
Abstract
A debate concerns the utility of large screening for acquired or inherited thrombophilia. The study concerns relationship between inherited thrombophilic status and lower limb deep vein thrombosis (LDVT) and highlights the possible use of extensive thrombophilia screening to determine an emerging risk of LDVT. From January 2010 to January 2012, 103 consecutive patients with LDVT were considered. In all, 57 (55.3%) patients with LDVT showed inherited thrombophilia. The most frequent trombophilic alterations were deficiency of protein S (33 patients, 32.0%), methylentethrafolate reductase (MTHFR) gene C677T variant (22 patients, 21.4%), protrombin gene G20210A alteration (50, 14.6%), and deficiency of protein C (12, 11.6%). Age and MTHFR variant were found related to LDVT and thrombophilia was related to distal LDVT. A high frequency of thrombophylic factor was found in patients with LDVT, but we believe that a generic genetic screening should not be suggested for these patients.
Introduction
Lower limb deep vein thrombosis (LDVT) is one of the most common events of venous thromboembolism (VTE). 1 –5 Inherited and acquired hypercoagulative status is considered as a pivotal factor in determining LDVT and consequently it is widely investigated. Genetically determined tendency to VTE is commonly known as inherited thrombophilia, and it is detectable at least in 30% to 40% of the patients with VTE. Consequently, it is normally considered to play a key role in the clinical picture of VTE as pulmonary embolism (PE) and LDVT. 6–7 The identification of the level of risk of VTE is crucial in developing optimal strategies for both preventing and treating new VTE events and also against the high rate of mortality (United States: 18 000-1 00 000 per year) caused by VTE. 7–8 Data from the RIETE Registry 9 did not provide the relationship between all the prothrombotic markers included in the thrombophilic panel, but however factor V Leiden (FVL) and resistance to activated protein C (prot C) were found as risk factors for developing LDVT. Moreover, a survey performed in a critical care department showed higher frequency of FVL in patients with isolated LDVT and also a significant presence of prothrombin G20210A mutations was found in patients with LDVT and PE. 10 In the past few years, the search for one or more thrombophilic markers including genetic variants (FVL, prothrombin G20210A, antipospholipid antibodies, lupus anticoagulants) or blood defects (antithrombin III, proteins C and S) represents an intriguing objective in the management of patients with clinical evidence or suspected for VTE. Between January 2010 and January 2012, we performed a monocentric survey among patients affected only with LDVT aiming to achieve the following targets: demonstrate a relationship between the thrombophilia and LDVT and consequently postulate about a possible extensive use of thrombophilia screening in order to determine an emerging risk of LDVT.
Materials and Methods
We considered 103 consecutive patients with LDVT who came as outpatients to the Medical Angiology Unit of Department Medical and Pediatric Science of University of Catania (Hospital Garibaldi,Catania, Italy) from January 2010 to January 2012. In all, 35 patients were male and 69 patients were female, and the mean age was 50.3 ± 4.3 years. Proximal LDVT (iliac, femoral, and/or popliteal veins) was diagnosed in 64 patients, while distal LDVT (subpopliteal veins) was found in 39 patients. Majority of the LDVT (n = 94) was provoked, while only 10 of these were idiophatic LDVT. We utilized a Mylab 70 ultrasound (US) system (EsaOte Ind. Genoa, Italy) equipped with a 7-10 mHz linear probe. The presence of echogenic pattern in deep veins of lower limbs and/or no compression of veins by the US probe (positive compression US test) were considered for diagnosis of LVDT. After US diagnosis of LDVT, all the patients underwent a laboratory screening for thrombophilia which included the search for the following markers: FVL mutations, protrombin G20210A mutations, C677T variant of MTHFR, prot C, and protein S (prot S) anticoagulant. Blood sample was taken at same time of US diagnosis, and all tests were conducted by our general laboratory of clinical pathology.
Statistical Analysis
Statistical analysis was performed using a statistical package (SPSS version 10.1 for Windows). Results were given as prevalence expressed in percentage. Odds ratio (OR) and confidence interval (CI) were also determined. Differences between patients with thrombophilia and control patients without thrombophilia were estimated by the Fisher exact test. To describe the association between thrombophilic factors and LDVT, we utilized a logistic regression analysis. The OR values were given with their corresponding 95% CIs. A P value <.05 was considered statistically significant.
Results
Table 1 shows the clinical characteristics of patients included in the study.
Features of Patients with LDVT.
