
Abstract
Introduction:
The sticky platelet syndrome (SPS) is a common cause of thrombosis. There are no prospective studies concerning treatment.
Objective:
To analyze changes in platelet hyperaggregability of patients with SPS who were given antiplatelet drugs and to assess its association with rethrombosis.
Methods:
A total of 55 patients with a history of thrombosis and SPS phenotype were prospectively studied before and after treatment with aspirin and/or clopidogrel.
Results:
Patients were followed for 1 to 129 months, median 13. Of 55 patients, 40 received aspirin, 13 received aspirin + clopidogrel, and 2 received only clopidogrel. The platelet aggregation response to adenosine diphosphate and epinephrine significantly diminished after treatment, and only 2 patients developed rethrombosis 52 and 129 months after starting therapy, with the freedom from rethrombosis rate of the patients being 96.4% at 129 months.
Conclusion:
Using antiplatelet drugs, the platelet hyperreactivity of patients with the SPS phenotype was reverted; and this translated into a substantial decrease in the rethrombosis rate.
Introduction
The sticky platelet syndrome (SPS) was first described in 1983 1 ; however, not until later did its prevalence receive significant recognition in the medical literature. 2 –33 The SPS is a rather common cause of arterial and venous thrombosis, 2 –6 and it accounts for about 20% of otherwise unexplained arterial events and 13% of unexplained venous thrombotic events. 2 –8 Three forms of the SPS have been identified: type I is marked by platelet hyperaggregability with both adenosine diphosphate (ADP) and epinephrine, whereas type II evidences hyperaggregability only with epinephrine and type III only with ADP. 3 –6 The platelet abnormality seems to be congenital, and the precise nature of the defect is currently unknown 4 ; it has been supposed that glycoprotein (GP) receptors on the platelet surface membrane may be involved, its abnormality leading into platelet hyperfunction. 7–8 Up to now, no molecular substrate has been found to explain the platelet hyperaggregability in the SPS phenotype, this being the reason why only a few research groups have accepted this entity as a true thrombophilic condition. 29 –33 Only a few attempts to correlate the SPS phenotype with molecular markers of platelet hyperaggregability have been described, the GP IIIa PLA1/A2 (HPA-1a/b ITGB3: c.196T>C) polymorphism 7,32 and the growth arrest-specific gene 6 (Gas6; Gas6: c.834+7G>A) polymorphisms. 8
The treatment of the SPS relies on diminishing the platelet hyperaggregability by means of employing antiplatelet drugs 18,28,31,33 ; in most cases, aspirin is adequate to revert the phenomenon, 28 but there are instances in which other antiplatelet drugs must be employed. Herein, we describe our experience in the treatment of 55 patients with the SPS, studied, and treated in a single institution.
Material and Methods
Patients
Between August 2002 and May 2013, all consecutive Mexican mestizo patients studied and treated in the Centro de Hematología y Medicina Interna (Clínica RUIZ) de Puebla were prospectively accrued in the study if, in addition to one of the following clinical markers associated with a primary hypercoagulable state 26–27 : (1) venous or arterial thrombosis at age below 40 years; (2) family history of thrombosis; (3) recurrent thrombosis without apparent precipitating factors; (4) thrombosis at unusual anatomic sites, and (5) resistance to conventional antithrombotic therapy, they had the SPS phenotype. Individuals with overt malignancy, pregnancy, puerperium, oral contraceptives, or other conditions associated with secondary thrombophilia were excluded from the study. Only patients with at least 2 consecutive assessments of the SPS were included in the study.
Assessment of the Sticky Platelet Syndrome Phenotype
In an effort to make results comparable and being consistent with the previous studies, the method described by Mammen et al
2,4
was used, using exactly the same conditions, agents, and dilutions: Blood was drawn, usually between 8:30 and 10:30
Treatment
All patients were initially instructed to receive aspirin, 100 mg/d, per os (po), with exception of individuals known to be allergic or intolerant to the drug, which were given clopidogrel 75 mg/d, po. Patients who failed to diminish the platelet hyperreactivity were switched to aspirin + clopidogrel at the same doses. In patients with the activated protein C resistance phenotype or protein C deficiency, rivaroxaban (10 mg/d) was employed. In patients with the 677C→T mutation in the 5,10-methylen-tetrahydrofolate-reductase (MTHFR), folic acid (5 mg/d) was used in addition to the antiplatelet therapy.
