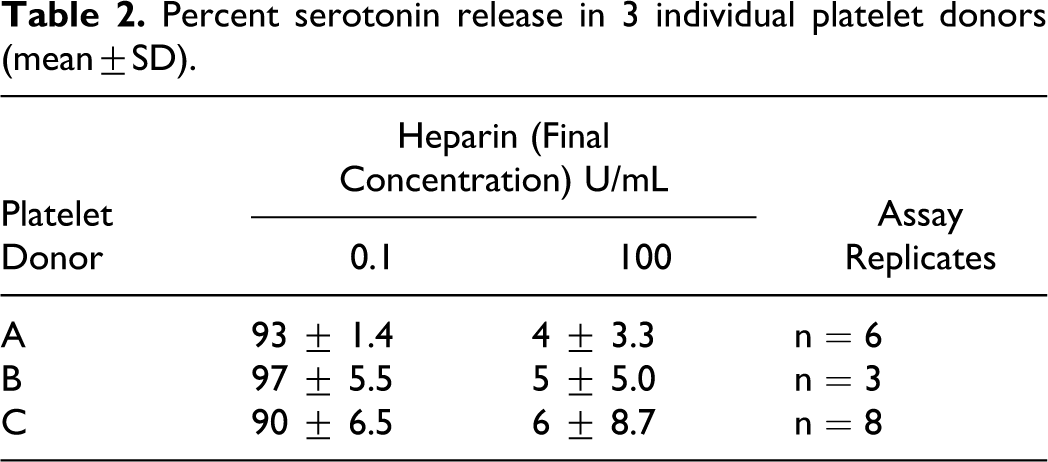
In the SRA, HIT antibodies cause platelet activation at low heparin concentration, but not at high heparin concentration 11,16 ; the identical response was seen with HIT-MoAb. All concentrations tested caused >80% release with 0.1 U/mL heparin and <20% serotonin release in the presence of 100 U/mL heparin (Table 1). As with human HIT antibodies, HIT-MoAb-mediated serotonin release was blocked in the presence of anti-FcγRIIa antibody ([IV.3] data not shown). There was slightly increased serotonin release in the presence of 100 U/mL heparin at the 2 highest concentrations of HIT-MoAb; this is characteristic of very high titer HIT antibodies obtained from patients as well. 17 The SRA response to concentrations of HIT-MoAb at 62.5 μg/mL was very consistent between several platelet donors and over multiple assay replicates (Table 2).
Percent Serotonin Release (Mean ± SD)
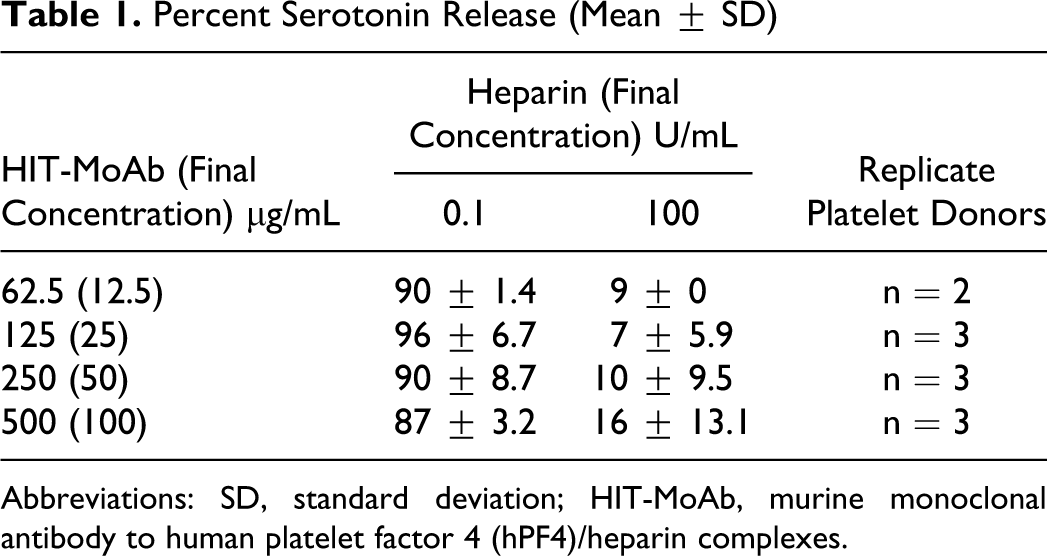
Abbreviations: SD, standard deviation; HIT-MoAb, murine monoclonal antibody to human platelet factor 4 (hPF4)/heparin complexes.
Percent serotonin release in 3 individual platelet donors (mean±SD).