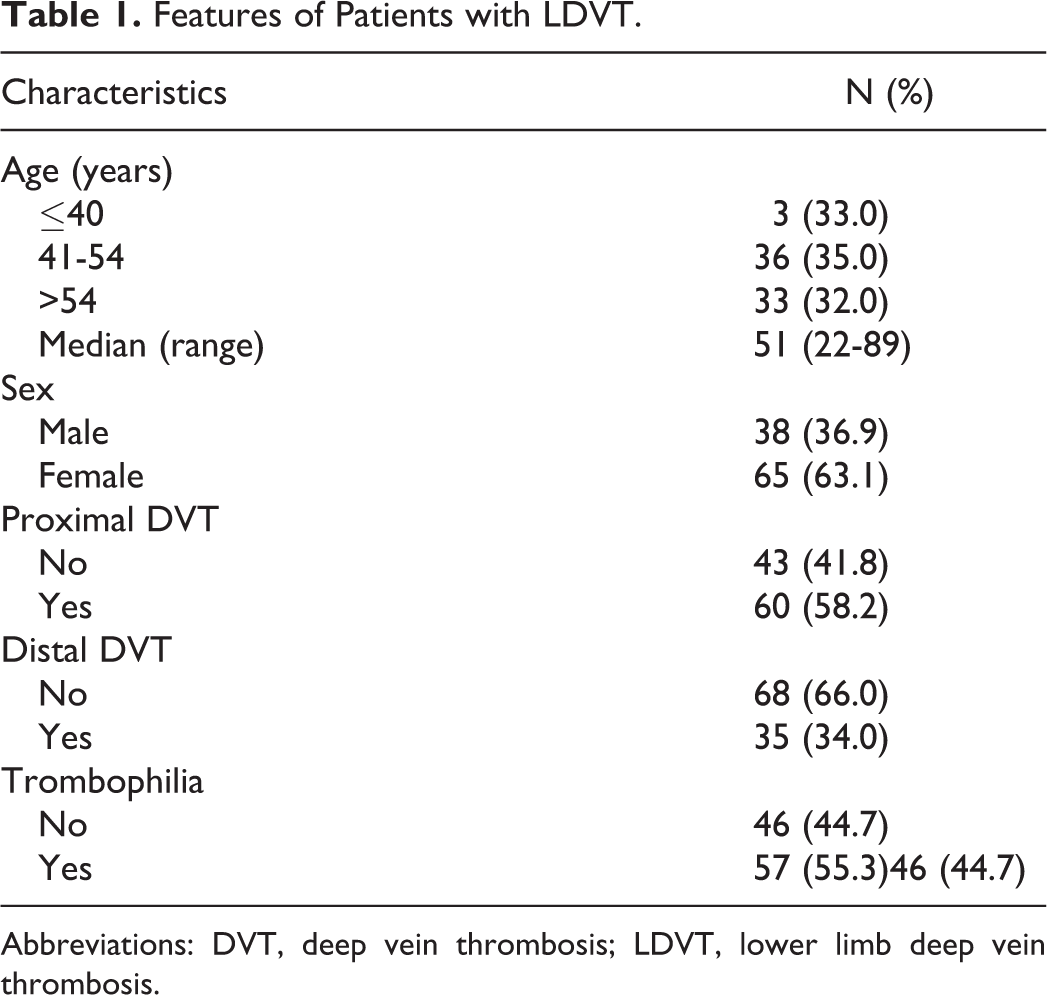
Abbreviations: DVT, deep vein thrombosis; LDVT, lower limb deep vein thrombosis.
In all, 57 (55.3%) patients with LDVT were found to have thrombophilia, while the remaining 46 (44.7%) did not have thrombophilia (Table 1). The frequency of thrombophilic factors in patients with LDVT was as follows: FVL in 8 (7.8%) patients, G20210A protrombin in 50 (14.6%) patients, and antithrombin III in 8 (7.8%) patients. Deficiency of anticoagulant prot C and prot S was found, respectively, in 12 (11.6%) and 33 (32.0%) patients with LDVT. The C677T homozygous variant of MTHFR was found in 22 (21.4%) of these patients (Table 2). The risk factors were as follows: 15 (14.6%) patients had cancer, 6 (5.8%) patients had cardiac disease, 2 (1.9%) patients had recent ischemic stroke, 3 (2.9%) patients were immobilized for more than 3 days, 4 (3.9%) patients had a recent birth (<6 months), 5 (4.8%) patients were pregnant, 9 (8.7%) patients used hormonal therapy, and 15 (14.6%) patients were obese (BMI ≥ 30; Table 3). Relationship between the above-mentioned risk factors for DVT and thrombophilia was found only in age as shown in Table 4. A relationship was found between thrombophilia and distal LDVT (OR 0.27, CI 0.10-0.63, P < .003) but not between thrombophilia and proximal LDVT (Table 5). When we considered different thrombophilic markers in patients with proximal and distal LDVT, we found a direct relationship between the MTHFR variant and the distal LDVT (OR 0.24, CI 0.07- 0.88, P < .031); conversely, no relationship was found between thrombophilic factors and proximal LDVT (Table 7).
