
Abstract
Atrial fibrillation (AF) not only is an independent risk factor for death but also confers significant risk of morbidity from stroke associated with left atrial thrombus. The association of interleukin 6 (IL-6) polymorphism with thrombus in AF has not been investigated before. We carried out a case–control study in Han Chinese. The IL-6 −634C/G genotypes of 31 patients with thrombus and 45 patients without thrombus were detected by polymerase chain reaction and restriction fragment length polymorphism. The frequencies of the IL-6 genotypes (CC, CG, and GG) were 29.03%, 54.54%, and 16.13% for the patients with thrombus, and 55.56%, 40.00%, and 4.44% for the patients without thrombus, respectively (P = .0391). Compared with the CC genotype, the G allele carriers (CG + GG) had a 2.79-fold increased risk of thrombus or severe spontaneous echocontrast (SEC). These results suggest that IL-6 −634C/G polymorphism is associated with thrombus and severe SEC, and the G allele is an independent risk for thrombus and severe SEC in Han Chinese patients with AF.
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia seen in clinical practice, affecting 1% to 2% of the general population. 1 –4 The prevalence of AF is strongly age dependent, affecting approximately 0.5% of persons aged 40 to 50 years and 5% to 15% of individuals at 80 years. The AF not only is an independent risk factor for death but also confers significant risk of morbidity from stroke associated with cardiogenic thromboembolism developed within the left atria (LA) appendage. 5,6 Compared to healthy population, nonvalvular AF has a 5-fold increased risk of ischemic stroke, and 1 in 5 of all strokes is attributed to this arrhythmia. 3
Interleukin 6 (IL-6) is a pleiotropic cytokine of 23.7 kDa secreted by many cells of the immune system, cardiovascular components, and adipose tissue, functions as a mediator of inflammatory response, and has both proinflammatory and anti-inflammatory properties. 7 –9 The potential role of IL-6 in thrombosis risk in patients with AF is currently under investigation. In a small pilot study, Conway et al 10 first showed that elevated plasma IL-6 concentration was an independent predictor of stroke or death among a cohort of 77 high-risk patients with AF. Similar findings have been reported by Roldan et al, 11 which showed that IL-6 levels were related to low-, moderate-, and high-risk stratification for thromboembolism in patients with AF, with the highest IL-6 levels among the high-risk group.
Circulating levels of IL-6 differ greatly between individuals. 12 This difference is due to both genetic and environmental influences. 13 The human IL-6 gene is located at chromosome 7p21 and contains 5 exons; 3 single-nucleotide polymorphisms in the IL-6 promoter region (−597G/A; −634C/G, and −174G/C) have been reported to influence IL-6 transcription, and −174G/C is reported to bein tight linkage disequilibrium with −597G/A. 14,15 However, the –174C allele was extremely rare and the –634C allele was common in eastern Asian populations, 9,16 –19 whereas in Caucasians the –174C allele was relatively frequent and the –634C allele was less frequent. 20 –22
Left atrial spontaneous echocontrast (SEC), a phenomenon of slow flow in the LA, has been correlated with increased risk of ischemic stroke and thrombus formation. 10 To date, the association of IL-6 polymorphism with LA thrombus formation and SEC has not been investigated before. We carried out a case–control study of the IL-6 −634C/G polymorphism to evaluate its putative association with LA thrombus in Han Chinese patients with AF.
