
Abstract
A retrospective study was performed to elucidate the characteristics of heparin-induced thrombocytopenia (HIT) in newly treated hemodialysis (HD) patients who essentially required anticoagulation with unfractionated heparin (UFH). Seventy-eight patients suspected of having HIT within 3 months of starting HD with UFH were selected for this study. Their platelet counts were routinely followed, and anti-PF4/heparin complex antibodies (HIT antibodies) were measured with enzyme-linked immunosorbent assay (ELISA) until the titer became negative. The characteristics of thrombocytopenia were a platelet count of ≤150 × 109/L and/or decrease of ≥30% and as caused by the intermittent use (3 times/a week) of UFH during HD. Fifty-five patients showed unexpected clotting in the extracorporeal circuit and/or arteriovenous fistula (AVF) thrombosis, while 23 patients had neither of these complications. The patients were classified into HD-related and non-HD-related thrombus groups. The impact of various combinations of the 3 clinical factors (thrombocytopenia, timing, and HD-related thrombus) and the results of ELISA as a laboratory factor were examined. A combination of 2 platelet factors (thrombocytopenia and timing) and ELISA positivity did not reveal the presence of HIT, while a combination of the 3 clinical factors and a positive ELISA improved the accuracy of HIT diagnosis. The findings on the 4-factor combination were supported by high rates of seroconversion in a serotonin release assay. Combining appropriate clinical factors and a positive ELISA may lead to the proper management of HD patients suspected of having HIT. In conclusion, while HD patients showed a drop of ≤150 × 109/L or ≥30% on days 7 to 30, unexpected clotting in the circuit and/or AVF thrombosis was considered as a sign of HIT development.
Keywords
Introduction
Heparin-induced thrombocytopenia (HIT) is a serious adverse reaction, and immune-mediated antibodies against the PF4/heparin complex (HIT antibodies) are involved in its pathogenesis. In the clinical setting of using heparin in hemodialysis (HD), the incidence of HIT is reported to be as high as 3.8% early after the introduction of HD. 1 Heparin-induced thrombocytopenia demands much more attention in patients on HD requiring extracorporeal circulation because anticoagulation with heparin is essential. There have been a few reports on the association between clotting in the circuit and arteriovenous access thrombosis (arteriovenous fistula [AVF] thrombosis) in relation to HIT, although the frequency of the seroconversion of HIT antibodies in HD has been evaluated.2–4 It remains unclear whether clotting in the circuit and arteriovenous access occlusion can be characterized HIT signs in HD patients with suspected HIT.
Although deep vein thrombosis (DVT), pulmonary embolism (PE), cerebral stroke, myocardial infarction, and limb gangrene are all well-known complications of HIT, it has not been evaluated whether circuit clotting and AVF thrombosis are indicators of HIT in newly treated patients on HD.
The study was carried out to clarify the diagnostic involvement of circuit clotting and AVF thrombosis as a HIT-related thrombus in HD patients with clinically suspected HIT. Also, we examined whether HIT antibody testing by the PF4/heparin enzyme-linked immunosorbent assay (ELISA) was useful to confirm HIT in HD patients.