Results
Patients
A total of 55 patients with a clinical marker of primary thrombophilia displaying the SPS phenotype were identified, 17 males and 38 females. Median age was 49 years, range 10 to 94. The median age of the males (59 years, range 22-64) was significantly higher than that of females (49 years, range 15-94). Estrogen use was recorded in 4 of 38 females. All patients fulfilled the criteria of a primary hypercoagulable state (vide supra). The vaso-occlusive episodes presented in the lower limbs in 35%, in the head and neck in 33%, in the abdomen in 19%, and in the eye in 6% of patients; 9% of the patients had a pulmonary thromboembolism.
Sticky Platelet Syndrome Phenotype
Of the 55 patients, 35 had type I SPS, 3 had type II SPS, and 17 had type III SPS. Of the 55 patients, 48 (87%) showed hyperaggregability at the highest dilution for ADP, whereas 30 (54%) of 55 showed hyperaggregability at the highest dilution for epinephrine. All patients showed hyperaggregability at the highest dilution with either ADP or epinephrine.
Treatment
Of the 55 patients, 53 were given aspirin initially whereas 2 were given clopidogrel upfront. Thirteen patients given aspirin initially were changed from aspirin to aspirin + clopidogrel, because the platelet hyperaggregability did not revert 4 weeks after starting the treatment. As a result, 40 patients received aspirin, 13 patients received aspirin + clopidogrel, and 2 patients received only clopidogrel. Patients were followed for periods of 1 to 129 months, median 13 months.
Response to Treatment
Patients were required to have at least 2 assessments of the SPS, 1 before and 1 after the treatment; the median of studies to asses SPS was 3 (range 2-9). Table 1 shows the data of the platelet aggregation response to the 3 dilutions of both ADP and epinephrine. It is clear that the mean values of the platelet responsiveness to both aggregation-inducing agents significantly diminished as a result of the treatment. Patients were treated and followed during a median of 13 months (range 1-129 months). Only 2 (3.6%) of the 55 patients developed another vaso-occlusive episode despite the treatment, 52 and 129 months after starting the antiplatelet therapy; interestingly these 2 episodes were located in the retinal central artery, and none of these 2 individuals had additional thrombophilic conditions associated despite a full laboratory workup. 26,27 All the 55 patients included in the study had at least 1 episode of thrombosis before starting the treatment; once the treatment was started, the freedom from rethrombosis of the 55 patients was 96.4% at 129 months; conversely, the rethrombosis rate at the same period was 3.6% (see Figure 1). The changes in the platelet aggregation patterns after the treatment with the antiplatelet drugs were analyzed for males and females separately, and the differences were found to be nonsignificant.
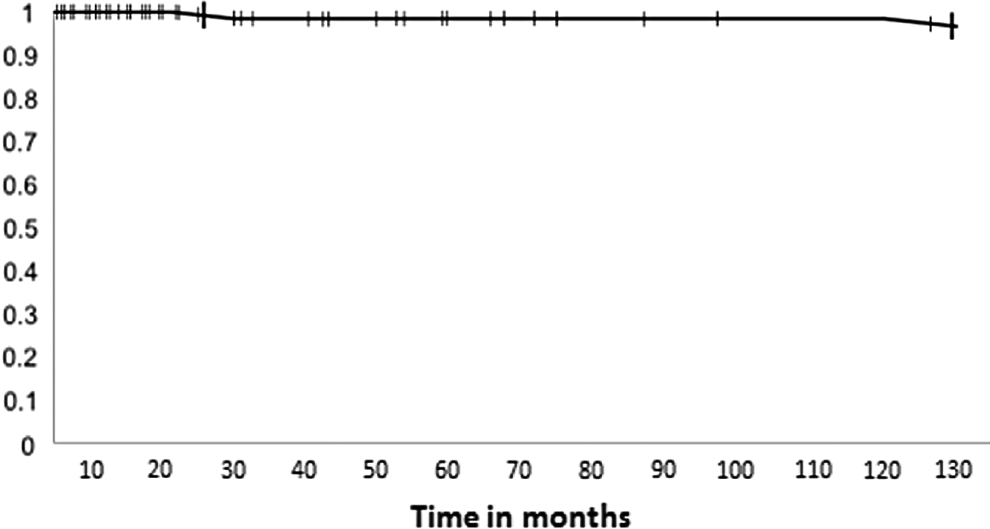
Freedom from rethrombosis in the 55 patients with sticky platelet syndrome treated with antiplatelet drugs. The thick marks represent rethrombosis episodes.
