
Abstract
Background:
Coagulation and anticoagulation systems are good targets of antiphospholipid antibodies. We assessed the contribution of the antiphospholipid antibodies to the thrombotic risk.
Methods:
Enzyme-linked immunosorbent assays on antibodies against phosphatidylserine and prothrombin (PS/PT), protein C, protein S, protein Z, and thrombomodulin were performed in 164 patients who showed positive results for lupus anticoagulant or anticardiolipin antibody.
Results:
Anti-β-2-glycoprotein I (β2GPI) and anti-PS/PT were significant risk factors for thrombotic events (P < .001, P = .049). However, there was no association between antiprotein C, antiprotein S, antiprotein Z, or antithrombomodulin and thrombosis. Coexistence of anti-β2GPI and anti-PS/PT antibodies was significantly associated with thrombotic events (P = .001). Interestingly, the absence of both anti-β2GPI and anti-PS/PT antibodies was a significant preventive factor for thrombosis (P = .003).
Conclusion:
Our data show a lack of association of antiprotein C, antiprotein S, antiprotein Z, and antithrombomodulin antibodies with thrombosis. However, the combination of conventional anti-β2GPI with anti-PS/PT antibody is expected to enhance the predicting power of thrombotic risk.
Keywords
Introduction
Antiphospholipid antibodies are a family of autoantibodies associated with an increased risk of thrombotic disease. 1 The predominant targets are anionic phospholipid-bound proteins such as β-2-glycoprotein I (β2GPI) and prothrombin (PT). Because the anti-β2GPI antibody is a strong predictor of thrombosis, 2 it is currently one of the laboratory parameters that indicates antiphospholipid syndrome. 3 In contrast, antiprothrombin antibody was not found to be a significant thrombotic risk factor. 4 A recent study showed that antiprothrombin antibody is directed against cryptic epitopes exposed when PT binds to phospholipids, because negatively charged phospholipid binds to PT during its activation. 5 Therefore, PT complexed with phosphatidylserine (PS) is more efficiently recognized by the anti-PT antibody than is by PT alone. Therefore, the antibody against a complex of anionic phospholipids such as PS and PT was strongly associated with thrombosis. 6,7
Among possible mechanisms predisposing to thrombosis, antibodies that inhibit the protein C anticoagulant pathway are good candidates for pathogenic antibodies, 8 because the protein C pathway plays a role in a major regulatory loop that limits thrombin generation. It has been reported that activated protein C (APC) resistance is a strong risk factor for venous thromboembolism 9 and is associated with coexistence of anti-PT. 10 The antibody against protein S was reported as a strong risk factor for thrombosis. 11 We also reported high prevalence (38.7%) of antiprotein S antibody in patients with systemic lupus erythematosus (SLE). 12 Besides the reports on antiprotein S antibody, there were a few reports about antibodies against protein C 13 and thrombomodulin 14 in autoimmune diseases.
Protein Z is a vitamin K-dependent plasma protein that serves as a cofactor in the inhibition of factor Xa by the protein Z-dependent protease inhibitor. Protein Z deficiency leads to a propensity for thrombosis; moreover, antiprotein Z antibody is also commonly present in patients with positive lupus anticoagulant (LA). 15,16 Considering that protein Z is a natural anticoagulant, antiprotein Z antibody may be a predisposing factor for antiphospholipid syndrome.
Although the antibodies against PS/PT, protein C, protein S, protein Z, and thrombomodulin were individually demonstrated as thrombotic risk factors in several studies, 6,7 to our acknowledge, there was no study to investigate the candidate antibodies simultaneously in high-risk thrombotic patients. This study investigated whether antibodies against PS/PT, protein C, protein S, protein Z, and thrombomodulin predict thrombosis in patients with positive LA or anticardiolipin (anti-CL) antibody. In addition, we determined whether a combination of these antiphopholipid antibodies provides additional predictive value for thrombosis. Finally, we investigated the significant difference of clinical characteristics and antibody prevalence in terms of the methods of LA tests.