Participants and Methods
Participants with chronic uremia due to a creatinine clearance of <10 mL/min and a serum creatine level of >8 mg/dL were newly treated with HD. They were referred to a clearinghouse for HIT of Kobe Research Projects on Thrombosis and Haemostasis for HIT antibody testing. Seventy-eight consecutive patients suspected of having HIT by their treating physicians were retrospectively chosen from medical records, covering the period between January 2004 and December 2006. The underlying disease was diabetic nephropathy (n = 46), chronic glomerulonephritis (n = 17), systemic lupus erythematosus (SLE) or a related disease (n = 7), nephrosclerosis (n = 3), cystic kidney (n = 2), unknown (n = 2), or renal cancer (n = 1). The participants (mean age: 70 ± 14.3 years, 43 males and 35 females) met all of the following criteria: HD was carried out 3 times a week with a hollow-fiber dialyzer and no heparin-coated materials; within 90 days after the introduction of HD using unfractionated heparin (UFH) 4 ; with the first use of the anticoagulant and a decrease in the platelet count of ≤150 × 10 9 /L or a fall of ≥30% from heparin usage; and no other causes of thrombocytopenia. The nadir of the fall in the platelet counts was counted in days from the first use of heparin to the day of a drop of ≤150 × 10 9 /L or fall of ≥30%. In addition to systemic HIT-associated thrombosis, circuit clotting and AVF thrombosis in relation to thrombocytopenia were evaluated as potential signs of HD-HIT. Clotting was defined based on visible clots in the dialyzer, air trap, and venous line, and, if found, HD was suspended before the scheduled time. New thrombotic occlusion in AVF related to the onset of HIT was diagnosed based on ultrasonic and angiographic procedures. Blood specimens were withdrawn at the time of suspected HIT and tested for immunoglobulin (IgG, IgA, and IgM) antibodies against the PF4/heparin complex (HIT antibodies) by ELISA (PF4 Enhanced, GTI, Wisconsin). An optical density (OD) of >0.4 was taken as a positive result. If positive, the measurement was repeated until the titer became negative. The serotonin release assay (SRA) was performed using platelets obtained from normal donors known to be highly reactive to HIT-positive serum. The platelets were incubated with 14 C-radiolabeled serotonin and then washed and responded in calcium-containing assay buffer. Platelet activation resulting in granule release was detected by the presence of radioactivity in the supernatant. Heparin-induced platelet activation was defined as greater than 20% serotonin release at a low dosage of 0.1 U/mL of heparin and less than 20% release at a high dosage of 100 U/mL.5,6
Fifty-five of 78 patients with a clotted circuit alone (n = 42), AVF thrombosis with clotting of the circuit (n = 8), and AVF thrombosis alone (n = 5) were classified into an HD-related thrombus group (thrombus group). In this group, 5 patients with thrombosis complicated at the time of suspected HIT included 3 with DVT, 1 with DVT + PE, and 1 with DVT + limb gangrene. Twenty-three of 78 patients without clotting of the circuit and AVF thrombosis were classified into a non-HD-related thrombus group (nonthrombus group). The latter group included 2 patients with thrombosis: 1 with DVT and 1 with DVT + PE.
Permission was obtained from the treating physicians and the ethics board to perform the study. Statistical analysis of sensitivity, specificity, and positive and negative predictive values was performed using the standard formulas with a 2 × 2 contingency table. For parametric variables, Student t test was used; and for nonparametric variables, the Mann-Whitney test was used.
Results
The 78 patients divided into thrombus and nonthrombus groups were compared in terms of the platelet count, fall in the count, timing of the fall, and the titer of OD with ELISA. No significant differences in the 3 platelet-related parameters were identified between the 2 groups. However, the OD titer was significantly higher in the thrombus group (Table 1 ). There were no significant differences among the 4 parameters including the OD between 5 patients with systemic HIT-associated thrombosis in the thrombus group and 2 patients with systemic thrombosis in the nonthrombus group. The presence of systemic thrombosis at the time of suspected HIT did not serve as a bias for differences in the 2 groups. In the thrombus group, there were also no differences in these parameters among the 3 subgroups of the circuit clotting alone, AVF thrombosis alone, and both combined. Thus, each factor of circuit clotting, AVF thrombosis, and the presence of systemic thrombosis did not separately influence the characterization of the thrombus group.