Frequency of Thrombophilic Factors in Patients With LDVT.
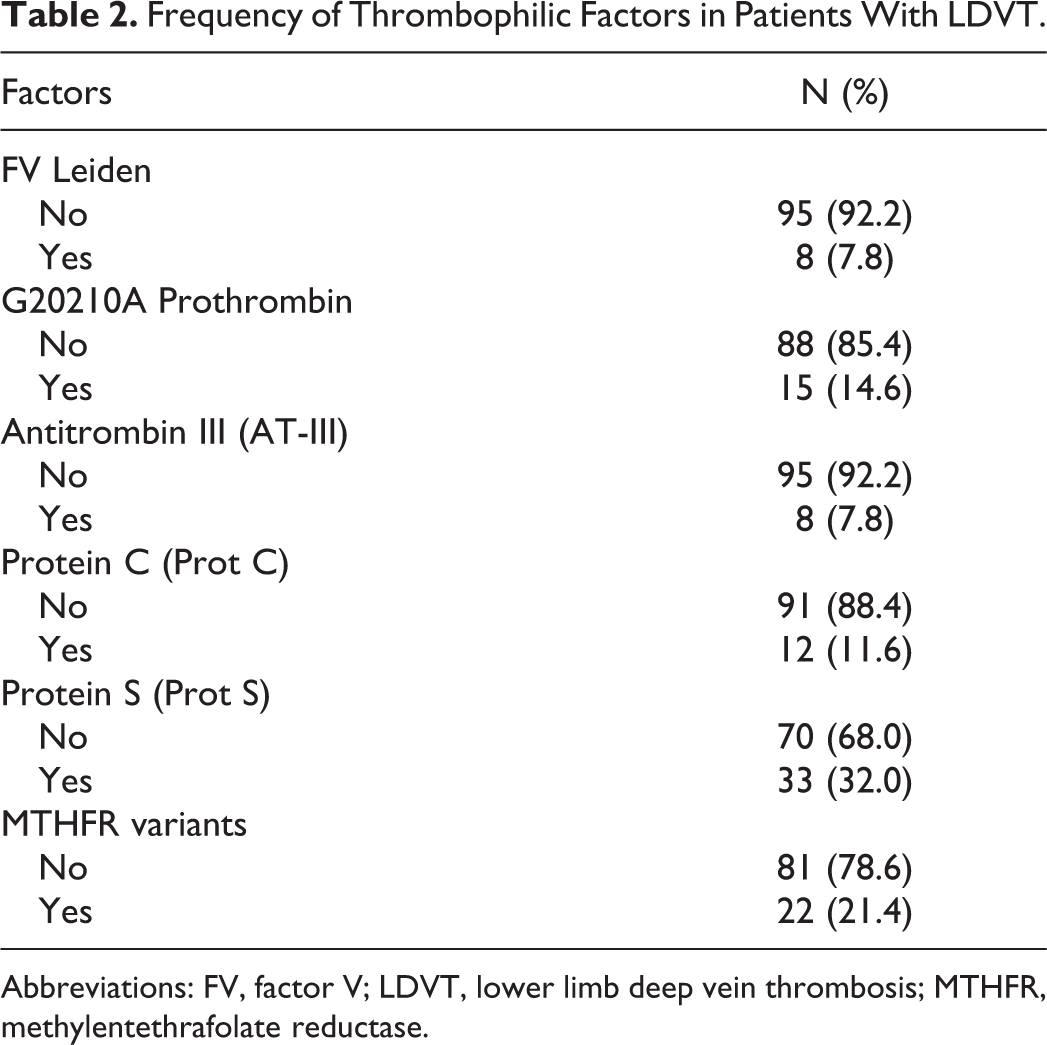
Abbreviations: FV, factor V; LDVT, lower limb deep vein thrombosis; MTHFR, methylentethrafolate reductase.
Frequency of LDVT Risk Factors in Study Cohort.