Materials and Methods
Study Population
This study was approved by the Institutional Review Board of Seoul National University Hospital. This study enrolled 164 patients with positive LA and/or positive anti-CL antibody from Seoul National University Hospital between June 2008 and June 2010. For these patients, LA or anti-CL antibody was ordered for the workup of prolonged clotting time, hypercoagulability, autoimmune disease, or pregnancy morbidity. None of the included patients harbored factor V Leiden or PT gene mutation or had received warfarin or heparin therapy.
The demographic, clinical, and laboratory characteristics of the study population are shown in Table 1. The median age was 42 (range, 10–95). In all, 59 (36.0%) patients were diagnosed with autoimmune diseases. Patients with SLE were the highest in number, followed by those with rheumatoid arthritis, Behcet disease, and Sjogren syndrome. In all, 26 (15.9%) patients experienced episodes of thrombotic events, venous thromboembolism in 16, arterial thromboembolism in 7, and both venous and arterial thromboembolism in 3 patients. The number of patients with positive results for LA and anti-CL antibody was 85 and 115, respectively.
Demographic, Clinical, and Laboratory Features of Patients (n = 164).a
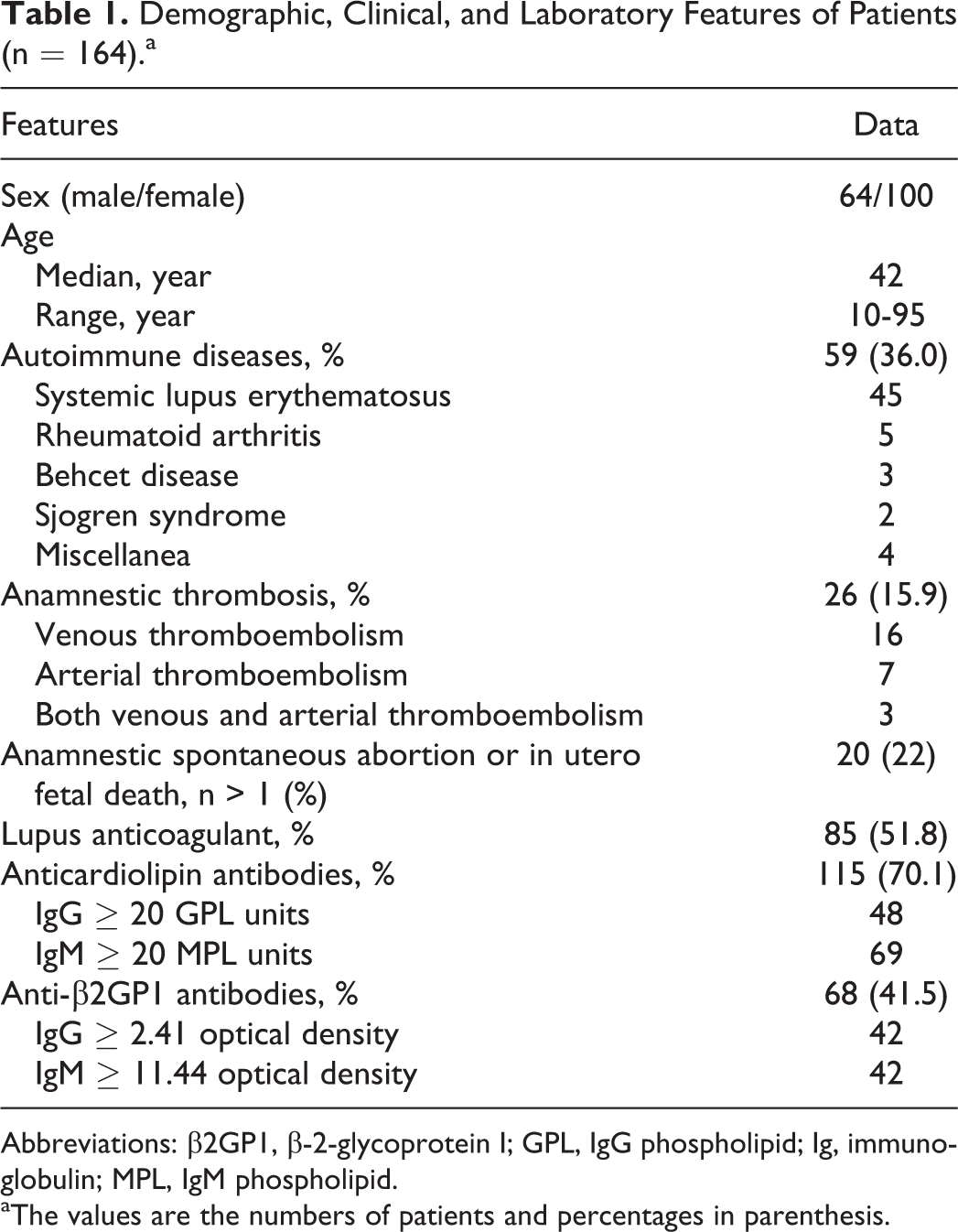
Abbreviations: β2GP1, β-2-glycoprotein I; GPL, IgG phospholipid; Ig, immunoglobulin; MPL, IgM phospholipid.
aThe values are the numbers of patients and percentages in parenthesis.
Plasma samples obtained from 45 normal healthy adults who have no history of hospitalization and autoimmune diseases were used to define the cutoff values for each assay.
Blood Samples
Peripheral blood was collected in commercially available sodium citrate tube (Becton Dickinson, San Jose, California). Within 2 hours after sampling, whole blood samples were double centrifuged for 15 minutes at 2000g and for 10 minutes at 2500g, and the platelet-free plasma samples were aliquoted and stored at −70°C.