Comparison of 3 Platelet-Related Factors and Titers of HIT Antibodies Between HD Thrombus and non-HD Thrombus Groups in 78 Patients Suspected With HIT on Hemodialysis
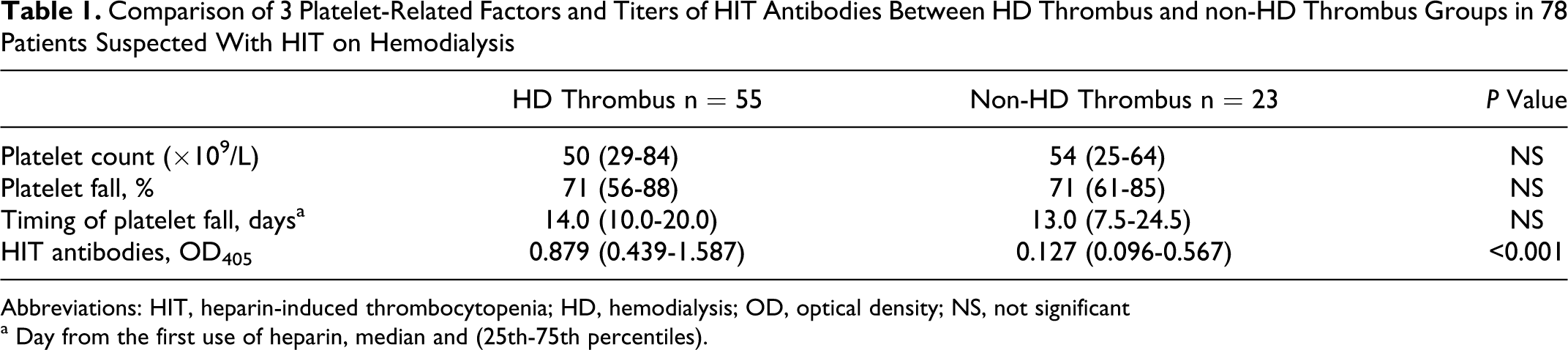
Abbreviations: HIT, heparin-induced thrombocytopenia; HD, hemodialysis; OD, optical density; NS, not significant
a Day from the first use of heparin, median and (25th-75th percentiles).
The frequencies of HD-related thrombus and HIT antibody positivity are shown in relation to the timing of the fall in the platelet count ( 1). The highest frequency for the nadir of thrombocytopenia was on days 11 to 15 from the first use of heparin and the second one was on days 6 to 10. The occurrence of HD thrombus versus non-HD thrombus increased on days 21 to 30, in which the seroconversion rate peaked at 100% and then decreased.
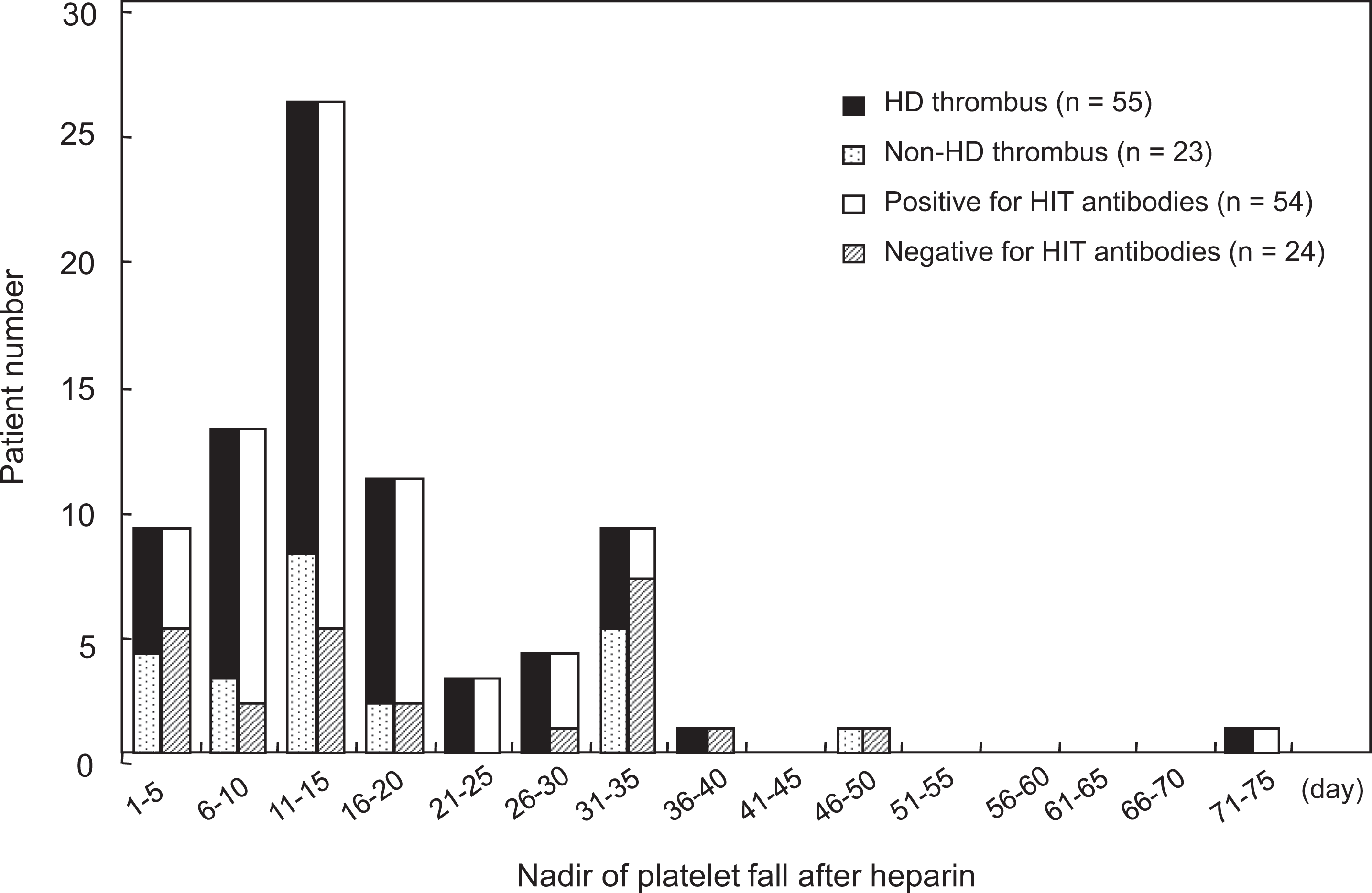
Nadir of thrombocytopenia in 78 suspected cases of HIT on hemodialysis (HD).
To clarify the timing of the platelet count fall in HD patients, the following 4 ranges (median: 14 days) were set: 25th to 75th percentile (days 10-20), 20th to 80th percentile (days 8-26), 15th to 85th percentile (days 7-30), and 10th to 90th percentile (days 5-34). There was no significant relationship between any of the ranges and the level of thrombocytopenia. Also, no relation was noted between each range and the formation of HD-related thrombus. When the fall occurred on days 7 to 30 (15th-85th percentile), the relation between the timing of the fall and HIT antibody positivity was the most significant (P < .001). Further, in the nonthrombus group that deviated from the 15th to 85th percentile (<day 7 and >day 30), no patient tested positive for HIT antibodies was noted. Thus, the range of the fall on days 7 to 30 was the most suitable for assessing HD patients.
The period from days 7 to 30 was divided into days 7 to 14 and days 15 to 30 before and after the median of day 14. When the timing of the fall occurred on days 15 to 30, the thrombus group was characterized by significantly higher levels of the positive rate and titer in ELISA compared with the nonthrombus group. Significantly higher levels of OD on <day 7 and days 15 to 30 in the thrombus group revealed that HIT antibodies may affect thrombotic formation in each term ( 2).
