
Abstract
Background:
In this study, our aim is to examine the role of the neutrophil to lymphocyte ratio (NLR) in the predictions of recurrence under long-term follow-up in patients whose sinus rhythms (SRs) were restored with amiodarone in acute atrial fibrillation (AF).
Methods:
Retrospectively, patients with acute AF, which successfully converted to the SR with amiodarone treatment, were recruited into the study. Patients experiencing the first AF attack were enrolled to the study and followed up for 5 years (median 23 months, 25-75 percentiles 12-24 months). Neutrophil to lymphocyte ratio was computed as absolute neutrophil count divided by lymphocyte count.
Results:
A total of 218 patients were recruited into the study and followed up for 21.6 ± 13.9 months; 87 (40%) patients had ≥1 recurrent AF attack within this period. The follow-up of 131 (60%) patients resulted in persisted SR without any other AF attack. Groups were similar in terms of age and gender. Left atrium (LA) diameter and NLR were increased, and platelet count and lymphocyte count were decreased in patients with AF recurrence in univariate analysis (P < .05 for all). Only LA diameter (for per mm, 1.077 [1.021-1.136], P = .006) and NLR (1.584 [1.197-2.095], P = .001) were independent predictors of AF recurrence in the multivariate analysis.
Conclusion:
Increased NLR is a marker of increased inflammation and may serve as simple, cheap, and readily available predictors of recurrence in the long-term follow-up of patients admitted with acute AF and successfully converted to SR with amiodarone.
Introduction
Atrial fibrillation (AF) is the most frequent sustained arrhythmia found in medical practice and increases stroke rate and mortality. 1 Pharmacological cardioversion is chosen as a less aggressive treatment in cases where patient is hemodynamically stable. In the treatment of AF, a number of antiarrhythmic drugs are used. Amiodarone is the most commonly used agent, restoring sinus rhythm (SR) with a high success rate and without a mortality increase. 2
Many studies have shown increased inflammation associated with AF. 3 Although C-reactive protein (CRP) is the most commonly used indicator of inflammation, it has been recently shown that the neutrophil to lymphocyte ratio (NLR) is also a marker of inflammation in certain states. 4 There are some conflicting data about AF and NLR association. 5 Although NLR is found to be significant in predicting AF recurrence after catheter-based ablation, 6 this is not the case in patients with acute AF, which was electrically converted to SR. 5
This study was aimed at determining the clinical values of NLR on AF recurrence over a long-term period within the setting of acute AF in patients who successfully converted to SR with amiodarone treatment.
Methods
Study Protocol
This study is a retrospective research based on medical records. It covers patients who admitted to the emergency department of Çorum Training and Research Hospital between the years 2006 and 2013 for acute (recent onset, ≤48 hours) AF and who had successfully converted to SR with amiodarone administration. Atrial fibrillation was screened using the International Classification of Diseases, Tenth Revision code (I4.8) from the hospital digital record system. The following patients were excluded from the study: patients who converted to SR naturally; patients converted to SR by direct current (DC) cardioversion or by a drug other than amiodarone; patients whose rhythm went on AF; and patients who have had acute stroke, a documented infection (white blood cell [WBC] count > 12 000/μL or 4000/μL and body temperature ≥38°C], acute coronary syndrome, bone marrow dysplasia, autoimmune or inflammatory diseases, and known malignancy.
A total of 1920 patients admitted to the emergency department and was diagnosed with AF during the study period. Of these patients, 518 had acute AF; 70 of the patients converted by DC cardioversion; 45 of the patients converted by a drug other than amiodarone; and 35 of the patients converted to SR spontaneously. Amiodarone was administered to the rest of the patients but 60 of them did not convert to SR. Therefore, 308 patients were successfully converted to SR by amiodarone administration. In all, 21 of the patients were excluded from the study due to the fact they had increased WBC, higher than the normal values, or had an infectious disease; 18 of them were excluded due to acute coronary syndrome and 2 were excluded due to hematologic malignancy; 49 patients were also excluded due to failure of researchers to access their follow-up records. Eventually, 218 patients (age 64.1 ± 14.6; 92 males) were recruited to the study.