Lupus Anticoagulant Tests
The LA test was performed on the ACL TOP coagulation analyzer (Instrumentation Laboratory, Milan, Italy) with 2 types of integrated tests; diluted Russell viper venom (dRVVT) assay (LAC Screen/Confirm kit; Instrumentation Laboratory) and silica clotting time (SCT) assay (Instrumentation Laboratory). 17 The “normalized ratio,” which was calculated as (patient screen results/mean of screen normal range) divided by (patient confirm results/mean of confirm normal range), was used according to the manufacturer’s instructions. The presence of LA was confirmed when a sample was positive in at least 1 of these 2 tests according to the guidelines proposed by the antiphospholipid antibodies Standardization Subcommittee of the International Society on Thrombosis and Haemostasis. 18
Antiphospholipid Antibodies
Immunoglobulin(Ig) G (IgG) and IgM anti-CL, anti-β2GPI, anti-PS/PT, antiprotein C, antiprotein S, and antiprotein Z antibodies were measured using commercially available enzyme-linked immunosorbent assay (ELISA) kits APhL (Louisville APL Diagnostics, Atlanta, Georgia), QUANTA Lite β2-GPI (INOVA Diagnostics, San Diego, California), QUANTA Lite aPS/PT (INOVA Diagnostics), ZYMUTEST antiprotein C (HYPHEN BioMed, Neuville-sur-Oise, France), ZYMUTEST antiprotein S (HYPHEN BioMed), and ZYMUTEST antiprotein Z (HYPHEN BioMed), respectively. The anti-CL was considered positive when the IgG phospholipid (GPL) units or IgM phospholipid (MPL) units exceeded 40 units. Besides the anti-CL, the upper 99th percentiles of the normal control values were chosen as the normal cutoff point for the other antibodies, anti-β2-GPI, 2.41 (IgG) and 11.44 (IgM); anti-PS/PT, 23.81 (IgG) and 85.84 (IgM); antiprotein C, 8.06 (IgG) and 9.43 (IgM); antiprotein S, 11.05 (IgG) and 12.49 (IgM); and antiprotein Z, 10.0 (IgG) and 10.0 (IgM).
