
Abstract
Objectives: The neutrophil to lymphocyte ratio (NLR) has been investigated as a new predictor for cardiovascular risk. Admission NLR would be predictive of adverse outcomes after primary angioplasty for ST-segment elevation myocardial infarction (STEMI). Methods: A total of 2410 patients with STEMI undergoing primary angioplasty were retrospectively enrolled. The study population was divided into tertiles based on the NLR values. A high NLR (n = 803) was defined as a value in the third tertile (>6.97), and a low NLR (n = 1607) was defined as a value in the lower 2 tertiles (≤6.97). Results: High NLR group had higher incidence of inhospital and long-term cardiovascular mortality (5% vs 1.4%, P < .001; 7% vs 4.8%, P = .02, respectively). High NLR (>6.97) was found as an independent predictor of inhospital cardiovascular mortality (odds ratio: 2.8, 95% confidence interval: 1.37-5.74, P = .005). Conclusions: High NLR level is associated with increased inhospital and long-term cardiovascular mortality in patients with STEMI undergoing primary angioplasty.
Introduction
The integral role of inflammation in coronary artery disease has been recognized. 1 Leukocytes play a major role in this inflammatory process. 2 The relationship between white blood cell (WBC) count and increased cardiovascular risk is well known. 3 –5
Recently, neutrophil to lymphocyte ratio (NLR) has emerged as a potent composite inflammatory marker, with higher levels associated with increased mortality in noncardiac disorders. 6 It has also been studied as a prognostic marker in patients undergoing percutaneous coronary intervention (PCI). 7 The aim of this study is to test the hypothesis that higher levels of admission NLR are associated with risk of inhospital and long-term cardiovascular mortality after primary PCI for ST-segment elevation myocardial infarction (STEMI) in a large population.
Methods
Patient Populations
In a retrospective study, 2620 consecutive patients with STEMI presenting at the institution of Siyami Ersek Thoracic and Cardiovascular Surgery Center, Training and Research Hospital between October 2003 and March 2008 were included. The study inclusion criteria were as follows: electrocardiogram (ECG) revealing STEMI, defined as >30 minutes of continuous typical chest pain and ST-segment elevation ≥1 mm in 2 contiguous electrocardiography leads or presumed new left bundle-branch block with cardiac enzymes above twice the upper normal limit within 12 hours of symptom onset or up to 18 hours if there was evidence of continuing ischemia or hemodynamic instability. 8
Of all, 210 patients were excluded due to missing or unavailable data about admission neutrophil and lymphocyte values (n = 136) and admission cardiogenic shock (n = 74). Therefore, the final study population consisted of 2410 patients. The study population was divided into tertiles based on admission NLR values. A high NLR group (n = 803) was defined as a value in the third tertile (>6.97), and a low NLR group (n = 1607) was defined as a value in the lower 2 tertiles (≤6.97).
All primary PCI procedures were performed in a single high-volume tertiary center (>3000 PCI/year) by expert operators performing >75 PCI/year. The study protocol was approved by the hospital’s ethics committee.
Analysis of Patient Data
The patients’ demographic information, cardiovascular history, and risk factors (smoking, hypercholesterolemia, hypertension, and diabetes mellitus [DM]) were obtained from the medical records. Reperfusion time and door-to-balloon time were also determined.
On admission, venous blood was obtained from all the patients. Neutrophils, lymphocytes, and WBC were measured as part of the automated complete blood count using a Coulter LH 780 Hematology Analyzer (Beckman Coulter Ireland Inc, Mervue, Galway, Ireland). The NLR was calculated as the ratio of the neutrophils and lymphocytes, both obtained from the same automated blood sample at admission of the study. A 12-lead ECG was recorded in each patient just after hospital admission, and also myocardial infarction type was recorded from ECG. The glomerular filtration rate (GFR) was estimated by the simplified modification of diet in renal disease (MDRD) equation. 9,10
Coronary Angiography, Primary Angioplasty, and Stenting
All patients received chewable 300 mg aspirin and clopidogrel (300mg loading dose) before coronary angiography. Angiographic data of the patients were evaluated from catheter laboratory records. Emergency coronary angiography and angioplasty were performed by the percutaneous femoral approach. Heparin (10 000 IU) was administered when arterial access was secured. After visualizing the left and right coronary arteries, 2.5 mg of nitrate was selectively injected into the infarct-related artery (IRA) to rule out possible coronary spasm. Angiographic assessments were made by visual assessment. Primary angioplasty including balloon angioplasty and/or stent implantation was performed only for IRA according to the lesion type. For each procedure, interventional success at the acute phase is defined as reducing to <50% of obstruction and stenosis of the IRA with thrombolysis in myocardial infarction (TIMI) 2 or 3 flow just after primary angioplasty. 11 After angioplasty, all patients were admitted to the coronary care unit, where 100 mg aspirin and 75 mg clopidogrel were continued in all patients. The use of glycoprotein IIb/IIIa inhibitors was left to the discretion of the operator. Concomitant medical treatment with β-blockers, angiotensin-converting enzyme inhibitors, and statins were prescribed according to American College of Cardiology/American Heart Association guidelines.
