
Abstract
Objective:
Neutrophil–lymphocyte ratio (NLR) has been associated with poor outcomes in patients with cardiovascular diseases. We aimed to compare NLRs among patients with nonvalvular atrial fibrillation (AF) with or without left atrial (LA) thrombus.
Methods:
A total of 309 (70.1 ± 9.8 years, 49% male) patients with nonvalvular AF have undergone transoesophageal echocardiography (TEE) to assess the presence of LA thrombus. Baseline NLR was measured by dividing neutrophil count to lymphocyte count.
Results:
Left atrial thrombus was detected in 32 (10.3%) of 309 patients. Mean NLR (2.2 ± 1.0 vs 2.7 ± 1.1, P = .026) was significantly higher among patients with LA thrombus compared to patients without LA thrombus. On multivariate analysis, NLR (odds ratio 1.59, 95% confidence interval 0.87-4.18; P < .02) was an independent risk factor for the presence of LA thrombus in patients with nonvalvular AF.
Conclusion:
Neutrophil–lymphocyte ratio, an emerging marker of inflammation, was independently associated with the presence of LA thrombus in patients with nonvalvular AF.
Introduction
Atrial fibrillation (AF) is the most common cardiac arrhythmia, especially in elderly population. Although its prevalence is lower than 0.5% in the fifth decade, it rises up to 5% to 15% in the eighth decade. 1 Despite novel anticoagulants or antiarrhythmic drugs, and new treatment concepts, it is still associated with increased mortality and morbidity. 2 A strong relationship between AF and thromboembolic events has been exactly defined. Up to 15% of the ischemic strokes are developed due to AF. 3
Currently, prevention of thromboembolic events is the main target for the management of AF. Therefore, various scoring systems including clinical features and comorbidities have been defined to identify patients with AF and at risk of thromboembolic complications. 4 Some imaging modalities to visualize the left atrium (LA) and the left atrial appendix (LAA), such as transthoracic and transesophageal echocardiography and so on, have been developed to image the actual or potential source of emboli. However, we have not yet had any definitive, powerful, and noninvasive tool to predict patients with increased risk of thromboembolic events due to AF.
Stasis due to loss of atrial contraction and chamber dilation are not the only pathophysiological determinant of spontaneous echo contrast (SEC) and thrombus in LA. Various factors such as hypercoagulability, inflammation, gender, so on are among the significant factors that increase the propensity to thrombosis in AF. 5 Thrombus in LA may be a consequence of a vicious cycle including thrombotic state, activation of acute phase response, inflammatory state, and raised levels of various inflammatory markers. 6,7
Neutrophil–lymphocyte ratio (NLR) is an easy and reproducible parameter derived from complete blood count (CBC) at bedside or emergency services during acute or chronic clinical scene. 8,9 It is a prognostic factor for poorer outcomes for cardiovascular diseases. 10 In a few studies, it was demonstrated to be associated with the presence of a thromboembolic stroke in nonvalvular AF. However, the role of NLR in predicting the presence of thrombosis which was the most important determining and preceding thromboembolic stroke in patients with nonvalvular AF has not been exactly evaluated in any study. In this study, we objectively evaluated whether NLR could significantly predict the presence of thrombus in LA, which was documented with transesophageal echocardiography (TEE) in patients with nonvalvular AF.
Materials and Methods
Study Population
A total of 878 consecutive TEE examinations performed at GATA Haydarpasa Training and Research Hospital between January 2009 and September 2012 were reviewed. Of these cases, 309 patients with nonvalvular AF (164 women, 53%) who had been performed TEE-guided direct current cardioversion were included. Medical data and archive of patients were analyzed and recorded in detail. The study population was divided into 2 groups according to the presence of thrombus in the LA. These patients had concomitantly any of the following comorbidities such as chronic kidney disease, malignancy, connective tissue diseases, prosthesis valve or native valvular heart diseases, anterior–posterior diameter of LA greater than 4 cm, chronic systemic disease, recent acute infectious or inflammatory disease, high body temperature >38°C, and white blood cell (WBC) count >12.000 cells/μL or <4.000 cells/μL were excluded from the study. Laboratory parameters of complete blood count (CBC), examined same day, including number of white blood cell, erythrocyte, and percentage of neutrophil, lymphocyte, monocyte, and so on were derived from the medical recordings (Abbott Cell-Dyn Sapphire, Chicago, IL, USA). The NLR was calculated based on the results of CBC obtained just as or before the TEE procedure.