Antithrombomodulin IgG antibody was measured according to the method described in a previous report 16 with some modification. In brief, microplates (Maxisorp, eBioscience, San Diego, CA, USA) were coated with purified human thrombomodulin (10 µg/mL; American Diagnostica, Stamford, Connecticut) in 0.1 mol/L carbonate buffer (pH 9.5, Sigma Aldrich, St Louis, Missouri) at 4°C overnight. After the test plasma was blocked with 1% gelatin (Sigma Aldrich), it (1:50 diluted with phosphate-buffered saline) was incubated for 1 hour at room temperature, and peroxidase-conjugated Fc-specific anti-human IgG (1:5000; Sigma Aldrich) was added for 1 hour. After the reaction was stopped using 3 mol/L sulfuric acid (Sigma Aldrich), the absorbance at 492 nm was measured. Results are expressed as the optical density (OD) difference between coated and uncoated wells. The cutoff value was defined as 0.34, which was the upper 99th percentile of OD readings from normal controls.
Statistical Analysis
Statistical analyses were carried out using the SPSS 12.0 (Chicago, Illinois). Data were tested for normality and were found to be nonnormally distributed. Comparisons of variables between different subgroups were performed using the Mann-Whitney U or chi-square tests. Odds ratios (ORs), as measures of the relative risk of thrombotic complication, were estimated using age- and sex-adjusted logistic regression analysis, and 95% confidence intervals (CIs) were also calculated. Two-sided P values <.05 were considered significant.