Definition
Time to reperfusion was measured as the time from symptom onset to the coronary reperfusion obtained with balloon inflation. Door-to-balloon time was defined as the time between hospital admission and balloon inflation. Patients were evaluated according to Killip clinical examination classification. 12 Advanced heart failure was defined as New York Heart Association classification ≥3. Anemia was defined as a baseline hemoglobin concentration <13 mg/dL in men and <12 mg/dL in women (World Health Organization definition). 13
Renal failure was defined as a GFR<60 mL/min per 1.73 m2, which was estimated by the simplified MDRD equation. 9,10 Patient with DM was defined as the patient with documented DM using either oral hypoglycemic agents or insulin treatment at admission.
Cardiovascular death was defined as unexplained sudden death, death due to AMI, heart failure, or arrhythmia. Repeat target vessel revascularization (TVR) was defined as need of PCI or coronary surgery because of restenosis or reocclusion of the IRA. Reinfarction was described as elevation of serum creatine kinase MB (CK-MB) enzyme levels by 2 times of the upper limit of normal and ST-segment re-elevations.
Follow-Up
Follow-up data were obtained from hospital records or by interviewing with (directly or by telephone) patients, their families, or their personal physicians. Major adverse cardiac events (MACEs) were defined as cardiovascular death, reinfarction, or repeat TVR (percutaneous or surgical). Only cardiovascular mortality was recorded.
Statistical Analysis
Quantitative variables were expressed as mean value ± standard deviation, and qualitative variables were expressed as percentage (%). Comparison of parametric values between 2 groups was performed by means of 2-tailed Student t test. Categorical variables were compared by the likelihood-ratio χ2 test or Fisher exact test. A backward stepwise multivariate logistic regression analysis that included variables with P < .1 was performed to identify independent predictors of inhospital cardiovascular mortality.
Age ≥70, female gender, DM, renal failure (GFR <60 mL/min per 1.73 m2), 3-vessel disease, unsuccessful procedure, tirofiban use, Killip class 2/3, MI history, and NLR >6.97 were entered into the model. The cumulative survival curves for cardiovascular mortality were constructed with the use of the Kaplan-Meier method with differences assessed with the log-rank test. A P value <.05 was considered statistically significant. All statistical studies were carried out with SPSS program (version 15.0, SPSS, Chicago, Illinois).
Results
Baseline Characteristics
The baseline characteristics are listed in Table 1. The high NLR group was older than low NLR group (mean age 57.5 ± 11.9 vs 55.9 ± 11.7, P = .003). Compared to low NLR group, DM and higher Killip class at admission were more prevalent in high NLR group. Hypertension, current smoker, and female gender were not statistically different between the 2 groups
Baseline Characteristics of Study Patients.