Transesophageal Echocardiography
Transesophageal echocardiography procedure was performed in a standard manner in all patients laid at lateral decubitus position, using the VingMed System Five with a multiplane TEE probe (GE Medical System, Hortan, Norway). The TEE was performed after locally anesthetizing the posterior and lateral walls of pharynx and following the conscious sedation. Written informed consent was obtained from all patients prior to the TEE. The TEE examinations were reviewed by two cardiologists, and multiple views were obtained. A thrombus was defined as an echodense mass with a uniform tissue different than that of the LA endocardial wall. 11
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation. Categorical variables were expressed as percentages. For calculation of correlations, Spearman correlation coefficient was used. Multivariate logistic regression analysis was used for the evaluation of the relations of parameters. P values <.05 and.01 were considered significant. Statistical analyses were done using SPSS 11.0 for Windows software.
Results
Totally, 309 (70.1 ± 9.8 years, 53% female) patients were enrolled in the study. The LA thrombus was detected in 32 (10.3%, 46.9% female) of 309 patients. The demographics and comorbidities of patients are summarized in Table 1. Two groups are age and sex matched. Hemoglobin, hematocrit, and monocytes were not significantly different among groups, whereas eosinophil was insignificantly higher in patients with thrombus in LA. Neutrophil count (58.9 ± 10.1 vs 64.2 ± 8.3, P = .005) was significantly higher, whereas lymphocyte count (29.5 ± 9.1 vs 26.3 ± 7.6, P = .034) was significantly lower in patients with the presence of thrombus in LA (Table 2). Also, NLR (2.2 ± 1.0 vs 2.7 ± 1.1, P = .026) was significantly increased in those patients (Table 2). Hypertension was present in 93.8% of the patients with LA thrombus, whereas diabetes mellitus (DM), congestive heart failure (CHF), and coronary artery disease (CAD) were equally distributed in patients with thrombus in LA. Unfortunately, 62.5% (n = 20) of the patients with LA thrombus were on antiplatelet therapy (acetylsalicylic acid or clopidogrel), whereas only 37.5% (n = 12) of those patients were on anticoagulant therapy (Table 1). The NLR was significantly higher in patients with LA thrombus (mean = 2.7, median = 2.69, 95% confidence interval [CI] 2.33-3.07) compared to without thrombus (Figure 1). Cutoff value for predictivity of NLR for the presence of LA thrombus was 2.59 (area under the curve = 0.646 [95%CI 0.541-0.752, P = .007]) with sensitivity and specificity of 53% and 69%, respectively. Receiver–operating characteristic curve is depicted in Figure 2.
