
Abstract
Introduction:
Despite various guidelines for venous thromboembolism (VTE) prevention, malpractice in prescribing thromboprophylaxis is common. In this study, factors associated with prescribing or not prescribing appropriate chemical thromboprophylaxis were assessed.
Materials and methods:
We enrolled high-risk patients for VTE (based on Caprini score) in the general surgery ward. They were divided into 2 groups based on receiving appropriate prophylaxis or not. Factors associated with prescribing thromboprophylaxis were analyzed.
Results:
A total of 613 patients were enrolled in this study. Head and neck operations (P < .0001), minor surgeries (P = .001), mastectomy (P = .012), and medical treatment (P = 0.034) were the factors associated with not prescribing thromboprophylaxis. In contrast, age (P < .0001), laparoscopic surgeries (P = .011), surgery duration (< .0001), oral contraceptive pill consumption (P = .005), and complete bed rest (P = .002) were protective factors.
Conclusion:
Minor surgeries, head and neck operations, mastectomy, and medical treatment are associated with overlooking anticoagulant administration. It is recommended to consider aforementioned pitfalls in routine practice and education.
Introduction
One of the most threatening and also common complications of general surgery is deep vein thrombosis (DVT). It can lead to pulmonary embolism (PE) with mortality rate up to 18%. 1 –3 It is estimated that 3 00 000 patients die due to venous thromboembolism (VTE) annually in the United States. 4
To provide adequate preventive measures, it is mandatory to thoroughly assess each patient’s DVT risk factors. 5 –7 There are many guidelines with regard to thromboprophylaxis, such as the American College of Chest Physicians and the Caprini risk assessment model that introduce risk factors and guide the practitioners to use appropriate prophylaxis. 6,8 –10 Despite existence of such guidelines, there are still several reports revealing that the current practice has deviated from these guidelines. It is possible that some factors affect appropriateness of thromboprophylaxis in patients who are hospitalized. 11
The goal of the present study was to compare thrombotic risk factors in 2 groups of surgical patients with appropriate and inappropriate administration of chemical thromboprophylaxis. The findings would suggest which factors are unnoted and need to be emphasized more in educating physicians.
Materials and Methods
This study was carried out between April 2011 and October 2011 in Shariati hospital affiliated to Tehran University of Medical Sciences. The hospital research committee approved the study protocol. All patients filled in an informed written consent form to participate in the study. Inclusion criteria were all patients who admitted in general surgery ward, whether they underwent surgery or not, enrolled consequently in the study to be assessed if they received appropriate prophylactic anticoagulant or not. Patients who did not have risk factors to receive chemical prophylaxis (Caprini score <3) were excluded from the study. Also, patients who were under anticoagulant therapy due to an underlying condition (such as previous VTE, cardiovascular disease, mechanical heart valve) were excluded. Demographic information, therapeutic procedures, risk factors for VTE which were mentioned by Caprini, 5 and chemical thromboprophylaxis administration were obtained during data collection. Data collection were done on the day of discharge mainly by reviewing patients’ medical charts. Related forms were completed by a trained physician who asked each patient supplementary questions.
A ward protocol was present for VTE prophylaxis based on the Caprini risk factor assessment and through the previous 2 years, all physicians received education every 6 months. Patients were visited by surgical residents under direct supervision of attending faculty. In this study, all nurses and physicians were blinded. Early ambulation strategy was generally conducted for all patients in the ward. Graduated compression stockings were also used for patients with moderate to high risk for VTE (Caprini score ≥2). Intermittent pneumatic compression (IPC) was used for patients with the highest risk (Caprini score ≥ 5) who were admitted to intensive care unit. The protocol recommended administration of 40 mg enoxaparin daily or 5000 units unfractionated heparin thrice daily for indicated patients (Caprini score ≥ 3) as chemoprophylaxis. Although based on Caprini Score, high-risk patients with score 3 to 4 can be treated with IPC or chemical prophylaxis, the hospital protocol has clearly recommended chemical prophylaxis for scores ≥3, due to lack of IPC for all of the patients in this group.