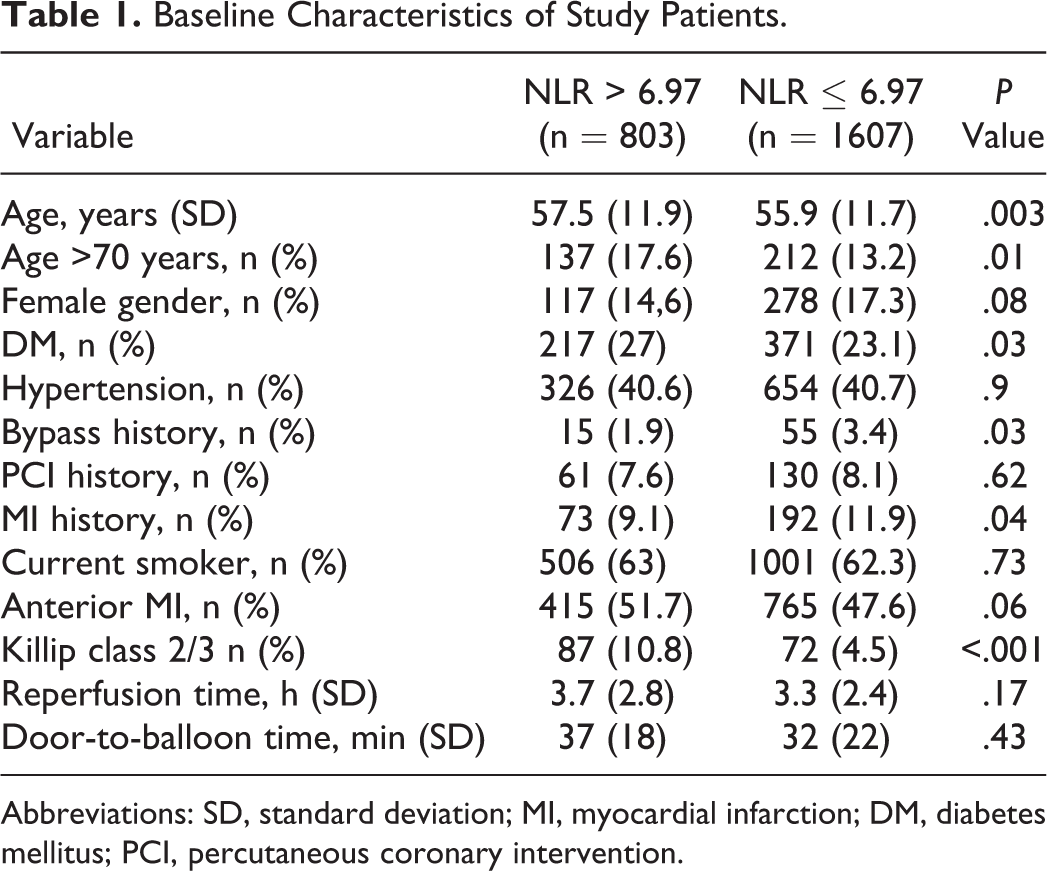
Abbreviations: SD, standard deviation; MI, myocardial infarction; DM, diabetes mellitus; PCI, percutaneous coronary intervention.
Laboratory Findings
Table 2 lists the patients’ laboratory data. Basal renal failure was more frequent in the high NLR group. Baseline leukocyte and neutrophil values were higher in high NLR group (14.23 ± 4.15 vs 11.65 ± 3.36 × 109/L, P < .001; 12.34 ± 3.66 vs 8.07 ± 2.9 × 109/L, P < .001, respectively). Baseline lymphocyte values were also lower in high NLR group (1.22 ± 0.42 vs 2.16 ± 0.76 × 109/L, P < .001). A higher enzymatic peak, admission blood glucose, and creatinine values were also observed in the high NLR group.
Laboratory Findings of Patients.