Results
The association between thrombotic events and individual laboratory test results using age- and sex-adjusted logistic analysis is presented in Table 2. The anti-β2GPI (IgG or IgM, IgG, and IgM) and anti-PS/PT (IgG or IgM, IgG, and IgM) were significant risk factors for thrombotic events. However, there was no association between antiprotein C, antiprotein S, antiprotein Z, and antithrombomodulin, and thromboembolism.
Association Between the Prevalence of Thromboembolism (TE) and Individual laboratory Test Results.a
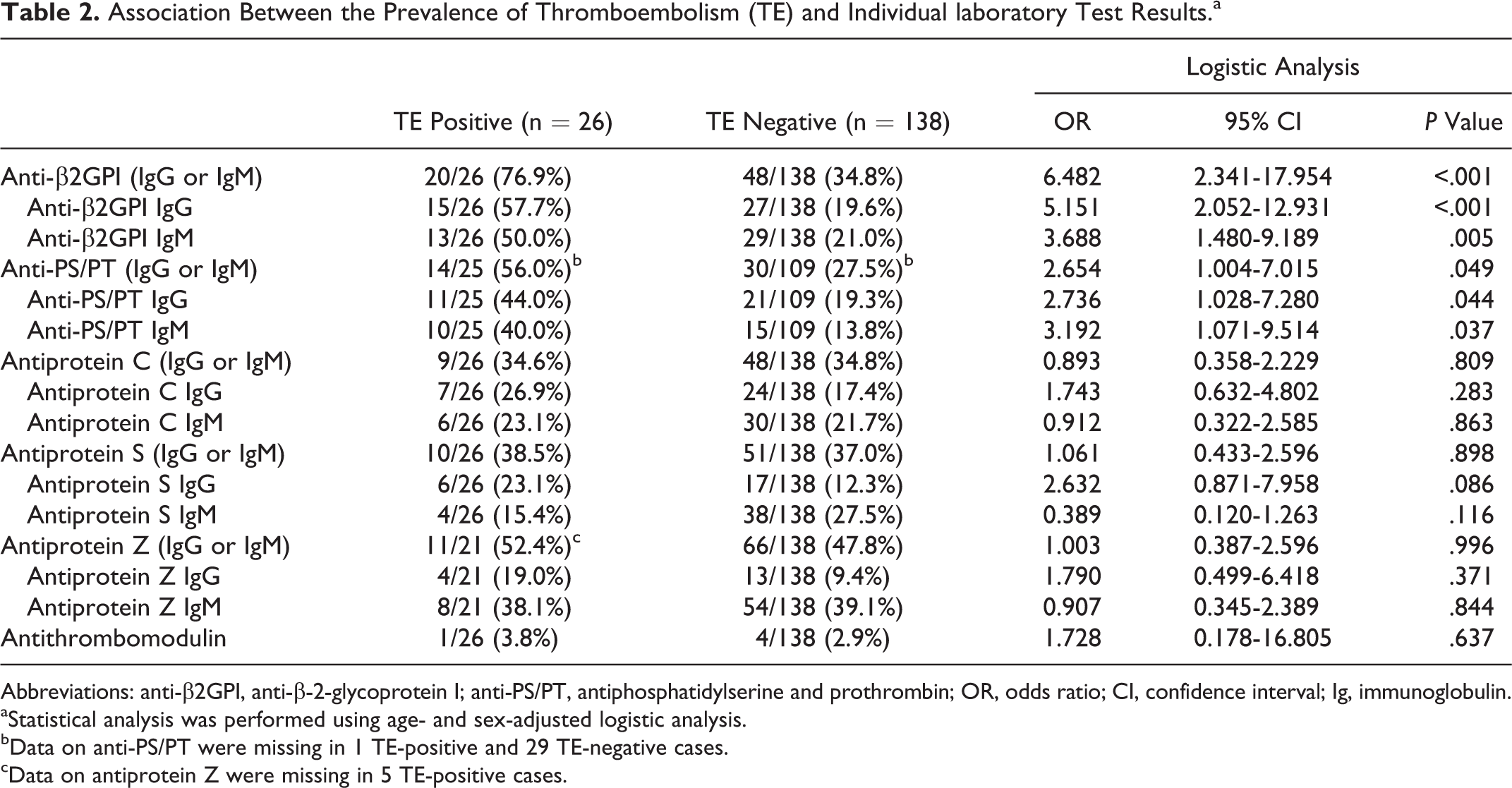
Abbreviations: anti-β2GPI, anti-β-2-glycoprotein I; anti-PS/PT, antiphosphatidylserine and prothrombin; OR, odds ratio; CI, confidence interval; Ig, immunoglobulin.
aStatistical analysis was performed using age- and sex-adjusted logistic analysis.
bData on anti-PS/PT were missing in 1 TE-positive and 29 TE-negative cases.
cData on antiprotein Z were missing in 5 TE-positive cases.
Because both β2GPI and PS/PT are considered to be the major targets of antiphospholipid antibodies, 1 we investigated the combined effect of anti-β2GPI and anti-PS/PT on thrombotic risk (Table 3). Double positivity of anti-β2GPI and anti-PS/PT (OR, 7.000; 95% CI, 2.289–21.404; P = .001) was a strong risk for thrombotic event. Interestingly, double negativity of anti-β2GPI and anti-PS/PT was a significant preventive factor for thromboembolism (OR, 0.189; 95% CI, 0.063–0.567; P = .003).