Other patients who had indication for chemical DVT prophylaxis were divided into 2 groups based on receiving appropriate chemical prophylaxis or not. We defined appropriate chemical thromboprophylaxis as receiving drug before and after operation with appropriate dosage and proper length of postoperative administration. Appropriate dosage was considered dosage of 5000 units unfractionated heparin or 40 mg enoxaparin 2 hours before surgery and 5000 units thrice daily for unfractionated heparin and 40 mg per day for enoxaparin postoperatively was considered as appropriate. Proper length of continuing thromboprophylaxis is 7 days for high-risk patients (Caprini score 3-4) and 30 days for very high-risk patients (Caprini score ≥5). 5 By comparing the 2 groups (with and without appropriate chemical prophylaxis), factors which were associated with prescribing anticoagulant regiments were analyzed. Also, we followed up the patients for 3 months to assess whether they sustained VTE. All patients with clinical signs of DVT were assessed by color Doppler sonography of the limb venous system. Patients with suspected pulmonary emboli underwent both color Doppler sonography and pulmonary computed tomography angiography.
We divided treatments into 9 categories for statistical analysis, abdominal surgery (including colectomy, esophagectomy, gastrectomy, liver resection, cholecystectomy, appendectomy, etc), abdominal wall hernia repair, mastectomy, head and neck surgery (eg, thyroidectomy and parathyroidectomy), minor procedures defined as procedures over skin and mucous membranes taking less than 45 minutes (eg, anorectal surgeries, resection of pilonidal sinus, and skin procedures), thoracic surgeries, and medical treatments. Minor procedures were mostly performed under spinal or local anesthesia.
Statistical Analysis
Data were analyzed using SPSS 16.0 for windows (SPSS, Chicago, Illinois). Age, body mass index (BMI), duration of surgery, and Caprini score of patients are expressed as mean ± standard deviation and categorical data are expressed as percentage. Normality of quantitative data distribution was tested by Kolmogorov-Smirnov test. Continuous data with or without normal distribution were tested by Student t test and Mann-Whitney U test, respectively. We analyzed qualitative data using chi-squared test. A P value <.05 was considered statistically significant. Multiple logistic regression (MLR) was used to measure the adjusted odds ratio (OR) for assessing missed thromboprophylaxis with regard to factors which had become significant in univariate analysis (P < .2). Stepwise elimination was done using backward method. Age and BMI were considered as continuous variables and other factors were entered as binary variables. The results of MLR were expressed as P values and OR with 95% confidence interval (CI). We considered P < .05 to be significant.
Results
Totally, 730 patients entered the studyand 117 patients excluded from the study due to score <3 based on the Caprini model (105 cases) or receiving anticoagulant therapy for another indication (12 cases). Among the remaining 613 patients, there were 286 (46.7%) men and 327 (53.3%) women. Mean age was 49.3 ± 15.8 (range: 14-89). Also, mean Caprini score was 5.7 ± 2.6 (range: 3-19). Table 1 compares demographic characteristics between the 2 groups.
Demographic Characteristics in Each Group.