For all patients who were admitted to the emergency department, a 12-lead electrocardiogram (ECG) was obtained and the heart rate, as well as blood pressure, was monitored during the amiodarone treatment and the following 24 hours. Intravenous 300 mg amiodarone in an 100 mL 5% dextrose solution was administered to all participants over 1 hour, then 900 mg of the same in a 500 mL 5% dextrose solution was administered over the next 23 hours as an institutional protocol. Aspirin and a therapeutic dose of subcutaneous enoxaparin (1 mg/kg) were given to all patients on admission. In the case of necessity, metoprolol and digoxin were given as rate-limiting agents. During the hospitalization of the patients, continued ECG monitoring was conducted for AF recurrence and other arrhythmias. Patients’ medical records were searched from index attack to August 2013 for AF recurrence.
Transthoracic echocardiography was performed for each patient during hospitalization. All measurements were performed using a commercially available machine (Vivid 4 or Vivid S5, GE Medical System, Horten, Norway) with a 3.5-MHz transducer. Measurements of the LA and left ventricular systolic and diastolic diameters were conducted with the standard criteria of the parasternal long axis. Left ventricular ejection fraction (EF) was measured by modified Simpson’s method. 7
Blood Sample Analysis
A whole blood count was made from all participants using the antecubital venous blood samples taken upon admission to the emergency department. The blood samples were collected in calcium EDTA tubes. Whole blood counts were evaluated using an auto-analyzer Sysmex XT-1800i Hematology Analyzer (Sysmex Corporation, Kobe, Japan). Neutrophil to lymphocyte ratio was calculated as the ratio of neutrophils to lymphocytes from these results. In addition, other laboratory findings were examined using the digital record systems.
Statistical Analysis
Continuous variables were tested for normal distribution by the Kolmogorov-Smirnov test. Continuous data showed as mean and standard deviation or median. Continuous variables were compared using the Student t test or Mann-Whitney U test between groups. Categorical variables were showed as percentages and compared with the chi-square test. The Pearson test was used in the correlation analysis between parametric variables. Spearman ρ test was used in the correlation analysis of the nonparametric variables. Multivariate logistic regression analysis was performed to determine the independent predictors of AF recurrence. The variables with an unadjusted P < .010 in univariate analysis were adjusted to the full model. There is a significant autocorrelation between NLR and lymphocyte count (r = −.353, P < .001), so lymphocyte did not recruited to the logistic regression analysis. A 2-sided P value < .05 was considered as statistically significant.
Results
In all, 218 patients (age 64.1 ± 14.6; 92 males) were recruited to the study. Patients were followed up for 5 years (median 23 months, 25-75 percentiles 12-24 months). During this period, 131 patients were in SR (group 1) and 87 of the patients had an AF recurrence (group 2). In terms of age, gender, active smoking, arterial hypertension, diabetes mellitus frequency, and AF duration, both groups were similar. Systolic blood pressure, diastolic blood pressure, and heart rate were similar between the groups. In addition, the EFs of the left ventricle were similar between the groups but in group 2, patients had a higher LA diameter when compared to group 1 patients. Groups were also similar for ongoing antiarrhythmic treatments when index attack was seen. Groups were also similar for upstream treatment of AF such as angiotensin-converting-enzyme inhibitors, angiotensin-receptor blockers, and statins. Levels of fasting plasma glucose, potassium, sodium, creatinine, blood urea nitrogen, and total cholesterol were not significantly different between the groups. Otherwise, hemoglobin, hematocrit, WBC, and neutrophil count values were not significantly different, but lymphocyte and PLT counts, and NLR, were significantly higher in group 2 (Figure 1). Demographic and clinical properties of both the groups are shown in Table 1.