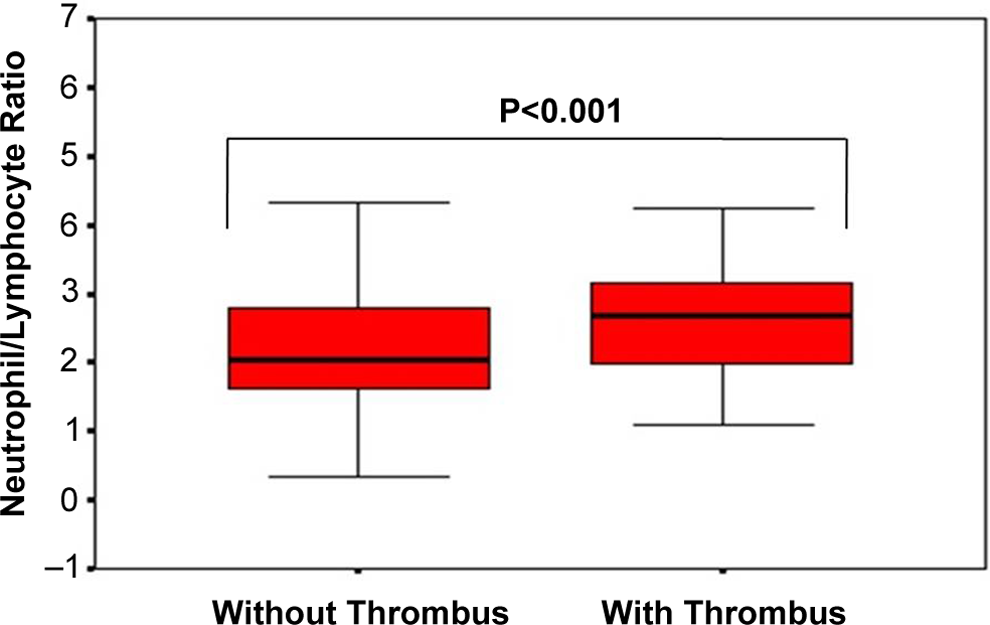
Comparison of ratio of neutrophil to lymphocyte among patients with and without the presence of thrombus.
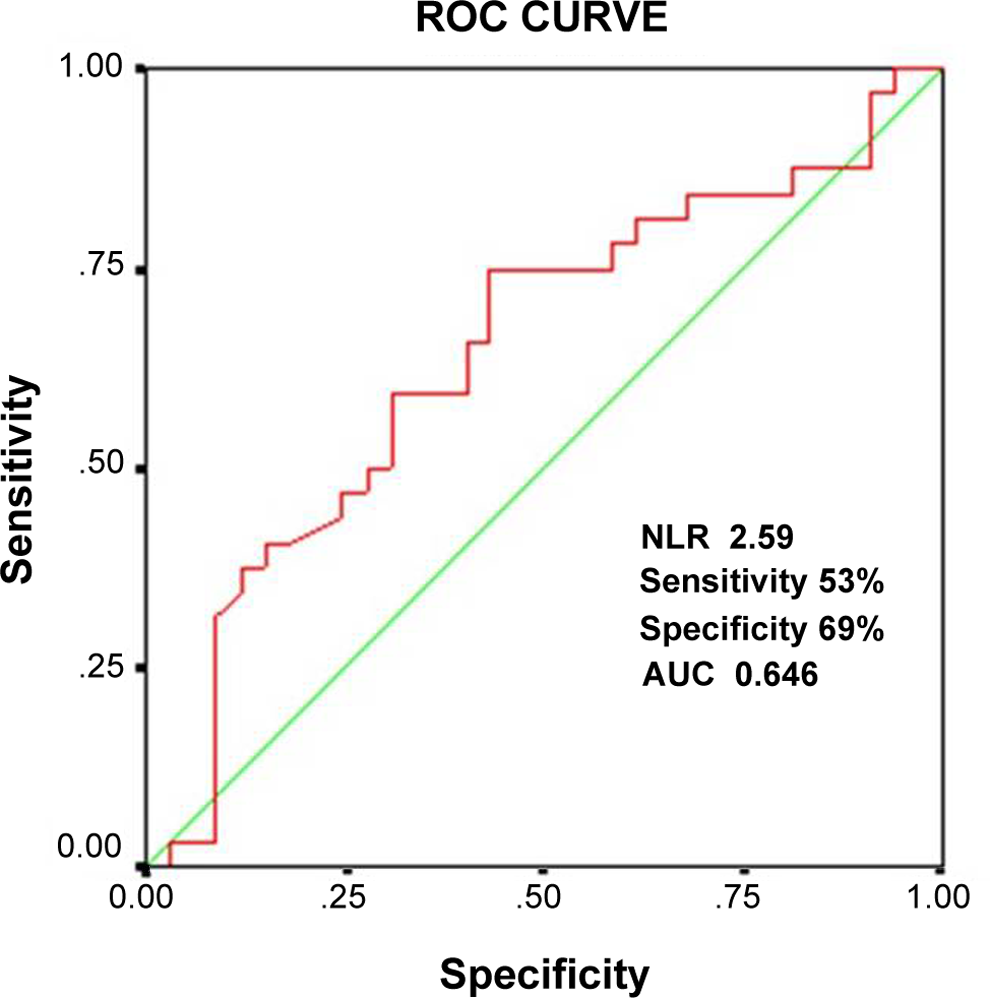
The ROC curve of neutrophil to lymphocyte in prediction of thrombus. ROC, receiver–operating characteristic; NLR, neutrophil to lymphocyte.