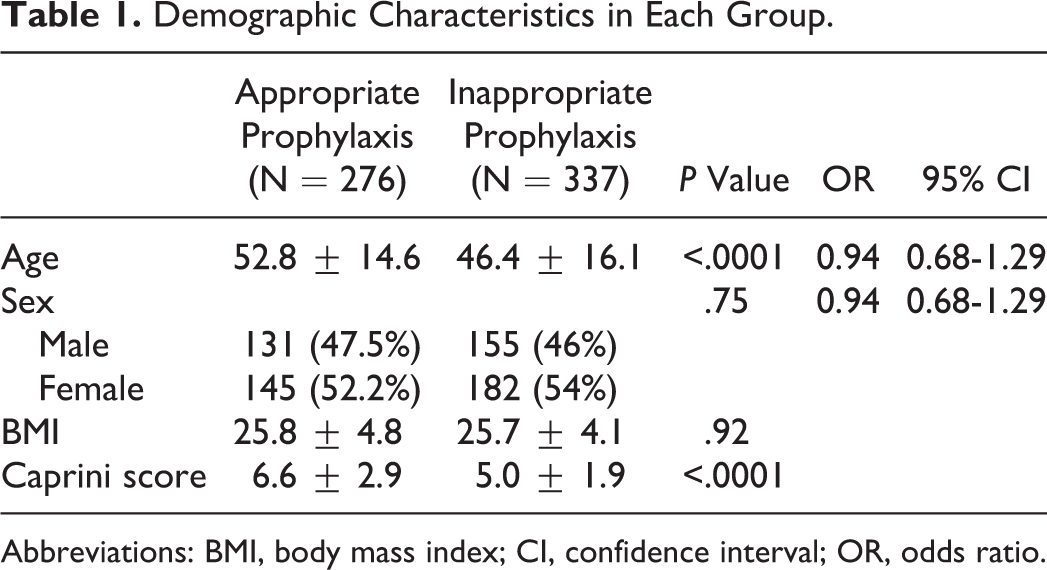
Abbreviations: BMI, body mass index; CI, confidence interval; OR, odds ratio.
Out of the 613 patients who were candidates to receive chemical thromboprophylaxis, 276 (45%) patients received appropriate chemical thromboprophylaxis while 337 (55%) patients did not receive appropriate drug. Patients who received appropriate thromboprophylaxis had higher Caprini score than the other group (6.6 ± 2.9 vs 5.0 ± 1.9, P < .0001).
We performed univariate analysis considering the Caprini factors such as different types of surgeries, age, gender, BMI, duration of surgery, current or history of malignancy, laparoscopic type of surgery, past surgical history, having varicose veins, immobility, central vein catheter, history of DVT in patient or his family, using contraception, pregnancy, and so on. Multivariate analysis of risk factors with P < .2 in univariate analysis was carried out and the result is shown in Table 2. Based on the MLR model, head and neck operations (OR = 2.73; 95% CI: 1.64-4.51), minor surgeries (OR = 3.97; 95% CI: 1.82-8.64), mastectomy (OR = 4.64; 95% CI: 1.41-15.30), and medical treatment (OR = 4.08; 95% CI: 1.11-14.98) were factors associated with not prescribing correct chemical thromboprophylaxis. On the contrary, age (OR = 0.98; 95% CI: 0.96-0.98), laparoscopic surgeries >45 minutes (OR = 0.51; 95% CI: 0.30-0.85), duration of surgery (OR = 0.99; 95% CI: 0.98-0.99), consumption of oral contraceptive pills ([OCPs]; OR = 0.32; 95% CI: 0.14-0.71), and complete bed rest more than 72 hours (OR = 0.36; 95% CI: 0.19-0.69) were protective factors for missing chemical prophylaxis. Table 3 illustrates reduced model after backward stepwise elimination which confirms the aforementioned findings.
Risk Factors in Each Group of Study and Comparison Between Risk Factors Embedded in Multivariate Model.