Platelet Aggregation Values in the 55 Patients With the Sticky Platelet Syndrome at Diagnosis and After Treatment With Antiplatelet Drugs.a
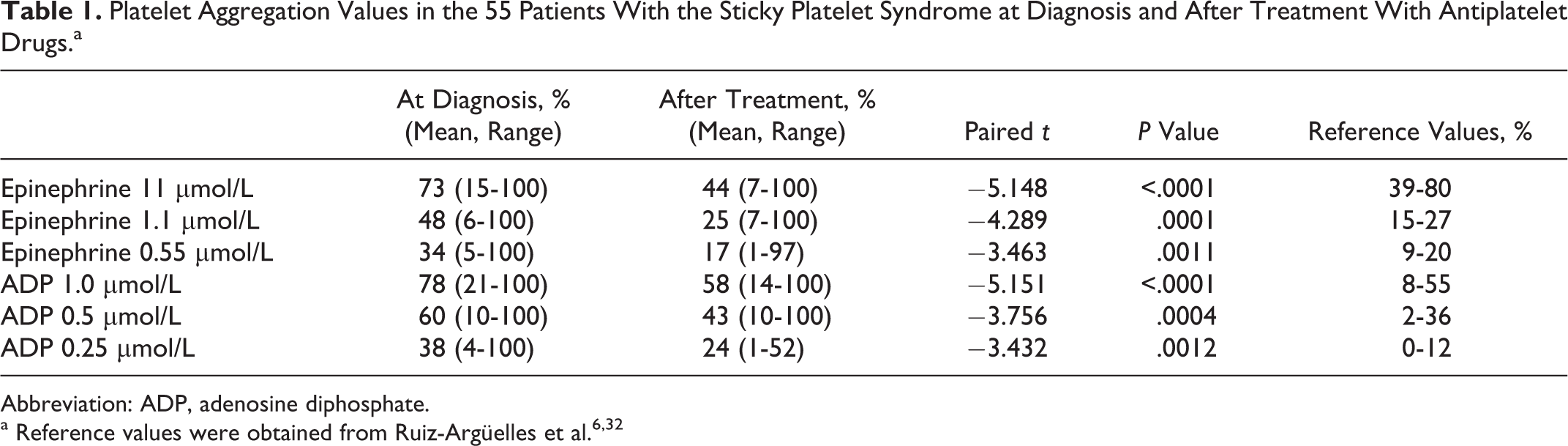
Abbreviation: ADP, adenosine diphosphate.
Discussion
In the last years, we have been interested in analyzing the changes in the hemostatic system of Mexican mestizos, which can result in thrombophilia. 6,26,27,35 –38 In these studies, we have found that the SPS is the second most frequent thrombophilic condition identified in Mexican mestizos with a clinical marker of thrombophilia, 6,26,27 only surpassed by the 677C→T mutation in the MTHFR gene. In Mexico, we 6,26,27,33 and others 22,25 have found that approximately 50% of Mexican mestizo patients with a clinical maker of thrombophilia display the SPS phenotype. Most patients with the SPS display other thrombosis-prone conditions but there are also instances of the SPS identified as the single thrombophilia marker 6,26,27,33 . It is therefore possible that the SPS may contribute to the so-called “multifactorial thrombophilia.” 26,33
There are few articles dealing with the treatment of the SPS; most experiences stem from case reports. 18,28,30 In this prospective study, we have shown that the platelet hyperaggregability of persons displaying the SPS phenotype can be reverted in most cases by means of aspirin; we were able to show this in 40 (75%) of 53 patients; in the remaining 25% of the individuals, other antiplatelet drugs were needed; in our experience clopidogrel was employed. What is more salient is that by means of the antiplatelet drugs, the rethrombosis rate at 129 months was 3.6%, thus indicating that the freedom from rethrombosis of the whole group of 55 patients was 96.4% at 129 months (see Figure 1). Accordingly, the simple and inexpensive treatment with aspirin was useful to prevent further thrombotic episodes in this cohort.
In summary, we have been able to prove that using antiplatelet drugs, mainly aspirin, the platelet hyperreactivity of patients with the SPS phenotype can be reverted and that this translates into a substantial decrease in the rethrombosis rate. Further studies are needed to confirm this observation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.