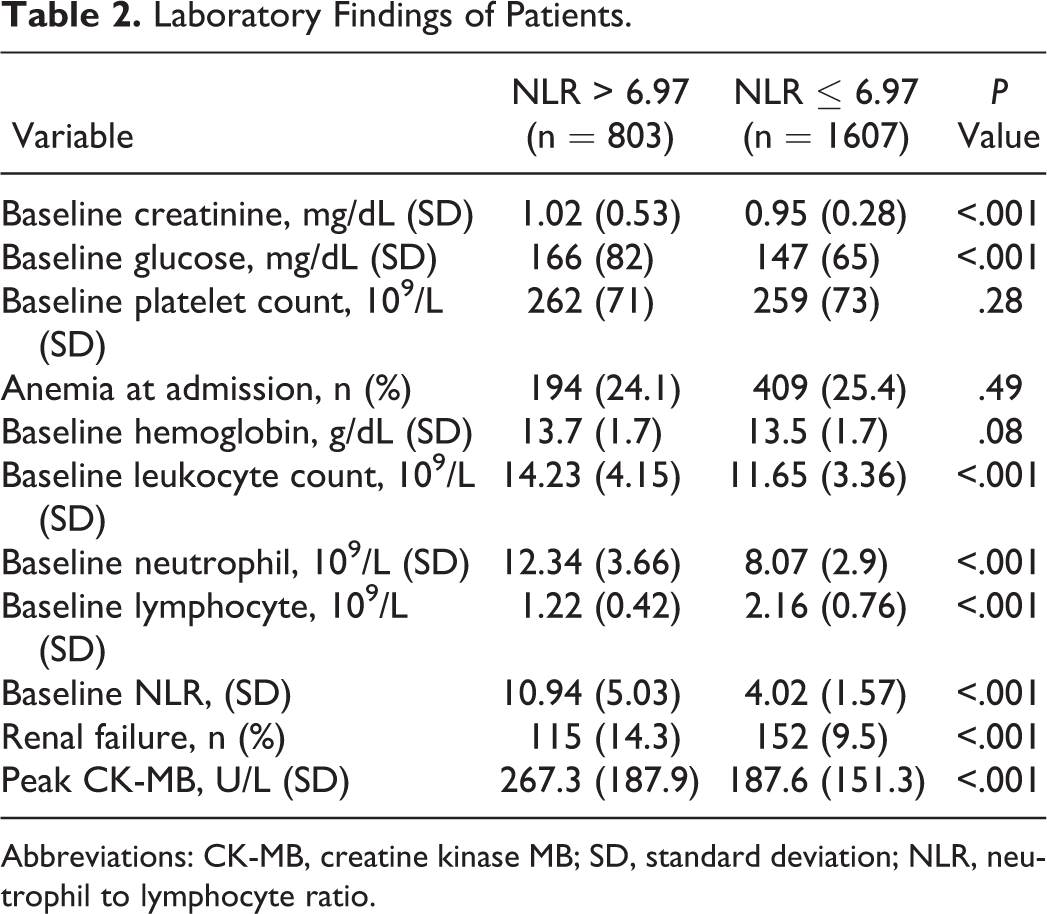
Abbreviations: CK-MB, creatine kinase MB; SD, standard deviation; NLR, neutrophil to lymphocyte ratio.
Angiographic and Procedural Characteristics
Angiographic and procedural characteristics are depicted in Table 3. Culprit lesions were similar in the 2 groups. Stent use, number of diseased vessels, and tirofiban use were not statistically different between the 2 groups. Postprocedural TIMI 3 flow ratio was less in patients with high NLR.
Angiographic and Procedural Characteristics of Patients.
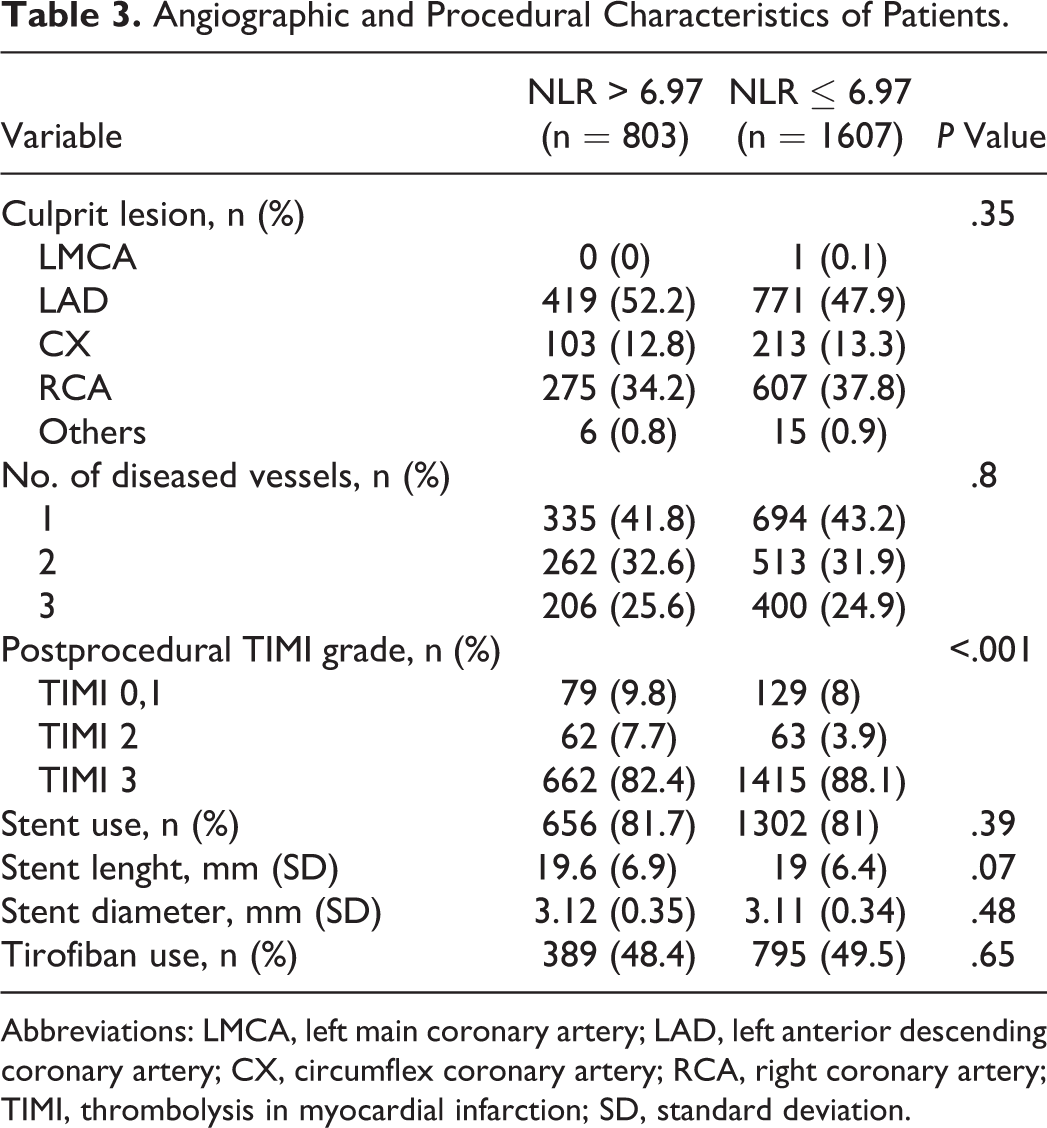
Abbreviations: LMCA, left main coronary artery; LAD, left anterior descending coronary artery; CX, circumflex coronary artery; RCA, right coronary artery; TIMI, thrombolysis in myocardial infarction; SD, standard deviation.