Participants and Methods
Participants
A total of 76 patients with nonvalvular AF underwent transesophageal echocardiography examination (TEE) were enrolled at 6 hospitals (Xinghua People’s Hospital, Affiliated Hospital of Nantong University, Ningxia People’s Hospital, Fourth People’s Hospital of Wuxi, People’s Hospital of Wuxi, and Shanghai Chest Hospital). These patients were assessed from January 2010 to December 2011 in order to detect LA thrombus before planned cardioversion. Cross-sectional and observational study was designed. The patients were divided into 2 groups according to the presence or absence of thrombus in the LA. Patients with LA thrombus were selected as the study group. This group consisted of 31 patients (20 men and 11 women, mean age 56.31 ± 11.25). Patients without LA thrombus on TEE during the same assessment period were selected as the control group. This group consisted of 45 patients (28 men and 17 women, mean age 55.18 ± 10.53). All study participants were unrelated and were Han Chinese. Details of medical history were obtained from all participants using a standardized questionnaire, together with information of drug intake and cigarette smoking. Blood pressure, height, weight, and waistline were measured by trained physicians or nurses according to standardized protocols. Participants with rheumatic valvular heart disease, severe cardiac failure, congenital heart disease, larger LA (>5.5 cm), or receiving anticoagulant drugs were excluded. The study was approved by the local ethics committee, and written informed consent was obtained from all participants.
Transesophageal Echocardiography
A standardized TEE was performed in all patients by experienced cardiologists. 23 A thrombus was diagnosed when there was a clearly defined echodense intracavitary mass not due to the pectinate muscles of the LA appendage. 24 Severity of the SEC was assessed according to the following criteria: 25 mild was defined as minimal echogenicity located in the LA appendage or sparsely distributed in the main cavity of the LA, which was possible to detect only transiently during the cardiac cycle but imperceptible at operating gain settings for 2-dimensional echocardiographic analysis. Moderate SEC was defined as a dense, swirling pattern in the LA appendage, generally associated with somewhat lesser intensity in the main cavity, which may fluctuate in intensity but detectable constantly through the cardiac cycle. Severe SEC was defined as an intense, echodensity, and a very slow swirling pattern in the LA appendage, usually with similar density in the main cavity.
Biochemical Analysis
Venous blood samples were obtained after at least a 10-hour overnight fast and then centrifuged at 2500 rpm for 30 minutes at 4°C and immediately stored at −80°C until analysis. Measurement of total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, and triglycerides was performed as described previously. 26
Determination of Genotypes
Genomic DNA was extracted from peripheral blood leukocytes by the salting out method with minimal modifications. Determination of IL-6 −634C/G genotypes was performed by polymerase chain reaction and restriction fragment length polymorphism as described previously. 9
Statistical Analyses
All continuous variables are expressed as mean and standard deviation. Student t test was used to compare continuous variables from 2 groups. Genotypes and alleles frequencies were obtained by direct count. Differences in the distribution of alleles and genotypes between the groups and deviation from Hardy-Weinberg equilibrium were assessed by χ 2 test. All significant tests were 2 tailed and were considered statistically significant at P < .05. SAS software (version 8, SAS Institute, Cary, North Carolina) was used in all statistical analyses.
Results
The clinical characteristics of all participants enrolled in the study are depicted in Table 1. There were no significant differences in gender, age, body mass index (BMI), blood pressure, serum lipid parameters, and the prevalence of type 2 diabetes mellitus, smoking status as well as left ventricular ejection fraction and LA diameter between the study group (patients with thrombus) and the control group (patients without thrombus). Some of the patients had the history of coronary artery disease, ischemic stroke, or transient ischemic attack, but no positive results were found between the 2 groups.