Comparison of Demographics and Laboratory Parameters and Distribution of Comorbidities Among Patients With and Without Thrombus.
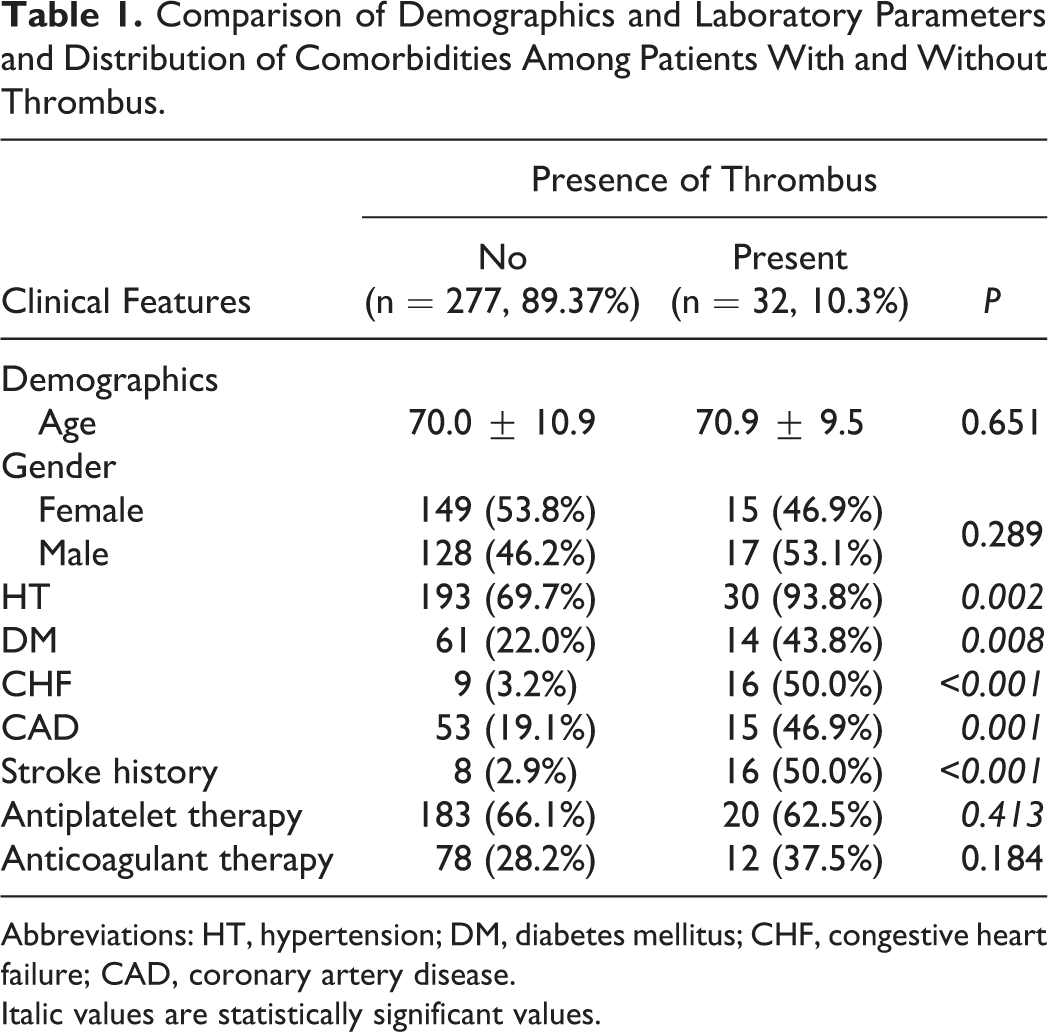
Abbreviations: HT, hypertension; DM, diabetes mellitus; CHF, congestive heart failure; CAD, coronary artery disease. Italic values are statistically significant values.