Inhospital and Long-Term Outcomes
Table 4 presents the inhospital and long-term outcomes after primary PCI. High NLR group had significantly higher incidence of inhospital cardiovascular mortality than low NLR group (5% vs 1,4%, respectively, P < .001). The MACE and advanced heart failure were more frequent in patients with high NLR values. Time of hospital stay was significantly higher in the high NLR group (7.5 ± 4.3 vs 6.9 ± 3.6 days, P = .001). Independent predictors of inhospital cardiovascular mortality were determined by a backward stepwise multivariate logistic regression analysis. These predictors of inhospital cardiovascular mortality are depicted in Table 5. Killip class 2/3 at admission, renal failure, age >70 years, DM, unsuccessful procedure, and NLR >6.97 were found to be independent predictors of inhospital cardiovascular mortality.
Inhospital and Long-Term Cardiac Events of All Study Patients.
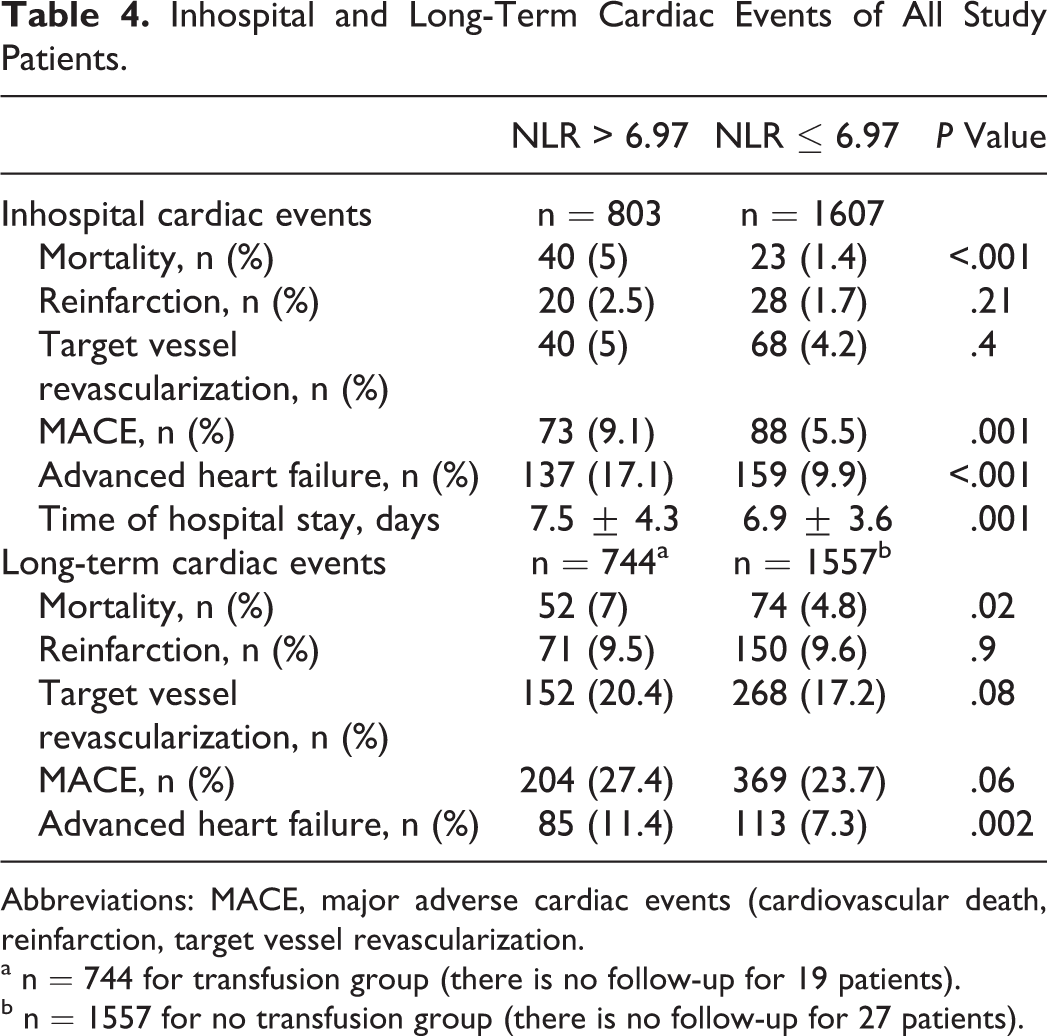
Abbreviations: MACE, major adverse cardiac events (cardiovascular death, reinfarction, target vessel revascularization.
a n = 744 for transfusion group (there is no follow-up for 19 patients).
b n = 1557 for no transfusion group (there is no follow-up for 27 patients).
Independent Predictors of Inhospital Cardiovascular Mortality.
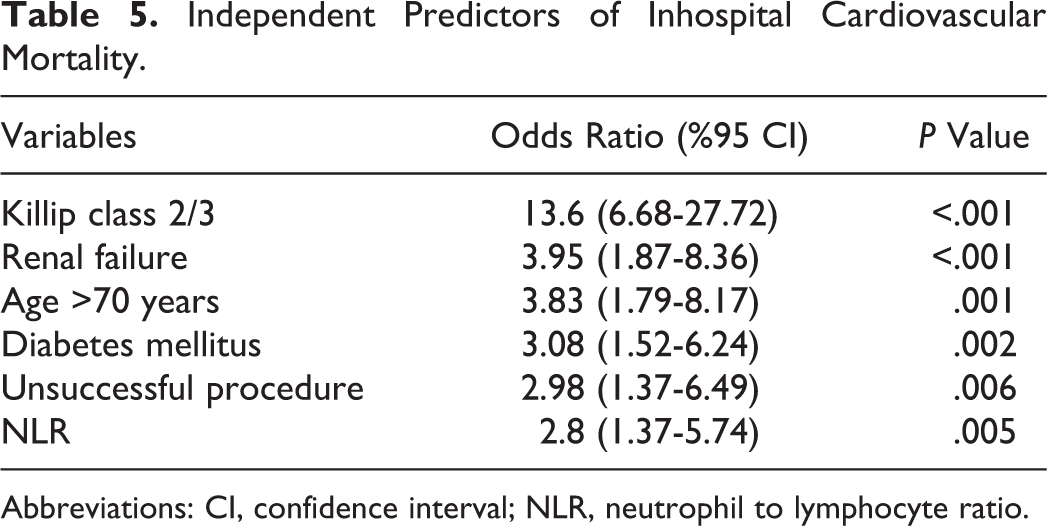
Abbreviations: CI, confidence interval; NLR, neutrophil to lymphocyte ratio.