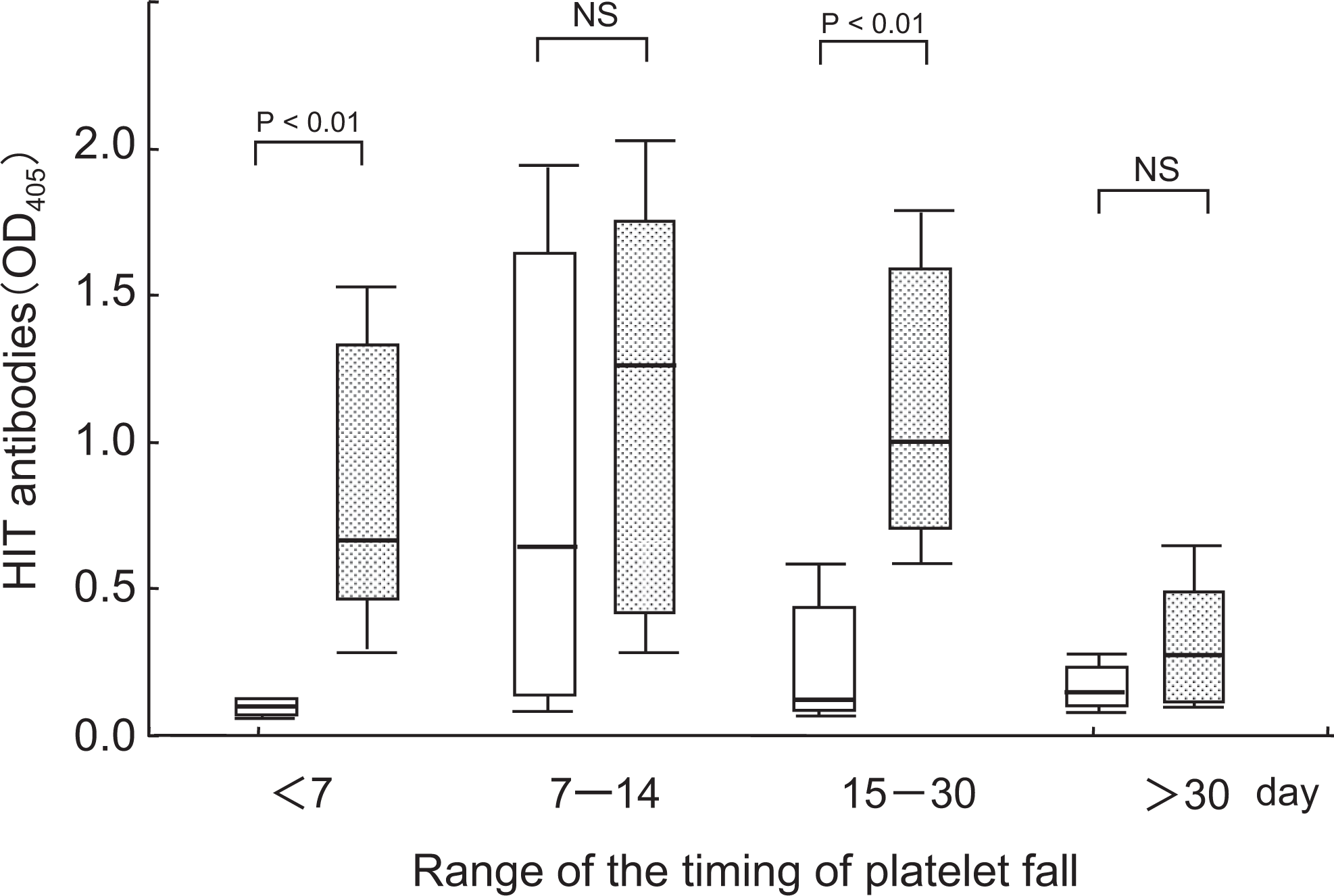
Timing of the platelet count fall in relation to HIT antibody titers between the HD thrombus and non-HD thrombus groups in 78 patients suspected with HIT on hemodialysis. □ indicates HD thrombus group; □, non-HD thrombus group; HIT, heparin-induced thrombocytopenia. *P < .05, box and 25th to 75th percentile whisker plots.