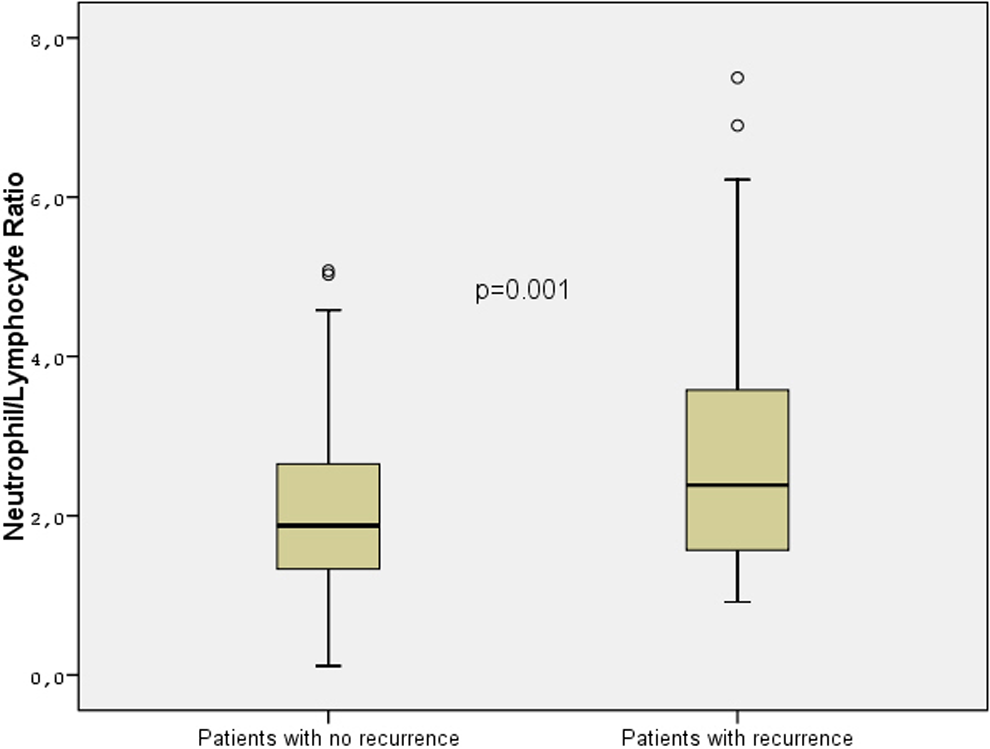
Box plot graphics of neutrophil to lymphocyte ratio values of groups.
Baseline Characteristics of the Groups.a
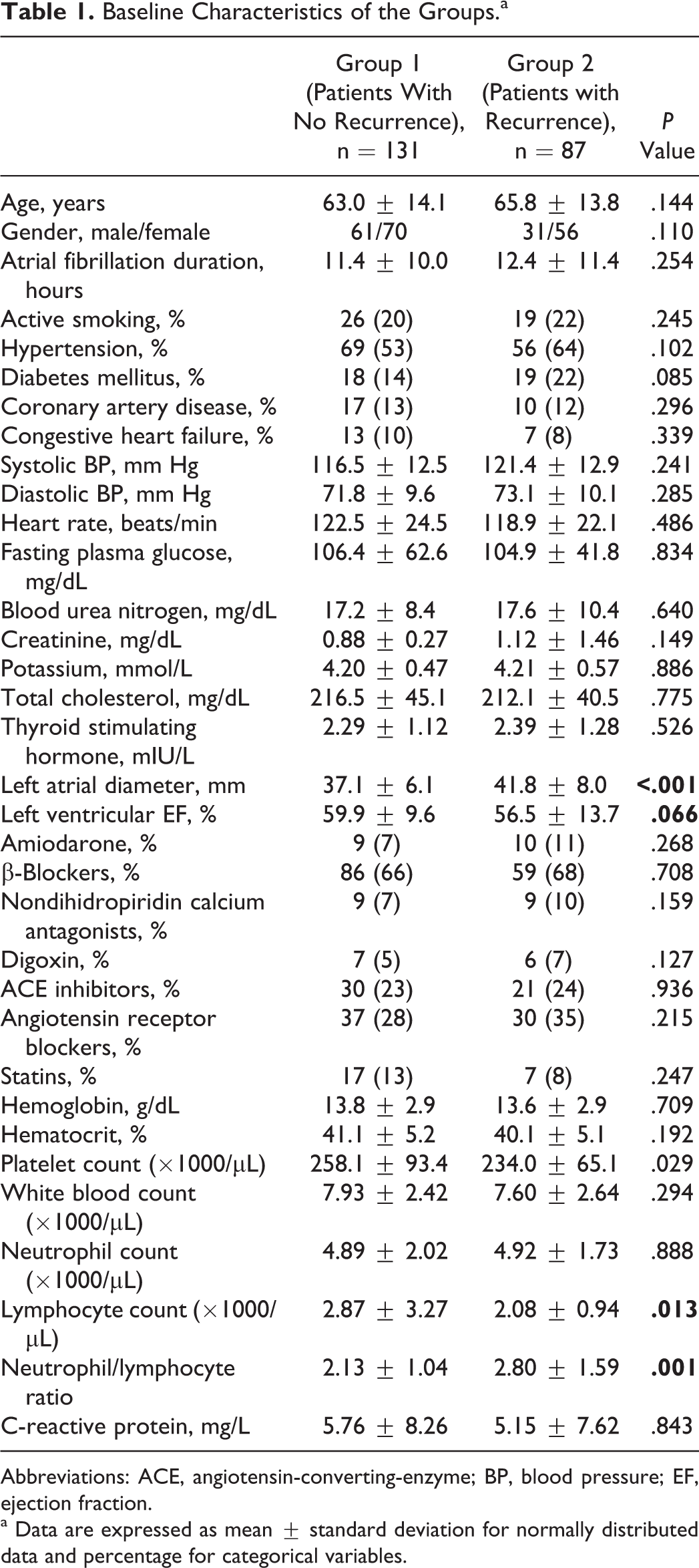
Abbreviations: ACE, angiotensin-converting-enzyme; BP, blood pressure; EF, ejection fraction.
a Data are expressed as mean ± standard deviation for normally distributed data and percentage for categorical variables.
Multivariate logistic regression analysis was performed to evaluate the independent correlates of AF recurrence. The variables with an unadjusted P < .010 in univariate analysis were adjusted to the full model. Multivariate