Platelet Aggregation Test
The HIT-MoAb caused platelet aggregation at 1 U/mL final heparin concentration. Platelet aggregation was negative when no antibody was added. Platelet aggregation was negative when HIT-MoAb concentration was at 60 μg/mL and positive when at 120 μg/mL and 200 μg/mL. Also, the area under the curve had increased more at 200 μg/mL than at 120 μg/mL, indicating a concentration-dependent effect of HIT-MoAb for platelet aggregation activity (Table 3).
Platelet Aggregation at Low Heparin Concentration (Mean ± SD)
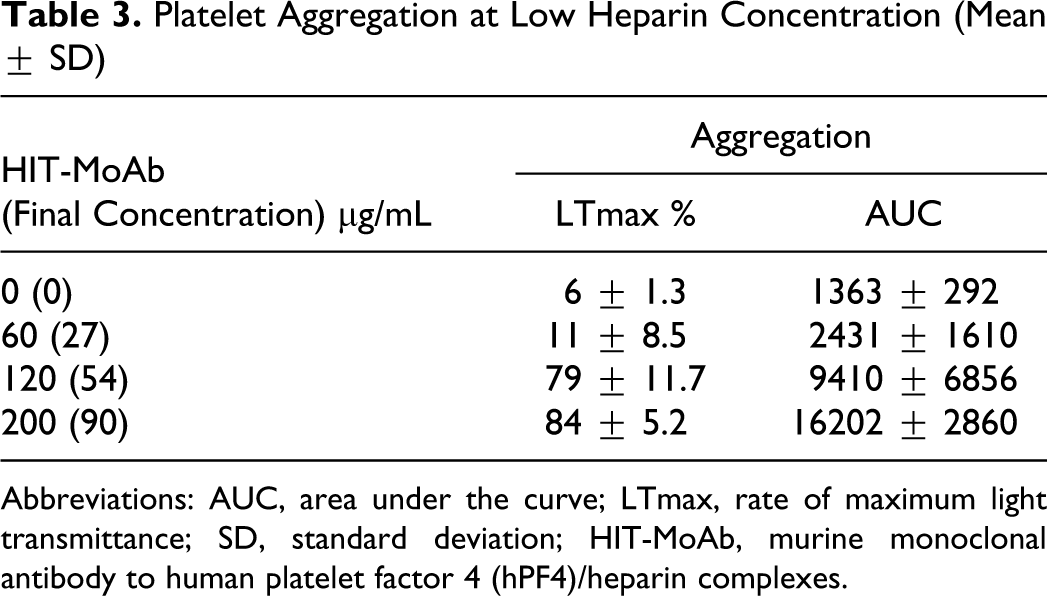
Abbreviations: AUC, area under the curve; LTmax, rate of maximum light transmittance; SD, standard deviation; HIT-MoAb, murine monoclonal antibody to human platelet factor 4 (hPF4)/heparin complexes.
Table 4 shows platelet aggregation at final concentrations of heparin of 1, 100, and 1 + IV.3 with HIT-MoAb concentration at 200 μg/mL. The HIT-MoAb caused platelet aggregation (mean: 84%) at 1 U/mL of heparin, on the other hand, platelet aggregation at 100 U/mL of heparin or at 1 U/mL of heparin + IV.3 was negative. This is the identical response to HIT antibodies obtained from patients.
Inhibition of Platelet Aggregation at High Heparin Concentration or IV.3 (Mean ± SD)
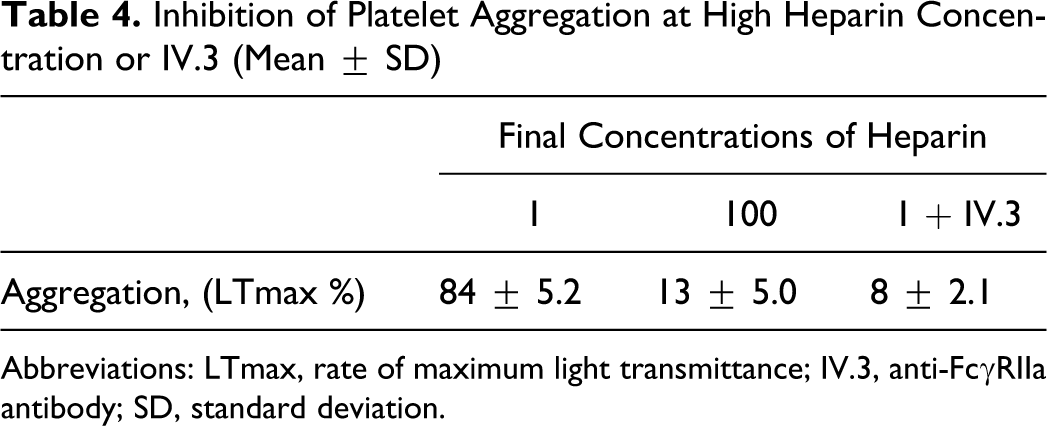
Abbreviations: LTmax, rate of maximum light transmittance; IV.3, anti-FcγRIIa antibody; SD, standard deviation.