Concerning the involvement of HIT antibody production in HD patients, the sensitivity, specificity, and positive and negative predictive values were calculated; patients were grouped based on the presence or absence of the 3 clinical factors (a fall in the platelet count, a fall occurring on days 7 to 30, and the presence of HD-related thrombus) versus the results of ELISA.
Although a 2-factor combination of 1 out of the 3 clinical factors and a positive ELISA did not play an important role in the diagnosis of HIT, a 3-factor combination of 2 clinical factors—a platelet count of ≤150 × 10 9 /L or a fall of ≥30%, and the presence of an HD-related thrombus, and the addition of 1 laboratory factor of a positive ELISA—improved the indexes. Moreover, a 4-factor combination, when adding a fall timing on days 7 to 30 to the 3-factor combination and ELISA positivity, reached diagnostic significance in HD patients with suspected HIT. Thus, the 4-factor combination indicated “HIT most likely” in HD patients. The findings were supported by the evidence of a high-frequency seroconversion of SRA in the 4-factor combination of 92.3% (Table 2 ).
Two or 3 Clinical Factorsa Versus ELISA for HIT Antibodies in 78 HD Patientsb
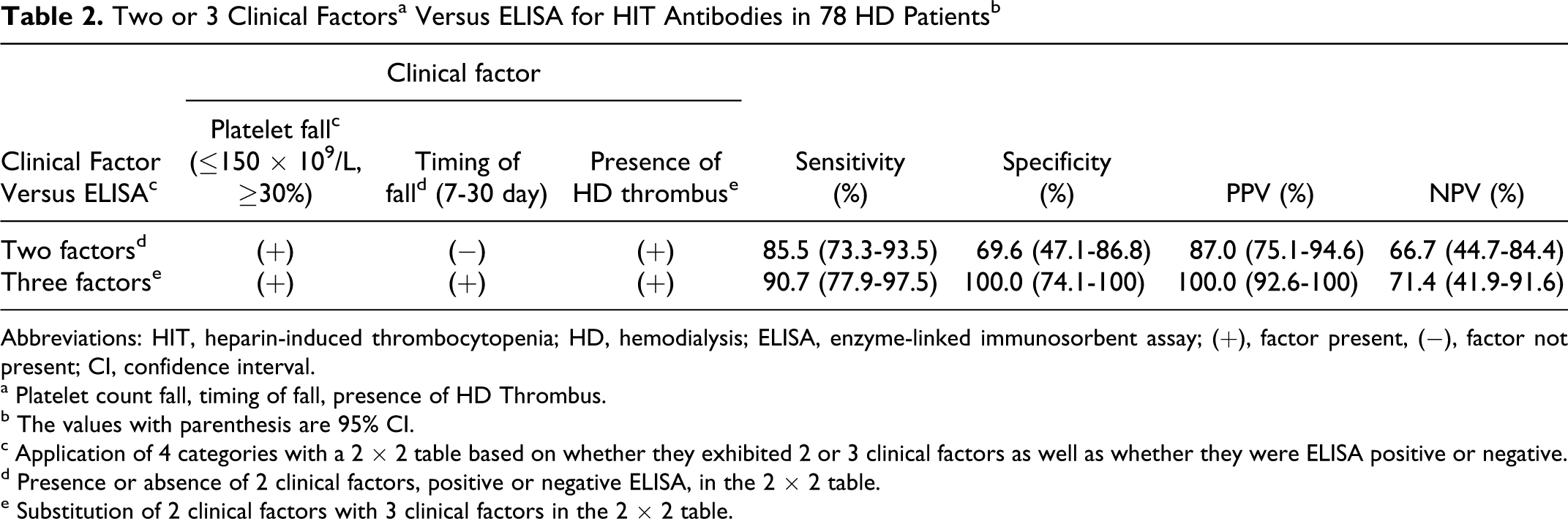
Abbreviations: HIT, heparin-induced thrombocytopenia; HD, hemodialysis; ELISA, enzyme-linked immunosorbent assay; (+), factor present, (−), factor not present; CI, confidence interval.
a Platelet count fall, timing of fall, presence of HD Thrombus.
b The values with parenthesis are 95% CI.
c Application of 4 categories with a 2 × 2 table based on whether they exhibited 2 or 3 clinical factors as well as whether they were ELISA positive or negative.
d Presence or absence of 2 clinical factors, positive or negative ELISA, in the 2 × 2 table.
e Substitution of 2 clinical factors with 3 clinical factors in the 2 × 2 table.