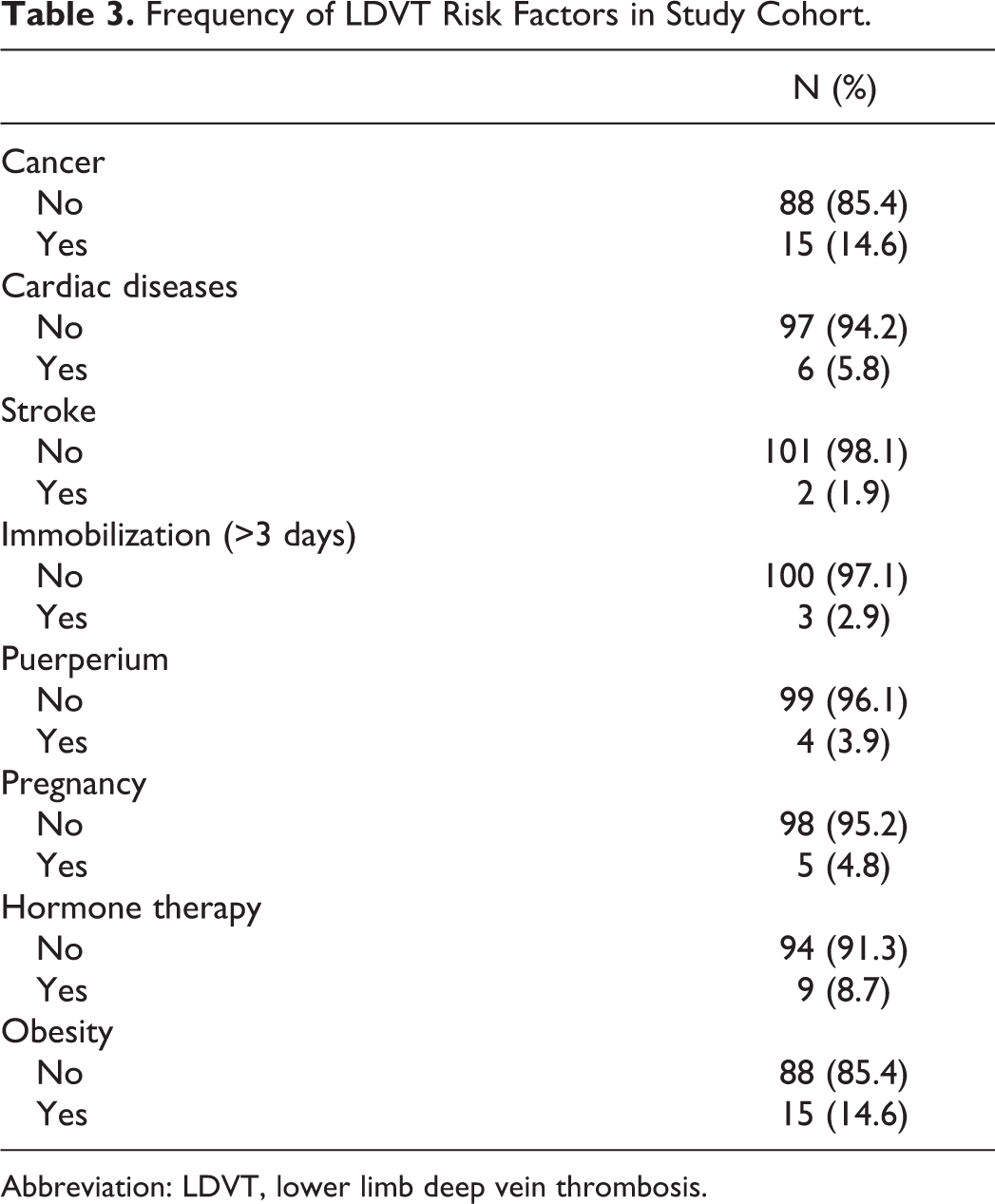
Abbreviation: LDVT, lower limb deep vein thrombosis.
Relationship Between Thrombophilia and Environmental Risk Factors for LDVT.