Comparison of Laboratory Parameters Among Patients With and Without Thrombus.
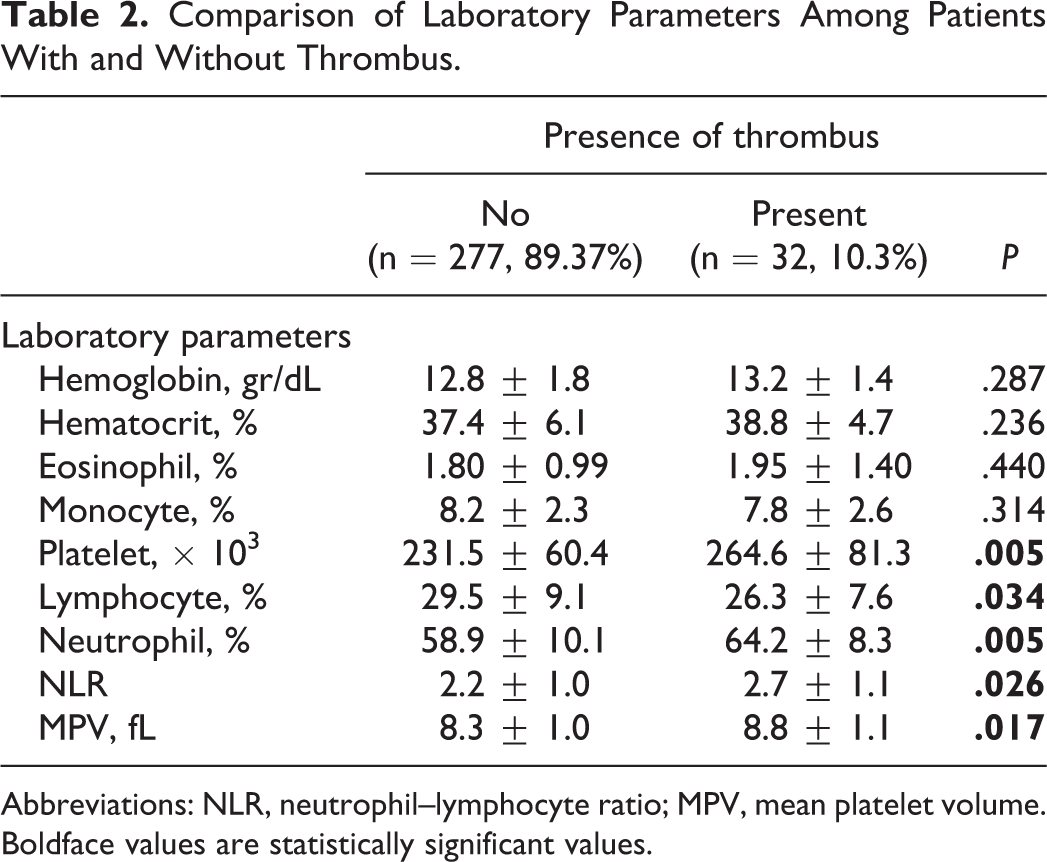
Abbreviations: NLR, neutrophil–lymphocyte ratio; MPV, mean platelet volume. Boldface values are statistically significant values.