Comparison of Clinical Characteristics Between 2 Groups.a
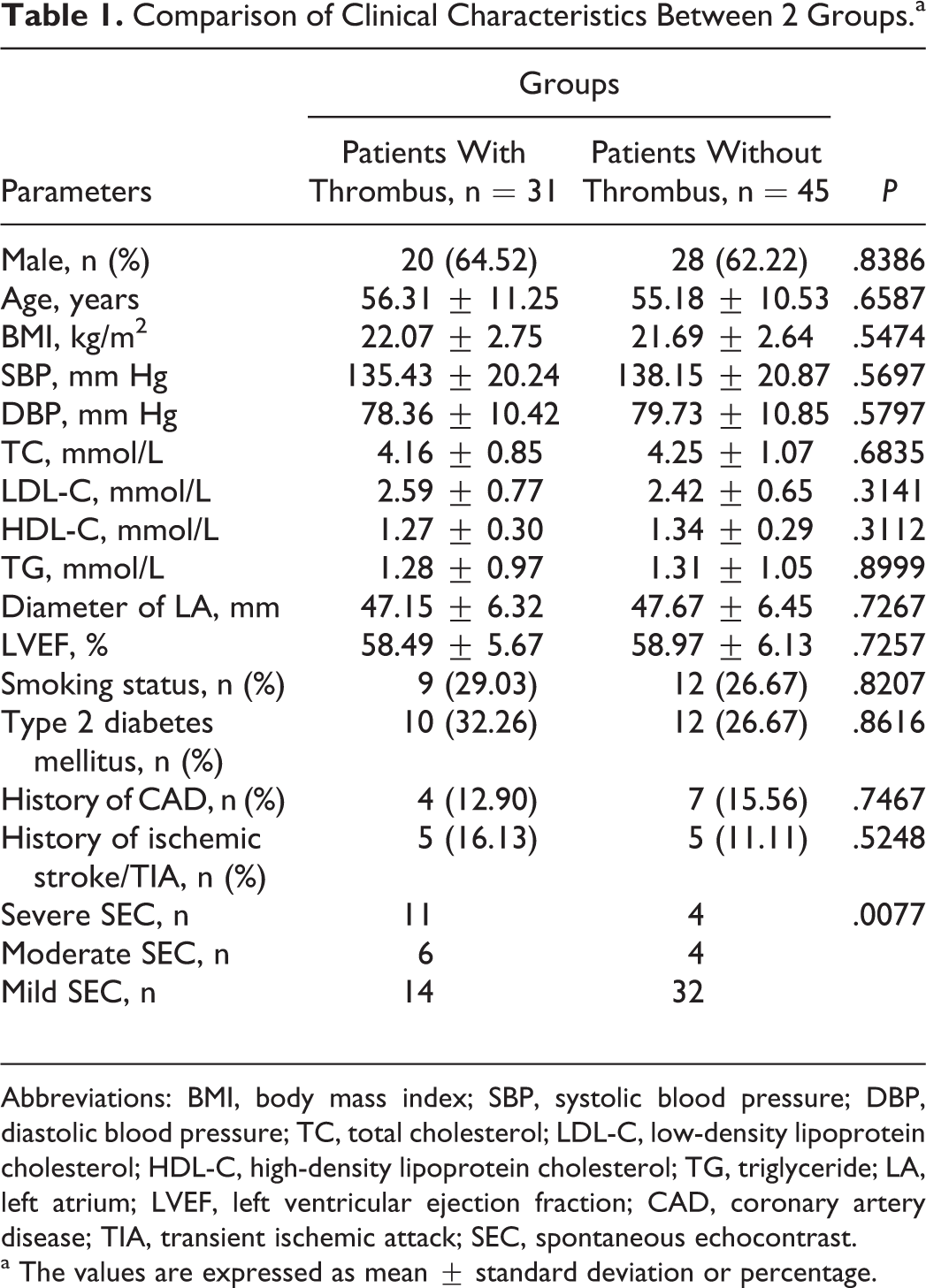
Abbreviations: BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; TC, total cholesterol; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; TG, triglyceride; LA, left atrium; LVEF, left ventricular ejection fraction; CAD, coronary artery disease; TIA, transient ischemic attack; SEC, spontaneous echocontrast.
a The values are expressed as mean ± standard deviation or percentage.
Among the 76 patients with AF, 71 (93.42%) had SEC on TEE. Of all, 15 (19.75%) patients were severe, 10 (13.16%) were moderate, and 46 (60.53%) were mild. Patients with LA thrombus had significantly higher prevalence of SEC compared to those without thrombus.