Thrombotic Risk of Combination of Anti-β2GPI with Anti-PS/PT Antibodies.a
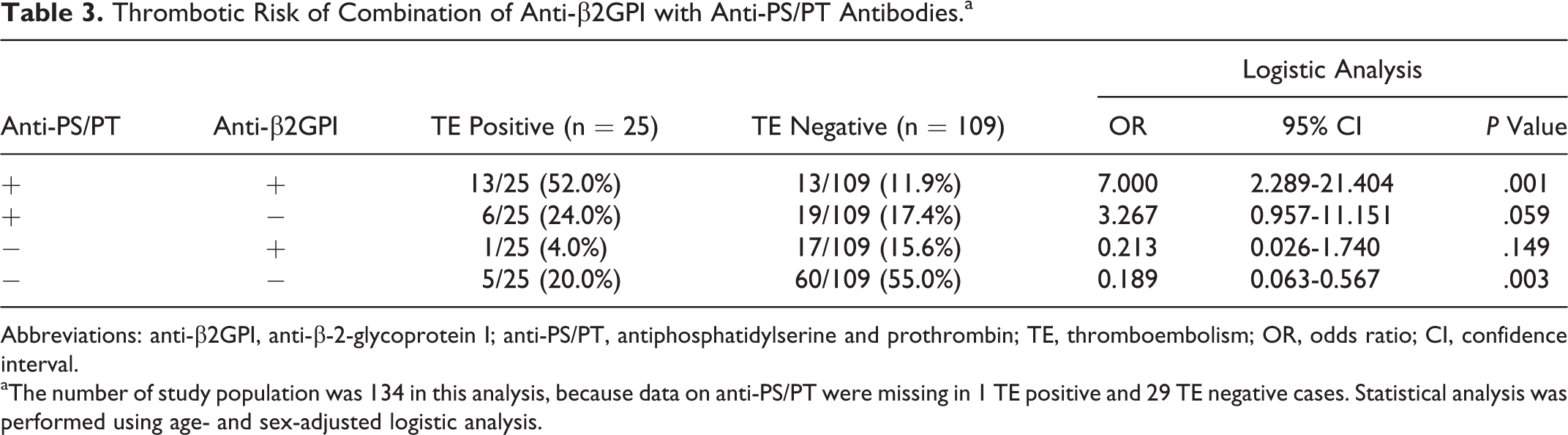
Abbreviations: anti-β2GPI, anti-β-2-glycoprotein I; anti-PS/PT, antiphosphatidylserine and prothrombin; TE, thromboembolism; OR, odds ratio; CI, confidence interval.
aThe number of study population was 134 in this analysis, because data on anti-PS/PT were missing in 1 TE positive and 29 TE negative cases. Statistical analysis was performed using age- and sex-adjusted logistic analysis.
We divided 85 patients with positive LA into 2 groups according to the detection methods of LA (Table 4). The dRVVT group included the patients with the ratio of the dRVVT, which exceeded that of the SCT, and the SCT group included those with the ratio of the SCT, which exceeded that of the dRVVT. Interestingly, the arterial thrombosis was significantly prevalent in the dRVVT group. However, the other frequencies of antiphospoholipid antibodies were not significantly different.