From the multiple regression analysis, NLR was positively correlated with age (β = .112, P = .050); and LA thrombus was correlated with NLR (β = .412, P = .005), hypertension (β = .131, P = .003), diabetes (β = .122, P = .008), CHF (β = .600, P ≤.001), peripheral arterial disease (β = .339, P ≤ .001), MPV (β = .136, P = .017), and neutrophil percentage (β =.159, P = .05; Table 3).
Correlation Analysis of NLR, Presence of Thrombus, Demographics, Laboratory Parameters and Comorbidities.
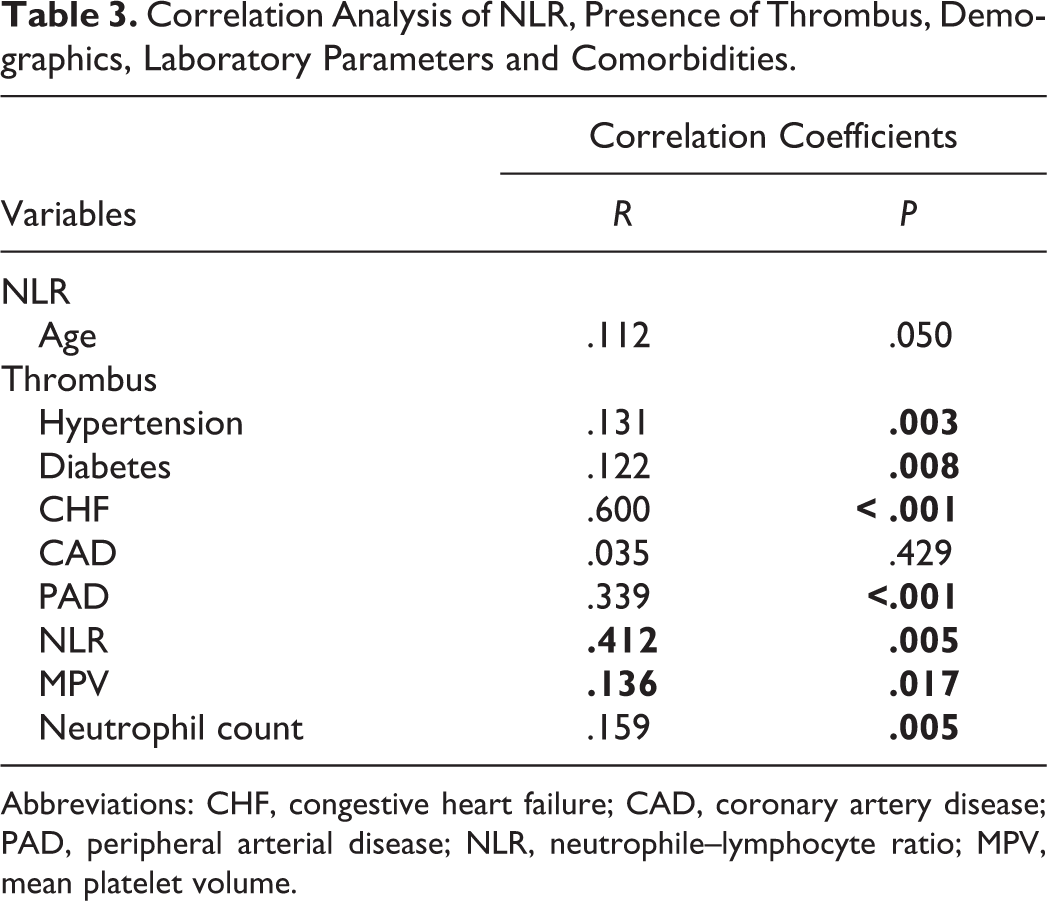
Abbreviations: CHF, congestive heart failure; CAD, coronary artery disease; PAD, peripheral arterial disease; NLR, neutrophile–lymphocyte ratio; MPV, mean platelet volume.