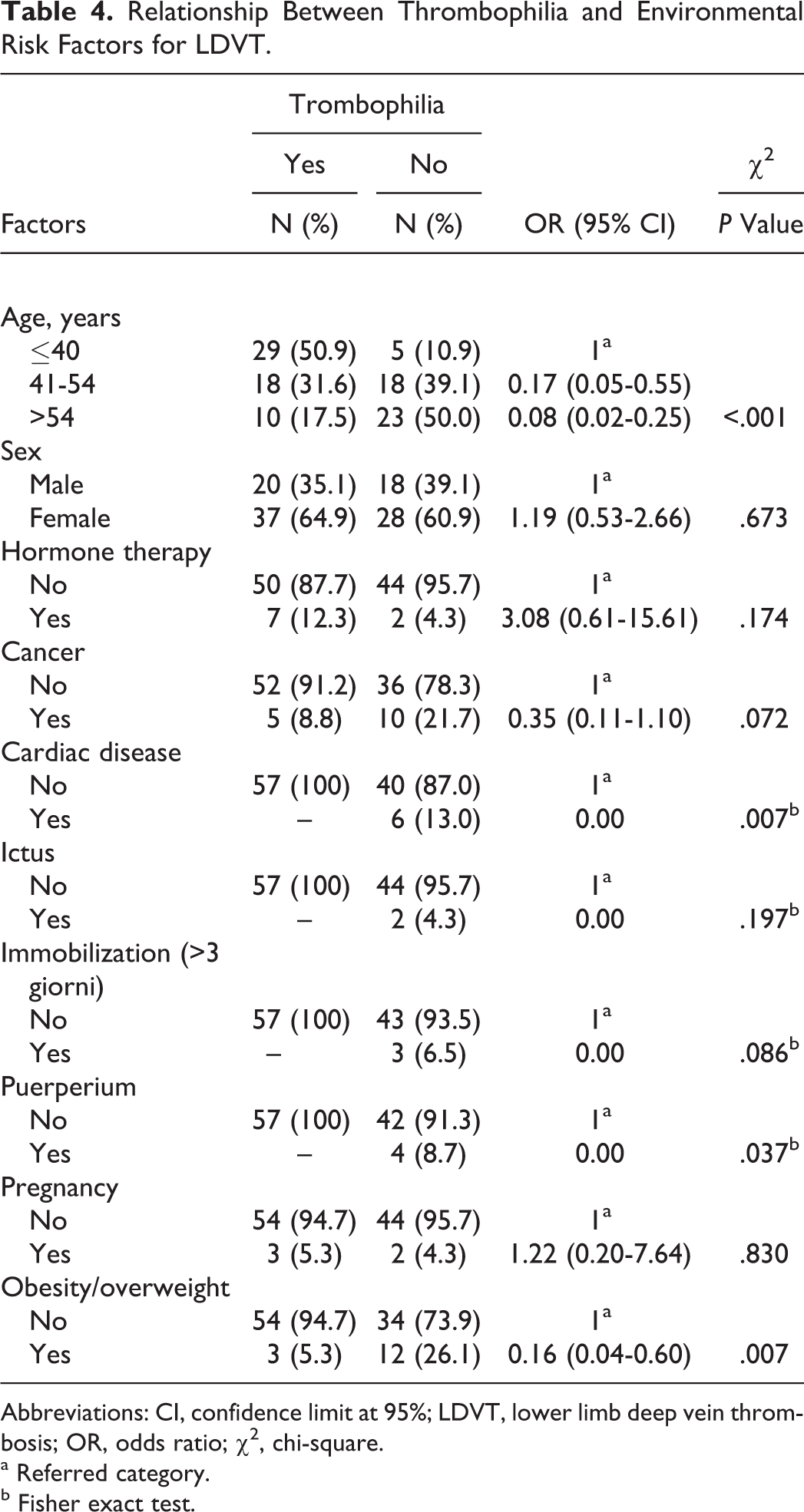
Abbreviations: CI, confidence limit at 95%; LDVT, lower limb deep vein thrombosis; OR, odds ratio; χ2, chi-square.
a Referred category.
b Fisher exact test.
Relationship Between Thrombophilia and Proximal or Distal Lower Limb Deep Vein Thrombosis (LDVT) in 103 Patients With LDVT.
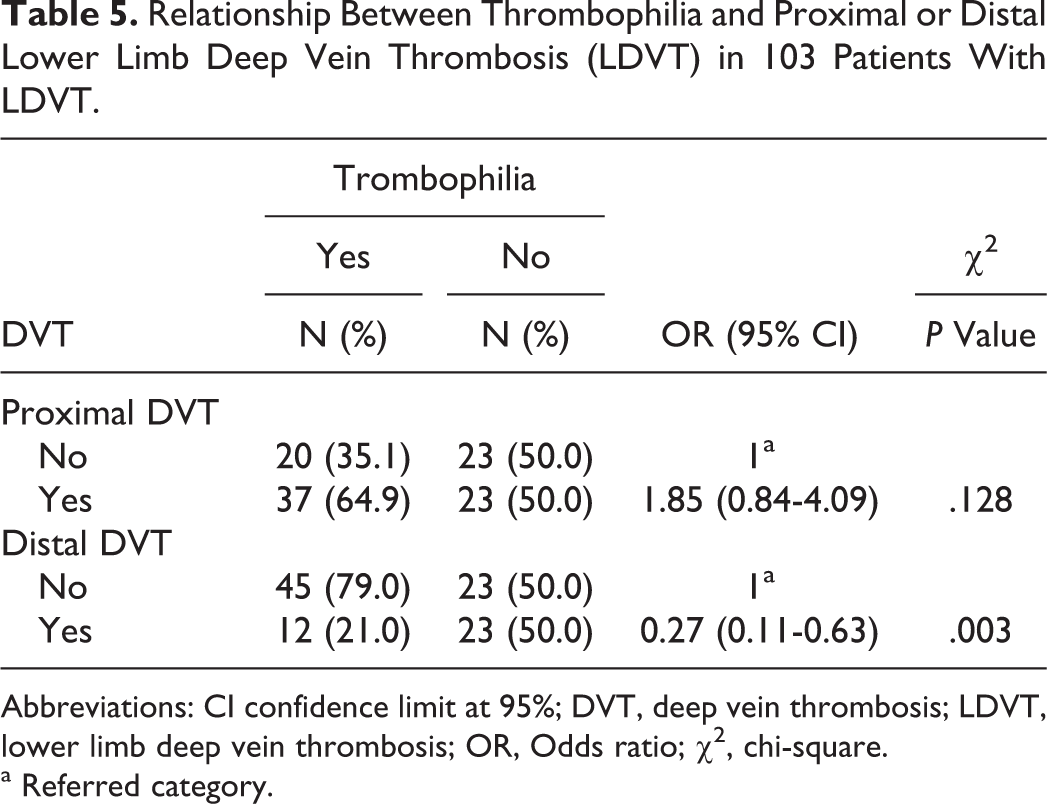
Abbreviations: CI confidence limit at 95%; DVT, deep vein thrombosis; LDVT, lower limb deep vein thrombosis; OR, Odds ratio; χ2, chi-square.