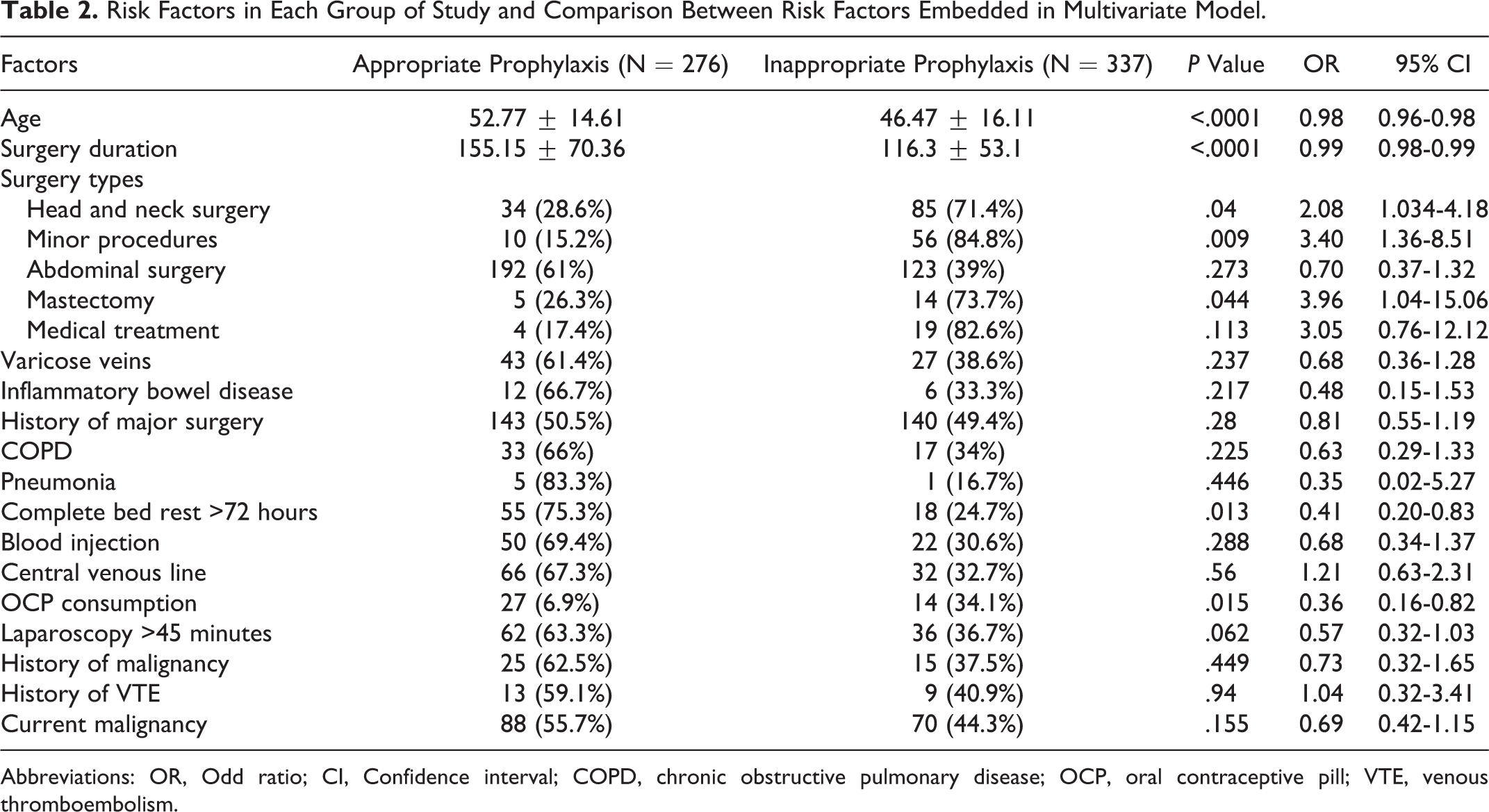
Abbreviations: OR, Odd ratio; CI, Confidence interval; COPD, chronic obstructive pulmonary disease; OCP, oral contraceptive pill; VTE, venous thromboembolism.
Reduced Model in Multivariate Analysis.