Clinical Features and Antiphospholipid Profile of 85 Patients With Lupus Anticoagulant Classified According to Detection Method of Lupus Anticoagulant.a
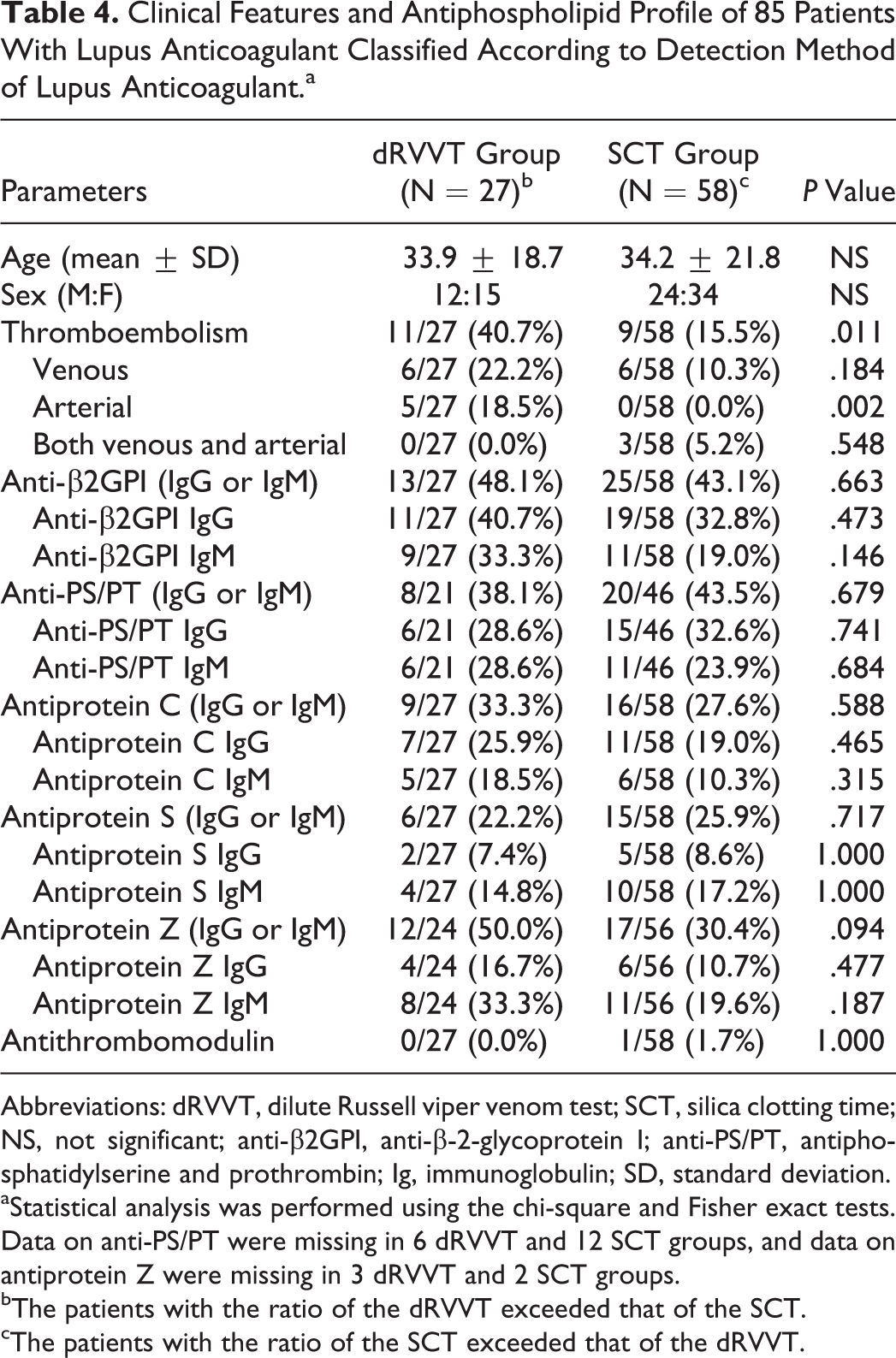
Abbreviations: dRVVT, dilute Russell viper venom test; SCT, silica clotting time; NS, not significant; anti-β2GPI, anti-β-2-glycoprotein I; anti-PS/PT, antiphosphatidylserine and prothrombin; Ig, immunoglobulin; SD, standard deviation.
aStatistical analysis was performed using the chi-square and Fisher exact tests. Data on anti-PS/PT were missing in 6 dRVVT and 12 SCT groups, and data on antiprotein Z were missing in 3 dRVVT and 2 SCT groups.
bThe patients with the ratio of the dRVVT exceeded that of the SCT.
cThe patients with the ratio of the SCT exceeded that of the dRVVT.