logistic regression analysis was performed, and LA diameter, EF, platelet count, and NLR were included in the analysis. Lymphocyte count was not included in the analysis due to significant autocorrelation with NLR. Furthermore, only the LA diameter (odds ratio [OR] 1.077, 95% confidence interval [CI] 1.021-1.136; P = .006) and NLR (OR 1.584, 95% CI 1.197-2.095; P = .001) were found to be independently correlated with AF recurrence (Table 2).
Independent Predictors of Atrial Fibrillation Recurrence in Logistic Regression Analysis.
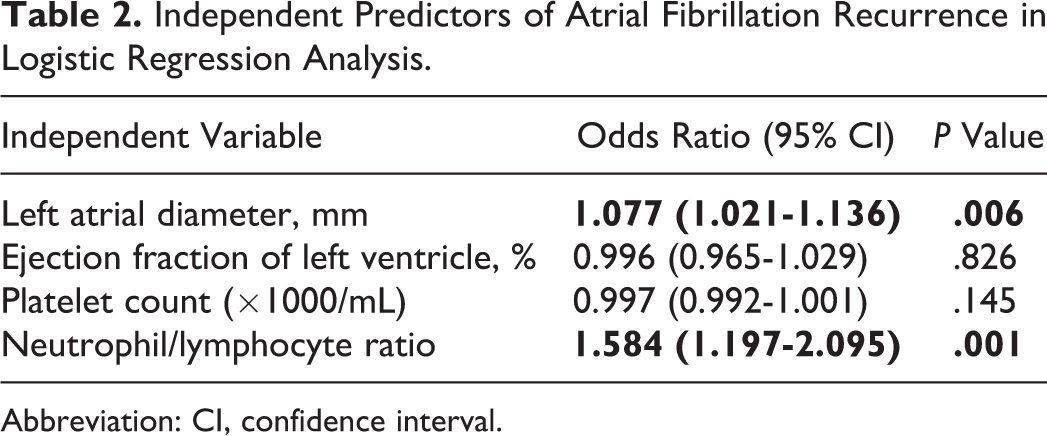
Abbreviation: CI, confidence interval.