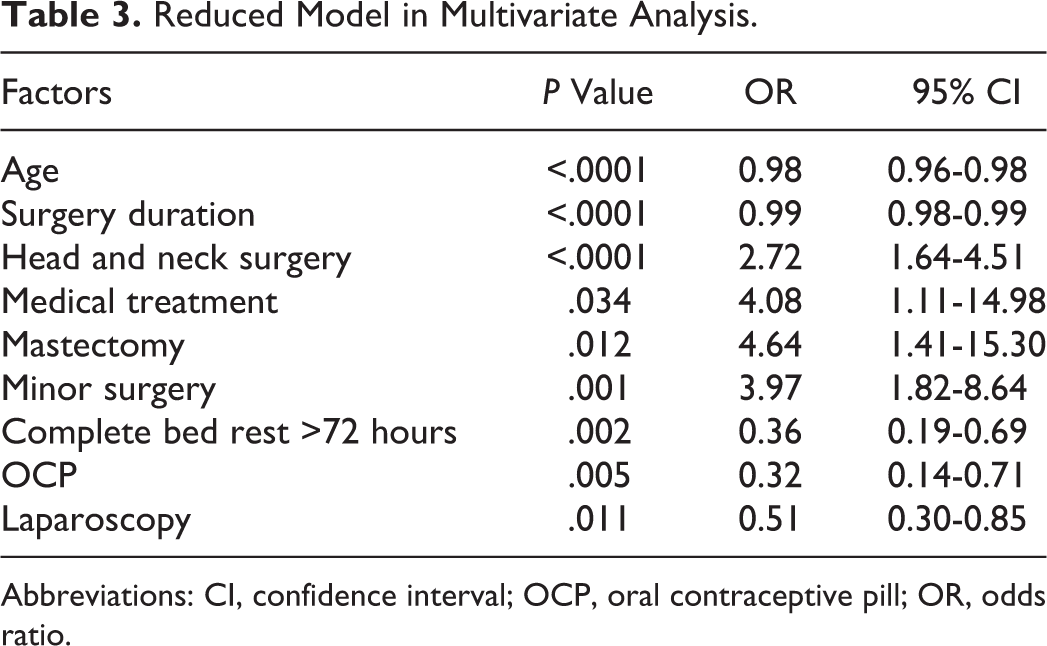
Abbreviations: CI, confidence interval; OCP, oral contraceptive pill; OR, odds ratio.
At 3-month follow-up, 603 (98.4%) patients out of 613 had been assessed. In all, 5 patients had been died (3 due to infectious complications, 1 due to myocardial infarction, and 1 case due to cerebrovascular accident) and 5 patients were lost to follow-up. Out of the 603 patients, 10 (1.7%) patients developed VTE clinically, while 8 (1.3%) patients had not received appropriate thromboprophylaxis, and 2 (0.3%) patients had received appropriate VTE prophylaxis (P = .198, OR = 3.32; 95%CI: 0.70-15.77). None of the patients with VTE died during the follow-up period.
Discussion
Several studies consistently demonstrated that morbidity and mortality of VTE can be diminished by appropriate prescription of prophylactic anticoagulant drugs. 12 –14 Although there are many evidence-based guidelines which show indications and proper usage of prophylactic anticoagulant, 5,6 many studies have revealed high rate of malpractice in using thromboprophylaxis. As a consequence, there are high-risk patients who do not receive any drug for prevention of DVT. 12 –15 Deheinzelin and colleagues showed that 29% to 37% of the surgical patients with moderate to high risk for VTE did not receive any thromboprophylaxis. 12 Amin and colleagues assessed practice of thromboprophylaxis in 227 centers in the United States and showed that just 34% of the patients with an acute medical condition and VTE prophylaxis indication had received appropriate thromboprophylaxis. 16 Our data also showed that only less than half of the patients (45%) had received appropriate chemical thromboprophylaxis. The aforementioned studies show that physicians do not consider all VTE-prone patients for appropriate prophylaxis based on the available guidelines. Besides the evidences that show mortality of VTE can be reduced by appropriate VTE prophylaxis, we can conclude that being not compliant with related guidelines increases the chances of VTE mortality.
In this study, by comparing 2 groups regarding receiving appropriate anticoagulant as a prophylactic measure or not, multivariate analysis suggests that surgeons consider “increasing age,” “immobility,” “laparoscopic surgery,” “use of OCP,” and “ prolonged surgeries” as factors to prescribe prophylactic anticoagulant agents. In other words, by increasing patients’ age and also prolongation of the surgery, the surgeons tend to prescribe chemoprophylaxis more. However, “minor surgeries,” “head and neck operations,” “ mastectomy,” and finally “medical treatment” are the factors associated with not prescribing prophylactic drug, regardless of the existence of other thrombotic risk factors. These findings reveal that kind of surgery or treatment has a crucial effect on physicians’ decision making about administration of thromboprophylaxis. In other words, this factor may distort a physician’s practice by ignoring the other risk factors. For example, physicians often ignore prescribing anticoagulants to patients undergoing minor surgeries without considering the presence of any other risk factors. Noticeably, people with higher Caprini score were more likely to receive proper VTE prophylaxis. This may demonstrate that having fewer risk factors (which causes lower Caprini score) or absence of special risk factors (eg, age, immobility, etc) leads to missing of appropriate anticoagulant prophylaxis.