Discussion
The platelet activation assays for detecting HIT antibodies are specific and useful to diagnose HIT. It is considered possible to diagnose HIT when the platelet activation assay is positive for HIT antibodies. 18 However, quality control of the assays remains problematic due to the difficulty of obtaining large amounts of antibodies from patients with HIT. There is a need for positive control material to validate HIT assays and to help identify optimal donors whose platelets are sensitive to HIT antibodies. 8 So, there is consideration that the monoclonal antibodies with reactivity similar to HIT antibodies will become a useful tool as a positive control in the platelet activation assays.
Arepally et al produced a murine monoclonal antibody to hPF4/heparin complexes (KKO) by administration of recombinant hPF4/heparin complexes to sensitized mice. They reported that KKO activated human platelets in the SRA in the presence of low concentrations of heparin (0.5-2.5 U/mL) when hPF4 (10 µg/mL) was added to PRP, and the platelet activation was inhibited by anti-FcγRIIa antibody (IV.3). 19
In the present study, we also generated a murine monoclonal antibody, HIT-MoAb, by administration of recombinant hPF4/heparin complexes to mice in a similar way to KKO and investigated the characteristics of the platelet activation by HIT-MoAb with SRA and PAT. The HIT-MoAb activated human platelets in the presence of low concentrations of heparin; furthermore, high concentrations of heparin and anti-FcγRIIa antibody (IV.3) inhibited the platelet activation induced by HIT-MoAb. These results indicate that the platelet activation by HIT-MoAb is comparable to the response to human HIT antibodies and that the reaction was caused by an immunological mechanism through FcγRIIa on the platelet membrane. In contrast with KKO, HIT-MoAb did not require the addition of hPF4 in order to activate platelets in the SRA and PAT. Platelet activation induced by HIT antibodies requires PF4 since the platelet aggregation induced by HIT antibodies is inhibited by the monoclonal anti-PF4. 20 However, it has been demonstrated that PF4 necessary for HIT-antibody-mediated platelet activation is present in these reaction systems 16 and that platelets can be activated by purified IgG HIT antibodies without adding PF4 in the platelet activation assays (both using washed platelets and PRP). 20 On the other hand, there is a difference in the subtypes of IgG in HIT-MoAb and KKO; HIT-MoAb is IgG1κ while KKO is IgG2bκ. De Reys et al reported that the platelet activation induced by murine monoclonal antibodies depended on the antibody subtype. 21 The differences in IgG subtypes might influence platelet activation.
Platelet activation assays have been regarded as the “gold standard” for diagnosis of HIT. However, these tests are only performed in a small number of laboratories in the world and there is no standardization among laboratories. 8,9,13 Each laboratory uses HIT-antibody positive specimens from previously diagnosed patients as positive control in diagnostic tests. The HIT-antibody positive specimens are also needed to select for platelet donors with high reactivity to the antibodies, a key point in improving sensitivity of the platelet activation tests. 11,12,22 However, in most general laboratories, it is difficult to obtain sufficient HIT specimens to use as positive control and for assessing platelet donors. And it is not possible to use non-HIT-related monoclonal antibodies to assess the responsiveness of donor platelets in HIT assays. Warkentin et al reported that there is no correlation between platelet donor reactivity to HIT serum and activation of the donor platelets by 3 IgG1-type murine monoclonal antibodies (Raj-1, JS-1, and Jun-1), which activate platelets through the Fc receptor. 22
Our study demonstrates that HIT-MoAb behaves like human HIT antibodies in the SRA and PAT. In these tests, without addition of PF4, HIT-MoAb activates platelets in the presence of low heparin and the response is inhibited in the presence of excess heparin. In contrast to antibodies from patients with HIT, HIT-MoAb has homogeneous properties and can be obtained in large quantities. We suggest that it may be possible to use HIT-MoAb as a positive control in platelet activation assays, to assess donor platelets to maximize assay sensitivity and to compare or standardize HIT assay procedures between laboratories.
Needless to say, the further study over a wider range of concentrations and with a larger sample of donor’s platelets is required for the HIT-MoAb to be established as a quality control reagent and they are now under investigation in our laboratories.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.