The effects of multiple variables on LA thrombus were analyzed using univariate and multivariate logistic regression analyses. The variables for which the unadjusted P value was <.01 on univariate analysis were identified as potential risk markers for LA thrombus and included in the full model. On multivariate analysis, NLR (odds ratio 1.59, 95% CI 0.87-4.18; P < .02) was an independent risk factor for the presence of LA thrombus in patients with nonvalvular AF.
Discussion
Atrial fibrillation is a cardiac arrhythmia that was associated with a five times increased risk of stroke and remained in the etiology for 20% of all strokes. 12 Presence of thrombus in LA in patients with AF is a significant and independent correlate of thromboembolic cerebrovascular accident rather than left atrial dimensions and functions. 13 So prediction of thrombus in LA gained importance in order to predict the stroke and is necessary for appropriate thromboprophylaxis in patients with AF. 14 Various factors either mechanical or hemorheological abnormalities contribute to propensity to LA thrombus, an echocardiographic evident of potential source for systemic embolism. 15
Inflammatory state that was previously attributed as having a causative role is currently under investigation for the nature and severity of systemic response to various atherosclerotic cardiovascular and cerebrovascular events, and so on. The NLR is a ratio of subtypes of WBC, which is a novel marker of inflammatory state and a predictor for not only long-term mortality in acute coronary syndrome but also overall and disease-specific survival. 16 Although it may represent the level of the systemic inflammatory response within the ongoing challenge of chronic disease, it may demonstrate the severity or potential of an acute challenging event to proceed poorer condition and also the capacity of systemic inflammatory response to overcome it. 9,17 It was also associated with higher inflammatory status in all the patients. 18
In our study, we found that the percentage of neutrophils significantly increased in patients with thrombus in LA. Increased neutrophil percentage compared to lymphocyte could probably be induced by the prolonged life span of activated neutrophils. This also represents an increased inflammatory milieu within blood, which may allow the development of a thromboembolic event.
Neutrophil–lymphocyte ratio was reported to be associated with increased cardiovascular mortality and morbidity. In a meta-analysis, it was found to be a significant predictor of acute decompansation and long-term mortality in patients with CHF. 19 Ertaş et al reported that NLR was associated with thromboembolic stroke in the study which enrolled 126 patients with nonvalvular AF, and they claimed that higher NLR could be caused by an inflammatory process. 20 However, the role of NLR in predicting the presence of thrombus in LA, which was the most important determining and preceding thromboembolic stroke in patients with AF has not been exactly evaluated in any study.
In our study, we documented that NLR was increased naturally due to raised neutrophil count and reduced lymphocytes. Additionally, increased NLR could be associated with the presence of thrombus in LA with a sensitivity and specificity of 53% and 69%, respectively. Since NLR could easily be derived and also reproducible from the CBC test using peripheral blood specimen, it can used in certain clinical circumstances that could potentially be associated with AF and thromboembolic events such as stroke, systemic embolus, originated from intracardiac thrombus. The NLR higher than a cutoff value determined previously may indicate the presence of thrombus and a potential for a stroke without performing any TEE and/or transthoracic echocardiography.
Kaya et al similarly demonstrated that increased C-reactive protein (CRP) and NLR were associated with SEC in patients with AF and mitral stenosis. 6 Our study is clinically significant for the documentation of the relationship of NLR with the presence of thrombus in LA in patients with nonvalvular AF. In our study we also found that thrombus was positively correlated with hypertension, diabetes, CHF, peripheral arterial disease, and also importantly with NLR.