Discussion
The anti-PT antibody population is heterogeneous and comprises antibodies directed against PT alone coated on γ-irradiated or -activated polyvinylchloride plates or against a PS/PT complex. 5 Anti-PT did not associate with thrombosis, while anti-PS/PT showed strong correlation with thrombotic events. 7 A recent study also confirmed that anti-PS/PT was superior to anti-PT for the detection of antiphospholipid syndrome. 19 In our results, anti-PS/PT was demonstrated to be a significant risk factor for thrombosis. However, the OR of anti-PS/PT (2.654) was not higher than that of anti-β2GPI (6.482). Since anti-β2GPI antibody was included as one of the markers in the international criteria for antiphospholipid syndrome, 3 we further analyzed the combined thrombotic risk of anti-β2GPI and anti-PS/PT. As expected, the combination of anti-β2GPI and anti-PS/PT strongly increased the thrombotic risk. Consistent with our result, a recent study demonstrated that positivity of multiple antibodies increased thrombotic risk. 20 Moreover, the lack of both anti-β2GPI and anti-PS/PT was a significant preventative factor for thrombotic events. This information could be important in choosing adequate markers for antiphospholipid syndrome detection in the future.
The protein C pathway is an important physiological anticoagulant system, 21 and the antibodies that inhibit the protein C anticoagulant pathway are likely candidates as pathogenic antiphospholipid antibodies. 22 Therefore, several targets against the protein C pathway such as protein C, 13 protein S, 11 and thrombomodulin 14 have been explored in antiphospholipid syndrome. Although the antiprotein S was prevalent in patients with SLE, 11 our results did not show any association of antiprotein S with thrombosis. Moreover, antiprotein C also did not have any thrombosis predictive power. One in vitro experiment showed that the antiphospholipid antibodies inhibited APC activity through inhibition of the phospholipid surface required for the anticoagulant function of the APC complex. 23 Therefore, rather than simple immunologic detection of antiprotein C and antiprotein S antibodies, a functional method to measure the resistance of APC is required for the detection of significant antiphospholipid antibodies.
In our study, antithrombomodulin IgG antibody was measured using the “in-house” ELISA system. Antithrombomodulin antibody was not a significant risk factor for thrombosis. Contrary to our data, other studies suggested that certain antiphospholipid antibodies reacted to thrombomodulin and induced thrombosis in animal model 24 and that antithrombomodulin antibody may be associated with venous thrombosis. 16
Our results of antiprotein Z antibody was not found to be significant, although a previous study suggested an association between antiprotein Z antibody and thrombosis. 16 These differences in clinical significance may result from differences in intrinsic sensitivity of detection systems or study populations.
The limitation of this study is to define statistical outcome as a thromboembolic event instead of antiphospholipid syndrome. Although antiphospholipid syndrome was officially diagnosed in patients with thrombosis when 1 of the 3 tests including anti-CL, anti-β2GPI, and LA was present on 2 or more occasions at least 12 weeks apart, 3 these tests were usually checked 1 time in our study population. However, thrombotic event is considered to be a good surrogate outcome for detection of useful antibodies. In practical field, clinician is needed to notice that the diagnostic tests for antiphospholipid syndrome should be checked on 2 consecutive occasions. Second, our study population included 20 patients with pregnancy morbidity (Table 1). Although there was a significant association of anti-β2GPI with pregnancy morbidity (OR 6.73, 95% CI 1.60-23.25, P = .009), anti-PS/PT antibody did not show any significant association with pregnancy morbidity, probably due to relatively small number of patients with pregnancy morbidity and some combined effect with thromboembolic event. In our study, therefore, we focused on the thrombotic risk of each antibody. Third, we did not perform each ELISA in duplicate, because the amount of specimen was not sufficient for 11 ELISAs.
In summary, our data demonstrated that anti-β2GPI and anti-PS/PT antibodies were significant thrombotic markers. However, antiprotein C, antiprotein S, antithrombomodulin, and antiprotein Z did not show any significant association with thrombosis. The coexistence of anti-β2GPI and anti-PS/PT antibodies was a strong thrombotic risk, and simultaneous absence of anti-β2GPI and anti-PS/PT antibodies was a negative risk factor. The anti-PS/PT antibody is expected to enhance the predicting power of thrombotic risk.
Footnotes
Authors’ Note
Both Hyungsuk Kim and Ji-Eun Kim contributed equally toward the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant of the Korean Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (A120659).