In the HD-related thrombus group, the seroconversion rate of the 3-factor combination (lacking reasonable timing) was 75%. In the nonthrombus group, a 3-factor combination (absence of HD thrombus) was at a rate of 71.4%. An approximate proportion of SRA seroconversion was found in the 3-factor combination between both the groups. A total of 15 patients with the 3-factor combination were classified as HIT likely because of serologic confirmation in 11 (73.3%) of the fifteen patients. In contrast, a 4-factor combination (suitable platelet fall, reasonable timing, and presence of HD thrombus) coupled with a negative ELISA was classified as HIT, unlikely owing to no positive SRA.
Consequently, the 4-factor combination was assigned as “HIT most likely” because HIT is most likely due to a high positive rate of SRA. The 3-factor combination was “HIT is likely” due to a moderate rate of seroconversion of SRA. Negative ELISA despite the presence of the 3-factor combination was adapted as “HIT is unlikely” (Table 3 ).
Evaluation of Patients With 3 Clinical Factors and ELISA
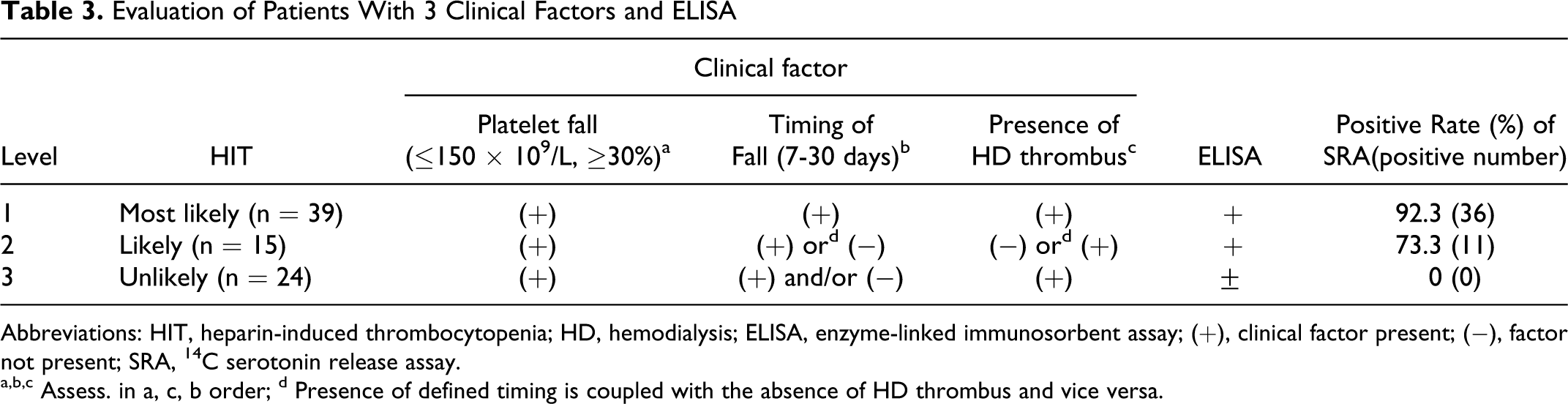
Abbreviations: HIT, heparin-induced thrombocytopenia; HD, hemodialysis; ELISA, enzyme-linked immunosorbent assay; (+), clinical factor present; (−), factor not present; SRA, 14 C serotonin release assay.
a,b,c Assess. in a, c, b order; d Presence of defined timing is coupled with the absence of HD thrombus and vice versa.