Also, we observed that thrombus was present in 62% of the patients with AF despite the antiplatelet therapy with acetylsalicylic acid or clopidogrel. It was documented that ineffectiveness of aspirin/clopidogrel and the antiplatelet resistance resulted in hypercoagulability and thromboembolic events associated with inflammatory states. 21 It was already shown that aspirin was ineffective in an embolic stroke originated from the cardiac chambers but not in a thrombotic stroke developed on an atherosclerotic plaque or narrowed lumen. 22 Thus, increased neutrophil count and higher NLR could be an evident for the ineffectiveness of antiplatelets in the presence of thrombus and could guide the physician and be a rationale for the earlier initiation of oral anticoagulants in nonvalvular AF.
Coexistence of hypertension in 93.8% of those patients with thrombus in LA is a significant finding that could highlight the reason why hypertension is one of the most important comorbidities in the etiology of thromboembolic events and strokes. We also found that NLR was significantly higher in patients with hypertension compared to ones without hypertension. It was documented that hypertension was the predominating cardiovascular risk factor among the patients with an ischemic stroke. 23 Although the presence of other important comorbidities such as CHF, CAD, and DM was significantly higher in patients with thrombus, prevalence of hypertension in patients with thrombus was remarkably higher compared to others in our study group. In correlation analysis of variables, thrombus was positively correlated with the presence of hypertension, diabetes, peripheral arterial disease, but not CAD (Table 2). The NLR may guide the practitioners and also neurologists, cardiologists, and family physicians in the decision of initiating any anticoagulant therapy in patients with AF with a lower CHADS (Congestive heart failure, Hypertension, Age >75 years, Diabetes, previous Stroke) score. The TEE could be effectively used in stratification of patients with nonvalvular AF by imaging left atrial abnormalities preceding thromboembolic events independent of the presence of low-intermediate risk (CHADS score 0-1) and may guide the anticoagulation therapy. 24 However, a performer of TEE and TEE equipment are not widely available and not easily applicable in many circumstances and health services. So NLR may aid the physician to decide the initiation and continuation of anticoagulant therapy in patients with nonvalvular AF.
Efforts have already been made to augment the predictive role of CHADS2 by inserting new parameters such as glomerular filtration rate <60 mL/min derived from Modification of Diet in Renal Disease formula and so on. 25 Thus, NLR could be a novel parameter with a potential to enhance the predictivity of CHADS2 or CHA2DS2-VASc (Vascular disease, Age, Female gender) scores. Also, we demonstrated that thrombus was still present in patients taking antiplatelet therapy, and higher NLR was also observed in those patients. Thus, higher NLR values in patients with AF and taking antiplatelet therapy may indicate that the choice of anticoagulant therapy would be better for those types of patients. Additionally, higher NLR may guide the cardiologist in postponing the electrical cardioversion of patients with AF and taking anticoagulant therapy after a 3-week period if TEE is not available or the patient is not willing, since higher NLR may have been indicating the presence of thrombus and may prevent unnecessary or inefficacious performing of TEE.
Study Limitations
One of the major limitations of our study is that it was a single-center, retrospectively designed study. The number of patients enrolled was relatively small. Although recorded data about the presence of LA thrombus was evaluated and diagnosed by an experienced cardiologist by means of TEE, data about the LA volume, flow velocities at LA appendices, and spontaneous echo contrast, which may be the determining factors for LA thrombus were not available for all patients. Additionally, inflammatory markers such as CRP or highly sensitive CRP could not be included in the analysis of data due to retrospective design of the study. Finally, since the exact definition of AF such as acute, paroxysmal, persistent, permanent, or long standing and also the duration of anticoagulation therapy are associated with thrombus in LA, unavailability of these parameters was another important limitation of our study.
Conclusion
In conclusion, inflammation is critically important in pathophysiology and also clinical outcomes of AF. The NLR is a widely available, easily derived, and reproducible marker of inflammation. In patients with nonvalvular AF, NLR is associated with the presence of thrombus within LA, which precedes a stroke or thromboembolic event. Thus, it may predict the potential risk of any subsequent thromboembolism. Prospective studies in large study populations may clarify the exact predictive role of that parameter in daily clinical practice at every stage of health services.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.