The median follow-up time was 21 months. Follow-up data after discharge were not obtained for 19 patients (2.3%) high NLR group and 27 patients (1.6%) low NLR group. Long-term cardiovascular mortality and advanced heart failure rates were significantly higher in patients with high NLR values. (7% vs 4.8%, P = .02; 11.4% vs 7.3%, P = .002, respectively). The Kaplan-Meier survival plot for cardiovascular mortality in both the groups is presented in Figure 1.
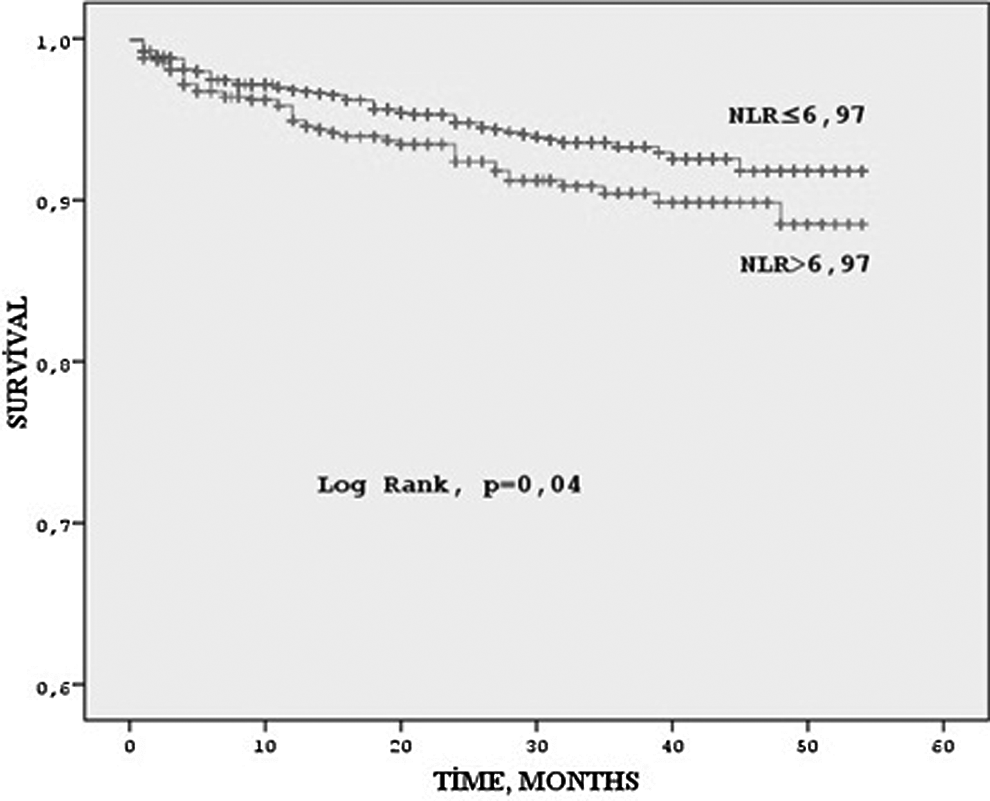
Kaplan-Meier curve for long-term survival according to high versus low neutrophil to lymphocyte ratio (NLR) groups.
Discussion
The main findings of the present single-center study are as follows: (1) patients in the high NLR group were older and had higher prevalence of DM, renal failure, advanced Killip class, and poor reperfusion; (2) high NLR is associated with a remarkable increase in inhospital and long-term cardiovascular mortality; and (3) after adjustment for potential confounders, high NLR was one of the independent predictors of inhospital cardiovascular mortality.