a Referred category.
Relationship Between Thrombophilic Factors and Proximal Lower Limb Deep Vein Thrombosis.
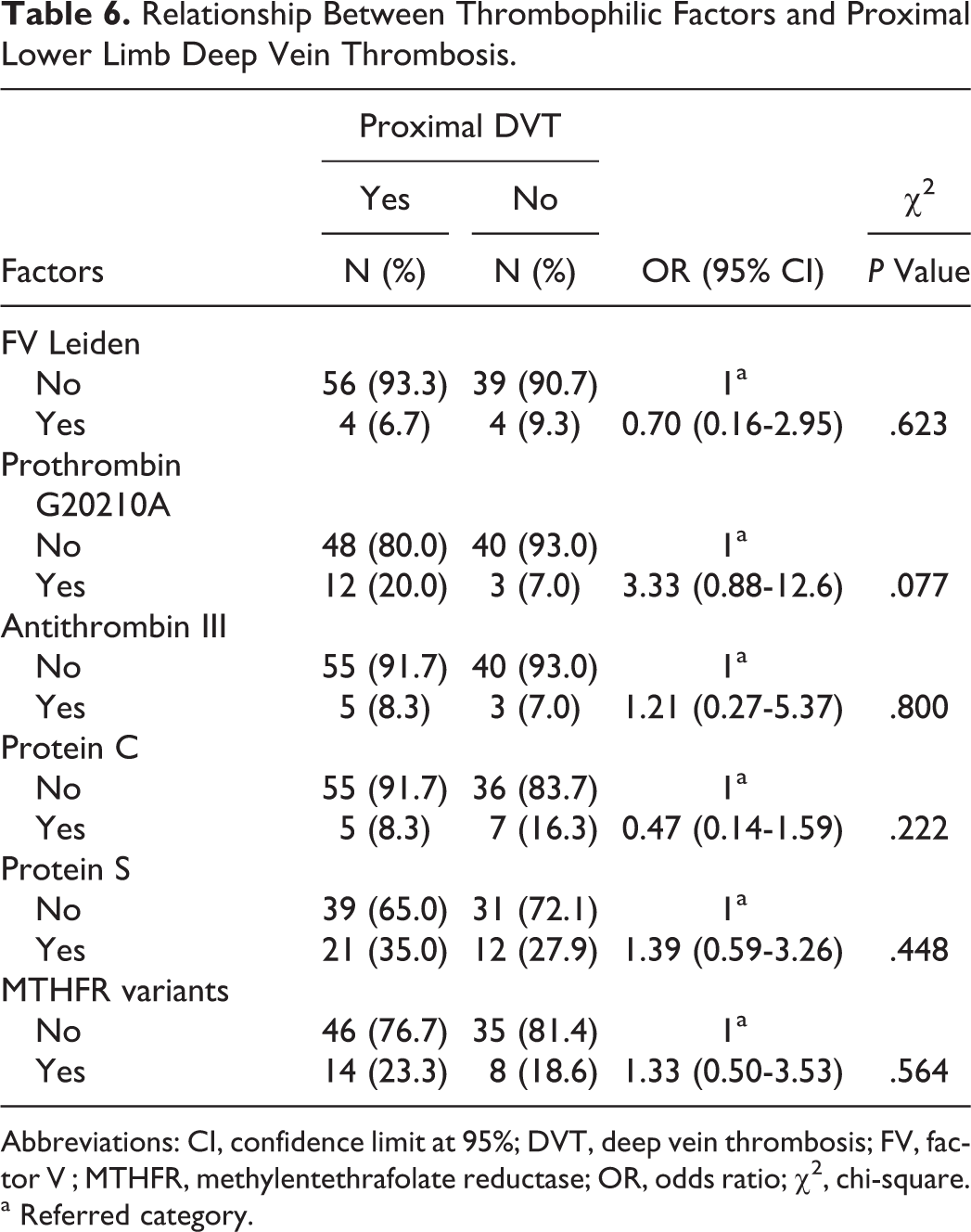
Abbreviations: CI, confidence limit at 95%; DVT, deep vein thrombosis; FV, factor V ; MTHFR, methylentethrafolate reductase; OR, odds ratio; χ2, chi-square.
a Referred category.