Discussion
In this study, it was shown that NLR is the independent predictor of AF recurrence during a long-term period in patients whose SR had been restored with amiodarone. Inflammation plays a role in the etiopathogenesis of many cardiovascular diseases. We discuss about inflammations on AF, 8 as well as on stabile atherosclerotic cardiac diseases and acute coronary syndromes. 9 Inflammatory infiltrations in the atrial tissue biopsy of lone AF 10 are the main evidence of this phenomenon. Also shown is that patients with AF have higher CRP levels than patients with SR in venous samples. 11 –13 In addition, other inflammation markers such as the tumor necrosis factor, interleukin (IL) 2, IL-6, IL-8, and monocyte chemoattractant protein 1 levels are related to AF. 14 There is no definite explanation as to how inflammation induces AF development. Neutrophil accumulation in the atrial tissue may create an arrhythmic substrate by stimulating atrial remodeling with the proinflammatory cytokines. Certain studies reported that a much longer AF period is associated with higher CRP levels, more inflammations, and remodeling. 8,15 Conversely, in other studies, the inflammatory indicators such as CRP and IL-6 levels, are not different, whether the AF is paroxysmal or permanent. 16 In this study, CRP levels were not different in patients with AF recurrence when compared to the patients with SR.
The WBCs, which indicate an inflammatory medium, were also significantly higher in patients with AF 17 than in patients with lone AF. 10 Previous studies have shown that increased pre- and postoperative WBCs are found to be independent predictors of postoperative AF in patients who underwent coronary artery bypass surgery. 18,19 These findings show the relationship between AF and inflammation based on electrical and structural remodeling. 20 Neutrophil to lymphocyte ratio is known to have a strong relation to systemic inflammation 21 and potentially has superior value than that of simple WBC. Neutrophil to lymphocyte ratio with a high neutrophil number indicates inflammation while NLR with a decreased lymphocyte number indicates physiological stress and poor general health and offers detailed information only when compared to leukocyte values. 22,23 Recently, NLR has been investigated widely in different states, and it was found that it is associated with various cardiovascular events. 24,25 For example, it was shown that increased NLR might be a strong predictor of adverse events in patients who had a coronary bypass graft surgery 26 and a percutaneous coronary intervention. 4
Gibson et al showed that pre- and postoperative NLR values are associated with increased risk of AF development after the coronary artery bypass grafting. 19 There are conflicting results about inflammation and AF recurrence after successful cardioversion of AF. 5 Aribas et al reported that increased high-sensitivity CRP (HsCRP) levels predict AF recurrence but NLR is not predictive of AF recurrence after a successful electrical cardioversion in patients with nonvalvuvar AF. 5 Im et al showed that NLR is related to early recurrence after radiofrequency ablation in patients with AF. 27 Canbolat et al found that increased preablation NLR values were associated with AF recurrence during the 19-month follow-up after successful cryoballoon-based AF ablation. 6 The association of NLR with inflammation and also with thrombogenicity was shown in patients with AF by previous studies. 28,29 However, there are no data about the follow-up after pharmacological cardioversion, so our study provides first data in this field. This study suggest that NLR may be useful in predicting AF recurrence during a long-term period after successful pharmacological cardioversion, as well as catheter-based ablation of AF. In this study, LA diameter was also found to be an independent predictor of AF recurrence. This finding is concordant with previous study results. 30 –32
Limitations
Retrospective design is the main limitation of this study. Moreover, this study is based on single-center experiments. In this study, conventional CRP kits were used. If the high-sensitive CRP kits were used, study results might have been stronger. Atrial fibrillation diagnosis in the follow-up was based on chronic AF or documented AF attacks in the controls of the patient. Therefore, silent AF attacks may have been missed due to the fact that ambulatory ECG monitoring was not carried out.
Conclusion
Neutrophil to lymphocyte ratio values were found to be independent predictors of late AF recurrence in patients admitted with acute AF and converted to SR by amiodarone. It may stand as cheap, readily available, and a simple marker in the prediction of AF recurrence during follow-up. However, it is certain that these results should be confirmed by large scale prospective studies.
Footnotes
Acknowledgments
We extend our thanks to Kaan KAYA, MD, Jülide Uzunonat, MD, Füsün İnceer, MD, Ali Elitok, MD, Betül Cengiz, MD, Gökan Bilgili, MD, Osman Karaaslan, MD, Tolga Dogan, MD, Arif Arısoy, MD, and Oguzhan Celik, MD, who worked in the clinic during this period and contributed to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.