Discussion
As unexpected occlusive complications involving the circuit lead to the discontinuation of dialysis and are sometimes life-threatening, the study determined whether clotting in the extracorporeal circuit and thrombotic occlusion in AVF could be characterized as thrombotic complications in HD-HIT patients. A strong association between the formation of a thrombus in AVF and the titer of HIT antibodies was noted, 7 while no relation between AVF thrombosis and HIT antibody positivity has been reported.8–10 Although AVF thrombosis can occur in non-HIT patients due to repeated puncture and careless compression, AVF thrombosis in HIT is suggested when thrombocytopenia occurs in combination with circuit clotting. In the present study, 7 (53.8%) of 13 patients with AVF thrombus were confirmed to have HIT using a functional assay, and the remaining 6 patients did not show a specific episode of HIT. The HD-HIT is not supported by the occurrence of AVF thrombus without a serological confirmation.
In a regular HD session, heparin is continually infused for 4 to 6 hours, then it is stopped until the next session 2 or 3 days later. Thus, the median of the nadir in the platelet count was delayed to day 14 (max: day 72, min: day 2) due to the intermittent use of heparin. The appropriate timing of the fall was estimated at days 7 to 30 for HD-HIT. Compared to the timing (days 5-10) in the 4 Ts pretest scoring system for HIT, 11 the timing in the case of intermittent heparin therapy exhibited a wider range and late emergence. It is suggested that thrombocytopenia caused by HIT antibodies may improve to some extent during the nonheparin days. Similarly, in 28 patients with HIT on chronic dialysis, the mean onset of HIT was day 61, and only 5 patients (17.8%) developed HIT on days 5 to 10, corresponding to the 4 Ts pretest criteria. 12
Unexpected clotting in the extracorporeal circuit may be a sign of HIT onset in HD patients, because circuit clotting during HD and/or AVF thrombosis in association with thrombocytopenia was noted at a relatively high frequency in 55 (70.5%) of the 78 patients suspected with HIT. If clotting occurs on days 7 to 30, heparin therapy should be suspended and an immune assay for PF4/heparin complex antibodies be performed. Positivity for HIT antibodies in the presence of clotting and/or AVF thrombosis resulted in an increased likelihood of HIT. Additionally, the OD of ELISA was significantly higher in the thrombus than in nonthrombus group. As a high titer of HIT antibodies reflects higher thrombin generation through a greater induction of microparticles via the immunomediated activation of platelets by anti-PF4/heparin antibodies, HIT-induced pathogenic production could be involved in the formation of thrombi in the circuit.13–15
In the study, a combination of the 2 clinical factors (an appropriate drop in the platelet count and HD-HIT-related thrombus) was not useful in identifying HIT. Additionally, the combination of 3 clinical factors, adding the timing of the fall, was potentially effective for the diagnosis of HIT. Third, a 4-factor combination through the addition of a positive ELISA can improve the accuracy of HIT diagnosis, and the usefulness of the 4-factor combination was supported by the results of high-frequency platelet-activating seroconversion. The 4-factor combination was capable of improving the diagnostic accuracy of HIT. Therefore, a HD patient with a 4-factor combination may be predicted to be the most likely to have HIT.
Comparable frequencies of seroconversion were found in each 3-factor combination derived from the thrombus and nonthrombus groups. Thus, the 3-factor combination from 2 groups was thought to be HIT likely. Another 3-factor combination (suitable platelet fall, defined timing, and absence of HD thrombus, or suitable platelet fall, nonfitted timing, and presence of HD thrombus) associated with negative ELISA was decided as HIT unlikely due to no positive SRA.
In conclusion, a precise approach to HIT diagnosis can be introduced using a combination of the HIT-related platelet factors and a positive ELISA in patients suspected with HIT. The appearance of clots in the dialyzer and circuit with an unexpected fall in the platelet count on days 7 to 30 may be a practical indicator of HIT in HD patients undergoing adequate anticoagulation with heparin.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.