Relationship Between Thrombophilic Factors and Distal Lower Limb Deep Vein Thrombosis.
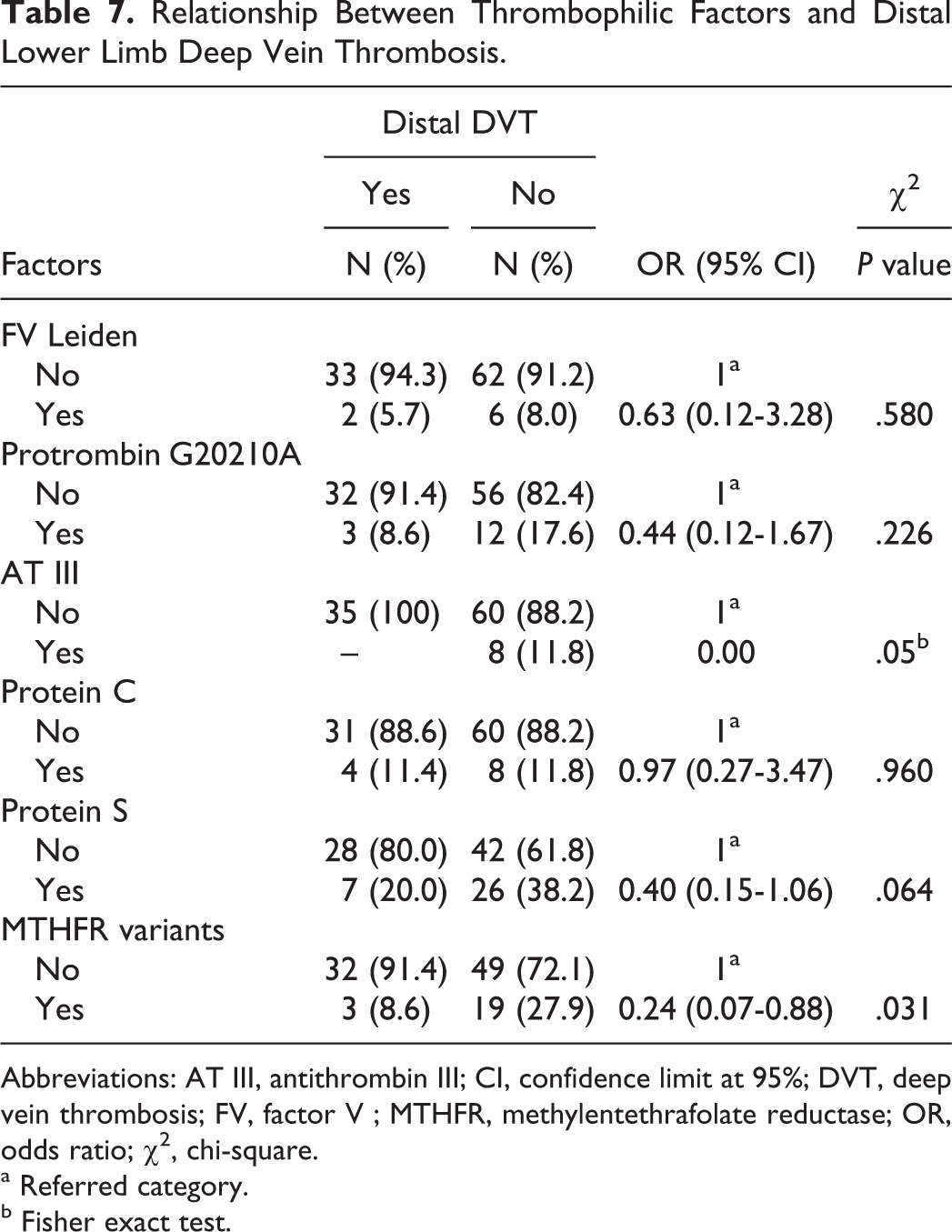
Abbreviations: AT III, antithrombin III; CI, confidence limit at 95%; DVT, deep vein thrombosis; FV, factor V ; MTHFR, methylentethrafolate reductase; OR, odds ratio; χ2, chi-square.
a Referred category.
b Fisher exact test.