On the other hand, as this study shows, medical patients are often missed for receiving anticoagulants. Similarly, Ageno showed that a significant proportion of medical patients, being high risk for VTE, had significantly missed the appropriate thromboprophylaxis prescription. 17 Another similar study on acutely ill medical patients showed just 16% of the patients who were candidate to receive VTE prophylaxis, received appropriate preventive treatment. 18
There is a couple of suggested grounds for not prescribing adequate thromboprophylaxis for patients. Basically, there has always been some setback in adapting new guidelines by physicians. 19 As Tooher et al and Michato implied in their studies, existence of perfect guidelines are not sufficient to resolve the issue of not prescribing adequate thromboprophylaxis. They suggested more complex approaches to overcome this problem. 11,20 The other probable reason is not diagnosing or considering VTE risk factors by physicians. This problem can be solved by holding continuous education programs for physicians and medical staffs. 13 Besides, concerns about bleeding and heparin-induced thrombocytopenia as complications of anticoagulant drugs make surgeons more cautious with heparin and similar drugs 12,21,22 which needs intense debate on risk benefit of anticoagulants in educational programs. Having bias toward some risk factors may be another basic problem. Type of surgery is an example since we showed inappropriate prescription of thromboprophylaxis agents in minor surgeries regardless of the existence of other risk factors. So paying attention to all VTE risk factors need to be more emphasized.
After following the patients for 3 months, 8 and 2 patients in inappropriate and appropriate receiving prophylaxis groups developed VTE, respectively. Although not statistically significant (possibly because of low sample size), it shows more VTE in the group without receiving adequate prophylaxis. As Nathens et al showed by even delay to start VTE prophylaxis in high-risk traumatic patients, the risk of VTE rises to 3-fold 23
As it was shown in this study, except some special risk factors (eg, age, immobility, laparoscopic surgeries, duration of surgery, and OCP), others which are mentioned in the Caprini model were not considered by the surgeons. Likewise, factors such as type of surgery are elements that may cause ignorance in anticoagulant prescription, without considering other risk factors. Noteworthy it is possible that due to the presence of numerous risk factors and small sample size for some factors in this study, they were excluded from the analyzing model. As well Kimmerly and colleagues showed that risk factors such as age >40 years, recent myocardial infarction, lupus anticoagulant, varicose veins, and mutation in factor V Leiden have been missed in assessment of thrombotic risks. 1 Other studies have brought up missed risk factors in VTE prophylaxis evaluations such as family history or past history of DVT, history of stillborn, and miscarriage in any trimester. 17,24 –26 Variations about missed factors in different studies are conceivably due to different populations in studies and dissimilar centers with diverse local protocols; hence, it is important to carry out several studies to assess different groups of patients in various kinds of hospitals. Also, different attitudes to VTE in different centers can be the other reason for heterogeneous reports.
The limitations which we encountered in this study included small sample size for some risk factors and limiting the study to general surgery ward. Expansion of such investigations to other surgeries and including medical patients can lead to positive changes in physicians’ attitude and practice. Also, in this study we have considered all of the abdominal surgeries in one category in order to divide procedures based on the anatomical site. However, major abdominal surgeries, such as cancer resections, have been accounted with higher risk for VTE due to current malignancy and longer operation duration.
Conclusion
Minor surgeries, head and neck operations, mastectomy, and not undergoing surgery (medical treatment) may cause overlooking prophylactic anticoagulant administration. Meanwhile, age, immobility, laparoscopic surgeries, duration of surgeries, and using OCP promote chemical thromboprophylaxis prescription. It is recommended to consider aforementioned pitfalls in routine education.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.