Table 2 summarizes the distributions of IL-6 −634C/G genotypes and allele frequencies for 2 groups. The genotype frequencies did not deviate significantly from those predicted by the Hardy-Weinberg equation for the patients with thrombus (χ 2 = 0.4124, P = .5207) or patients without thrombus (χ 2 = 0.3092, P = .5782). The frequencies of the IL-6 −634C/G genotypes (CC, CG, and GG) were 29.03%, 54.54%, and 16.13% for the patients with thrombus, and 55.56%, 40.00%, and 4.44% for the patients without thrombus, respectively (P = .0391). The derived allele frequencies for the C and G alleles were 56.45% and 43.55% in the patients with thrombus and 75.56% and 24.44% in the patients without thrombus, respectively (P = .0133).
Genotypes and Alleles Frequencies of IL-6 −634C/G.
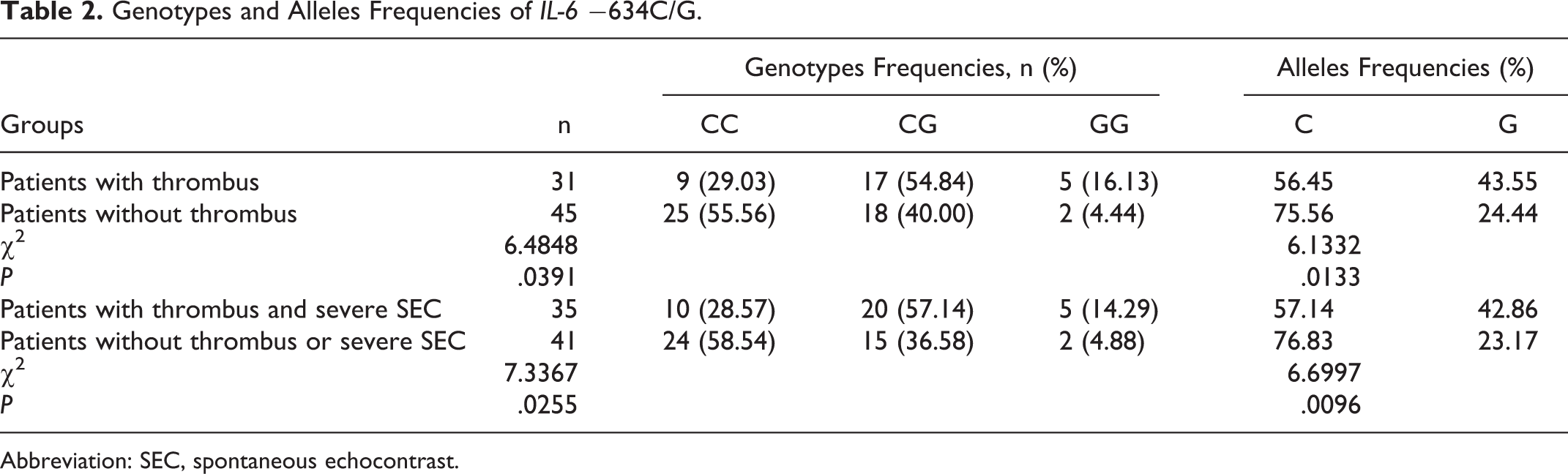
Abbreviation: SEC, spontaneous echocontrast.
Because severe SEC was a predisposition to thrombus formation, the patients with thrombus or severe SEC were pooled into 1 group. These patients also had significantly higher GG (14.29%) and CG (57.14%) genotype frequencies and G allele frequency (42.86%) than those in the patients without thrombus or severe SEC. Compared with the wild type CC, the G allele carriers (CG + GG genotypes) had a 3.53-fold increased risk of thrombus or severe SEC (crude odds ratio [OR] = 3.53, 95% confidence interval [CI] = 1.35-9.23, P = .0114). After being adjusted for gender, age, BMI, blood pressure, serum lipid parameters, smoking status, and prevalence of type 2 diabetes mellitus, the association persisted (adjusted OR = 2.79, 95% CI = 1.09-7.16, P = .0389; seen in Table 3).