Discussion
Lower limb deep vein thrombosis represents the most common venous thrombotic disease and its sequel as postthrombotic syndrome and chronic thromboemebolic pulmonary hypertension are 2 relevant clinical problems. Therefore, identifying patients with high-risk LDVT is the primary goal of the health practitioners. This is done by searching for procoagulative status by screening for different thrombophilic markers, and this is considered as an intriguing and very interesting tool. In order to identify an emerging risk of VTE and LDVT, we considered both environmental situations (age, immobilization, trauma, recent surgery, pregnancy and/or puerperium, contraception, cardiac chronic disease) and genetic predisposition demonstrated by deficiency of anticoagulant markers (antithrombin III, Prot C, and Prot S) and/or the presence of peculiar thrombophilic markers (FVL and prothrombin G20210A gene polymorphism). Data furnished from clinical and epidemiological researches show a low frequency of deficiency of natural anticoagulant proteins (<0.5% in general population), 11 but more severe procoagulative traits can be used to explain the 5- to 10-fold increased risk of VTE. 12 –14 Conversely, the prevalence of FVL and prothrombin G20210A gene polymorphism is up to 5% in the general population and raises up to 50% in patients with VTE. 15 –17 However, whether thrombophilic abnormalities impact on the development of VTE remain an unclear and debated question to date. This question concerns whether inherited thrombophilia could be found in a large part of patients with LDVT. It also concerns the clinical role of thrombophilia because such thrombophilic conditions are rare but result as severe traits of thrombotic events; differently, more common genetic variants are associated with a low thrombotic risk. 18 –22 The role played by thrombophilic disorders is assessed by evaluating both clinical conditions of patients and specific situations that increase thrombotic risk. When screening for inherited thrombophilia in general population, this could be no effective in eliciting the susceptibility to LDVT. Furthermore, results from the RIETE 9 registry stated that indiscriminate application of thrombophilia tests is useful in clinical practice and that they are indicated only in patients with a suspected risk of recurrent VTE (or LDVT). Another previous and complete review summarized that screening should be limited to patients for whom clinical choices may be affected by positive results or to patients with yet known thrombotic defects and, finally, to patients with early-onset or idiopathic venous thrombotic events or when the venous disease involves unusual sites. 19 We performed a study aiming to demonstrate both frequency of thrombophilic disorders and relationship between thrombophilia and its markers with proximal and distal LDVT. In our study, thrombophilia was frequently found. In fact, nearly 55% of the patients with LDVT demonstrated one or more of factors for inherited thrombophilia, and prot S anticoagulant deficiency was the most frequent defect (found in 32% of our patients with LDVT). In this study, we also found a high frequency of the MTHFR homozygous variant (21% of the patients with LDVT). Furthermore, we found a significant frequency of both G20210A prothrombin variant (almost 50% of the patients with LDVT) and prot C anticoagulant deficiency (12% of the patients with LDVT). Based on these findings we concluded that in our study thrombophilia was highly frequent. With the exception of a slight correlation between MTHFR homozygous mutation and distal LDVT which in our experience is less frequent than proximal (proximal 37 Vs distal 12), our study demonstrates that none of the factors that screened inherited thrombophilia show a direct and significant relationship with LDVT, both proximal and distal. Our findings agree with other previous opinions on the usefulness of large screening, and we believe that a generic genetic screening on thrombophilia is not helpful to elicit the emerging risk of LDVT. 21 –24 The main limitations of our study are that it is a monocentric survey performed on a small cohort of consecutive outpatients with LDVT, but its advantage is that it is focused only on LDVT which is the most common and easily diagnosed clinical picture of VTE. The major part of research focused on thrombophilia in VTE as a general question, and some researches highlighted the role played by hypercoagulative states in DVT of upper limbs, which shows a lower frequency compared to LDVT or PE. 25 –30 Differently, a few and recent studies were strictly focused only on the relationship between thrombophilia and LDVT only. 1 –30 The individuation of the predisposing factors for LDVT is yet a relevant clinical question in order to screen the emerging risk, to lower its morbidity, and finally to manage the affected patients. An ideal thrombophilic screening should be able to stratify the risk and also to lead both useful prophylaxis and treatment. Our findings suggest that an indiscriminate screening of inherited thrombophilia is not helpful in LDVT. Furthermore, it is known that many environmental factors have to be considered in the pathogenesis of LDVT. Our results demonstrate that none of the factors shows a strong direct and positive relationship with LDVT. Hence, our study, which was strictly focused on LDVT, can be considered as an added proof to the fact that large screening for thrombophlia is not helpful in eliciting the risk of LDVT.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.