Leukocytosis is one of the common findings in acute STEMI. Leukocytes infiltrate the damaged and necrotic tissue. In particular, neutrophils are the first type of leukocytes. Neutrophilia reflects the systemic inflammatory status, and neutrophils secrete many enzymes such as elastase, myeloperoxidase, oxygen-free radicals, and acid phosphatases that further contribute to tissue damage. 14 –16 In addition, increased neutrophil–platelet aggregates could be seen in microcirculation, leading to the no-reflow phenomenon, larger infarct size, and poor prognosis. 17 –19 In acute conditions, lymphopenia, especially low CD4+ during stress response, is another common finding, and it is associated with poorer prognosis after STEMI. 20 Regulatory CD4+ T cells have decreased response to increased oxidized low-density lipoprotein and cortisol secretions. 20,21 In addition, lymphopenia is observed in inflammatory states because of increased lymphocyte apoptosis. 22 Apoptotic cells contribute to proinflammatory cytokine secretion. 23 In 2 studies, lymphopenia was found to be related to mortality after STEMI. 24,25
Over the last few years, studies have focused on the association of NLR and STEMI. In 2007, Takahashi et al 26 found that neutrophilia on admission was associated with impaired microvascular reperfusion and poor functional recovery after primary PCI in 116 patients. This study population was small and limited to patients with anterior STEMI. Furthermore, there was no follow-up. In another small study by Li et al, 27 higher neutrophil counts, NLR, and levels of high-sensitivity C-reactive protein were found to be predictors of thrombus formation in patients with STEMI. Takahashi et al 28 examined the neutrophil count in 228 adult patients with STEMI who underwent primary PCI and showed that neutrophilia on admission was associated with impaired microvascular perfusion, left ventricular dilatation, and long-term MACE. Núñez et al 29 showed through a study of 470 patients with STEMI that the maximum NLR value is a useful marker for predicting mortality; however, the primary PCI ratio was only 3.8% in this study. Recently, Lee et al 30 reported that increased NLR was an independent predictor of MACE in diabetic patients presenting with acute myocardial infarction; in their study, there were 2559 patients with STEMI, and they obtained data on revascularization with either thrombolytic therapy or primary PCI. Chia et al 31 evaluated 363 patients who underwent primary PCI and found that elevated leukocyte and neutrophil counts were related to myocardial infarct size and poor 6-month cardiovascular events. Kruk et al 32 reported that high-sensitivity C-reactive protein and the WBC count were predictors of inhospital death in 1078 patients with STEMI admitted for primary PCI. Cho et al 33 examined 739 patients undergoing primary PCI. The higher NLR group had higher mortality at 6 months. They excluded cardiogenic shock, as in our study.
Not surprisingly, the NLR levels were higher in older patients in our study. This was because older patients more commonly had a higher inflammatory burden, hypertension, anemia, bad nutritional status, and age-associated diseases including DM and renal failure. Higher DM, renal failure, and admission blood glucose were more commonly observed in patients with high NLR. These findings correlated with the study by Cho et al. 33 Neutrophilia in DM is probably due to increased plasma cortisol, leptin, and insulin levels. In addition, advanced glycation end products, oxygen free radicals, and cytokines might contribute to high NLR in diabetic patients. 30 Nonetheless, NLR was an independent predictor of mortality after adjusting for these confounding factors.
Madjid et al 34 reported that neutrophils can obstruct capillaries in coronary microcirculation, aggravate ischemia, and extend the infarct area. Oxidative and proteolytic injury by neutrophils contribute to infarct expansion. Furthermore, distal embolization of leukocytes might reduce coronary flow. These can explain the correlation between NLR and the infarct size as measured by the peak CK-MB. 32 Mariani et al 35 showed a significant relationship between neutrophil counts and reperfusion after primary PCI. In another study, Barron et al 5 found a correlation between neutrophilia and myocardial infarct expansion that is related to the early development of congestive heart failure. These findings are all compatible with our study that reports higher enzymatic peak, poorer reperfusion, and worse inhospital and long-term cardiac events in the high NLR group.
Study Limitations
This study carries the well-known limitations of the retrospective design, and it is a single-center study. It is nonrandomized and thus subject to selection bias. However, we were careful to include consecutive patients. Reperfusion markers such as myocardial blush grade or ST-resolution could not be determined. We did not look at high-sensitivity C-reactive protein, B-type natriuretic peptide, other proinflammatory cytokines, and markers of oxidative stress. Despite adjusting for multiple risk factors, it is possible that there might have been residual confounding conditions and medications. We have no data on any changes in NLR levels during the course of hospital stay. In addition, we did not examine leukocyte and lymphocyte subtypes.
Conclusion
This study was conducted in a large primary PCI population, and it showed that patients with high NLR had worse clinical outcomes and higher mortality, both inhospital and over a long-term period, than patients with low NLR. In summary, NLR is an inexpensive and powerful prognostic factor in patients undergoing primary PCI for STEMI. We hope that this study will stimulate a prospective investigation, including all confounding factors, in patients with STEMI.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.