Relative Risk of Thrombus or Severe SEC According to IL-6 −634C/G Genotypes.
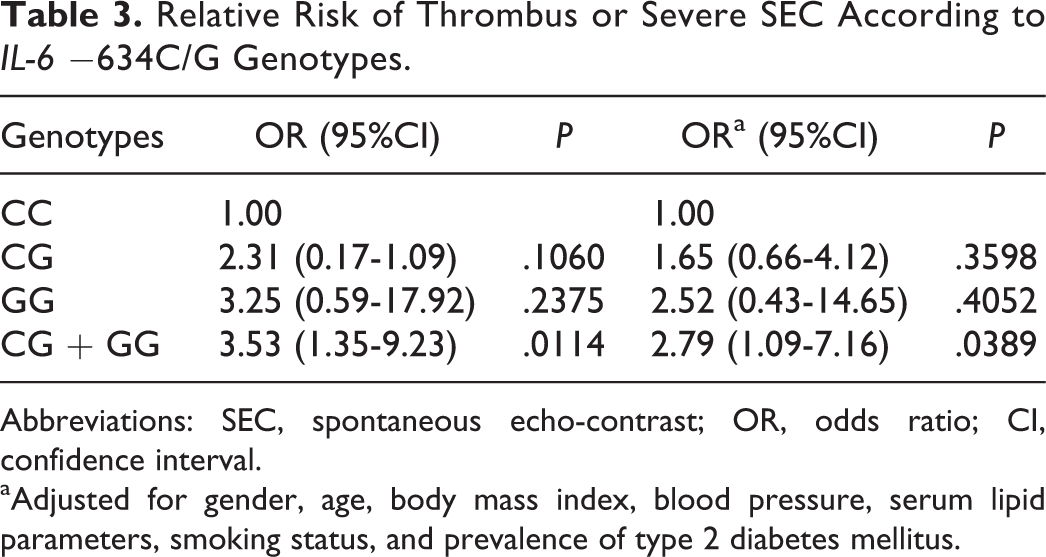
Abbreviations: SEC, spontaneous echo-contrast; OR, odds ratio; CI, confidence interval.
aAdjusted for gender, age, body mass index, blood pressure, serum lipid parameters, smoking status, and prevalence of type 2 diabetes mellitus.
Discussion
To the best of our knowledge, this is the first study to provide evidence that polymorphism of inflammatory cytokine might play an important role in the risk of thrombogenesis in AF. Compared with the wild type CC, the G allele carriers (CG + GG genotypes) had a 2.79-fold increased risk of thrombus or severe SEC.
Recently, several lines of evidence support a strong association between inflammation and the pathogenesis of AF. Inflammatory infiltrates and myocyte necrosis were found in atrial tissue in patients with AF and in animal models of AF. 27 In addition, some studies have shown that levels of inflammatory mediators, such as IL-6 and high-sensitivity C-reactive protein (hs-CRP), were increased in patients with AF and were associated with unsuccessful cardioversion. 28,29 Furthermore, treatment with anti-inflammatory agents, such as statins, in patients with AF was associated with a significant decrease in the risk of arrhythmia recurrence after successful cardioversion. 30,31
The possible association between AF and inflammation might support the potential role of inflammation on prothrombotic state in cardiac chambers during atrial arrhythmia. There is increasingly strong evidence for the presence of hypercoagulable state in AF, even in the absence of underlying heart disease. 3 The abnormal inflammatory state might drive the prothrombotic state in AF, which might contribute to the increased risk of thrombogenesis and, subsequently, thromboembolism. 29 Both CRP and IL-6 could increase tissue factor production from monocytes in vitro. 32 The IL-6 also stimulated platelet production, platelet sensitivity to thrombin, and stimulation of transcription of fibrinogen. 33,34 In addition, inflammatory cytokines were linked to both endothelial activation and damage. 35 Tissue factor and high stroke risk were independent associates of IL-6, whereas fibrinogen and plasma viscosity were independent associates of CRP amounts. 36
Conway et al 10 first confirmed the putative link between inflammation and thromboembolism in AF in a small pilot study, showing that elevated plasma IL-6 concentration was an independent predictor of stroke or death among a cohort of 77 high-risk patients with AF. In the same study, another inflammatory cytokine, CRP was found to be independently associated with dense SEC in the LA, which was a well-recognized independent predictor of stroke and thromboembolism in AF. Then in another study including 104 patients with AF, Thambidorai et al 37 further showed that increased CRP levels were correlated with LA thrombus and severe SEC. In addition, Roldan et al 11 found that IL-6 levels were related to low-, moderate-, and high-risk stratification for thromboembolism in patients with AF, with the highest IL-6 levels among the high-risk group.
Most recently, in a prospective study, Cianfrocca et al 38 demonstrated that LA appendage velocity and CRP were independently associated with the risk of thrombogenesis in AF in a large homogeneous population of patients with persistent AF. These findings, along with the greater incidence of embolic events observed during a mean period of 24 ± 15 months of follow-up in patients with dense SEC again support the hypothesis that blood stasis and inflammation constitute 2 major independent components of thrombogenesis.
Our study has some potential limitations. First, the relatively small sample studied in our report may affect the outcomes. It is difficult to find patients with thrombus and archive screening is needed to increase the number of patient with thrombus. In addition, we intentionally excluded patients receiving anticoagulant therapy, because inclusion of these patients might have led to underestimation of the incidence of thrombus. However, large prospective studies are needed to establish whether the IL-6 −634C/G polymorphism is a risk factor for LA thrombus formation in patients with AF. Second, the absence of the evaluation of serum IL-6 and CRP levels in relation to different genotypes may limit the outcomes. Circulating levels of IL-6 vary widely within populations, 12 and genetic factors are thought to play a major role, along with environmental factors, particularly inflammation. 13 The IL-6, as a principal upstream mediator of the acute-phase proteins, also regulates CRP gene expression. 7,39,40 The association of IL-6 polymorphism with higher serum CRP concentration maybe due to an increase in IL-6 gene transcription and the consequent effects of increasing levels of IL-6 on CRP gene expression. 9 Our previous report 9 along with the studies conducted in Japanese and Koreans 18,41 –45 indicated that IL-6 −634G allele was associated with higher circulating levels of IL-6 and CRP in eastern Asians. However, assessment of serum IL-6 and CRP levels concordant with IL-6 −634C/G polymorphism in patients with AF, especially in patients with AF with LA thrombus, is required in further study. Finally, although all the study participants were Han Chinese population and thus the possibility of ethnicity as a confounding factor could be excluded, the association of the IL-6 −634C>G polymorphism and LA thrombus in AF in other populations remains unknown and needs further study. Accepting the limitations of our present study, we believe that the potential predictive value of IL-6 −634C>G polymorphism and the possible role of inflammation in the pathogenesis of thrombogenesis in AF are areas that deserve further study.
In conclusion, our data support that IL-6 −634C/G polymorphism is associated with LA thrombus and severe SEC and the G allele is an independent risk for thrombus and severe SEC in Han Chinese patients with AF. Given the inherent limitations of case–control studies and the complex nature of genetic susceptibility for chronic degenerative diseases, the prospective and interventional clinical studies with larger sample size are required to be conducted in individual ethnic groups to confirm our observations.
Footnotes
Authors’ Note
Xin-Tao Deng and Min-Hui Jiang should both be considered first authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: grants from the “Summit of the Six Top Talents” Program of Jiangsu Province (2009046), Natural Science Foundation of Ningxia Autonomous region (NZ10168), and Nantong Municipal Commission of Science and Technology (S40015, S2008021).