
Abstract
Data from the Nationwide Inpatient Sample, 1999 to 2008, were used to assess the effects of advancing age on in-hospital case fatality rate of patients with acute pulmonary embolism (PE) stratified according to stability. Among adults, all-cause case fatality was affected more by advancing age (1.8 deaths/10 years of age) than death attributable to PE (0.7 deaths/10 years of age). All-cause case fatality rate was affected more by advancing age in unstable adults than in stable adults (5.3 deaths/10 years of age vs 1.7 deaths/10 years of age). Case fatality rate attributable to PE was also affected more by advancing age in unstable adults than in stable adults (4.1 deaths/10 years of age vs 0.6 deaths/10 years of age). Limited data suggest that the case fatality rate of children was comparable to that of the elderly individuals. These results may influence the prognostic value of risk assessment tools for patients with PE.
Case fatality rate in patients with acute pulmonary embolism (PE) is recognized to increase with age. 1 –7 It would be more informative to assess the impact of age on case fatality rate in patients with PE stratified according to stability and according to all-cause death or PE attributable to death. Prognosis of PE differs according to whether patients are stable or unstable 8,9 and whether the patients have a primary or secondary diagnosis of PE. 10 The impact of age on all-cause case fatality rate and case fatality rate attributable to PE were assessed in stable and unstable patients with PE using the database of the Nationwide Inpatient Sample (NIS).
Methods
Patients with acute PE discharged from short-stay hospitals throughout the United States from 1999 to 2008 and their in-hospital case fatality rates were identified from the NIS, Healthcare Cost and Utilization Project (HCUP), Agency for Healthcare Research and Quality (AHRQ). 11 The NIS contains data from 5 to 8 million hospital stays from about 1000 hospitals and is designed to approximate a 20% sample of US nonfederal, short-term hospitals.
International Classification of Diseases, Ninth Edition, Clinical Modification (ICD-9-CM) codes were used to identify patients (Table 1). The impact of advancing age on case fatality rates was assessed in patients according to whether they were unstable (shock or ventilator dependent) or stable (not in shock and or ventilator dependent). Within these stratified groups, the effects of advancing age on case fatality rates were further assessed according to sex and race. The definition of “unstable patients” did not include patients with PE who had a high-expected mortality but were not in shock or on ventilatory support.
International Classification of Diseases, 9th Edition, Clinical Modification Codes Used.
Abbreviation: ICD-9-CM, International Classification of Diseases, Ninth Edition, Clinical Modification.
In-hospital all-cause case fatality rates and case fatality rates in patients who had a primary (first-listed) diagnosis of PE and none of the comorbid conditions described in the Charlson Co-morbidity Index 12 were analyzed separately. Deaths in patients with a primary diagnosis of PE and none of these comorbid conditions were assumed to be caused by PE. Conditions included in the Charlson Co-morbidity Index 12 and the ICD-9-CM codes we used to identify these comorbid conditions are shown in Table 2. This method of classifying comorbidity provides a simple, readily applicable, and valid method of estimating the risk of death from comorbid disease. 12
Comorbid Conditions Listed in the Charlson Index 12 in Patients Who Underwent Pulmonary Embolectomy and International Classification of Diseases, Ninth Edition, Clinical Modification Codes Used.
Abbreviations: ICD-9-CM, International Classification of Diseases, Ninth Edition, Clinical Modification; HIV, human immunodeficiency virus; AIDS, acquired immune deficiency syndrome.
Statistical Methods
Case fatality rate was defined as the proportion of patients with PE who died. Linear regression analyses were used to calculate the slopes of the curves. Pearson correlation analyses were performed to assess the extent of dispersion of points around the regression lines, and regression curves were compared using StatTools, Palisade Corporation, Ithaca, New York (www.stattools.net).
Results
All-Cause Case Fatality Rates According to Age
From 1999 to 2008, 2 110 320 patients were discharged from short-stay hospitals in the United States, with a diagnosis of PE. All-cause in-hospital case fatality rate was 187 085 (8.9%). Among adults aged
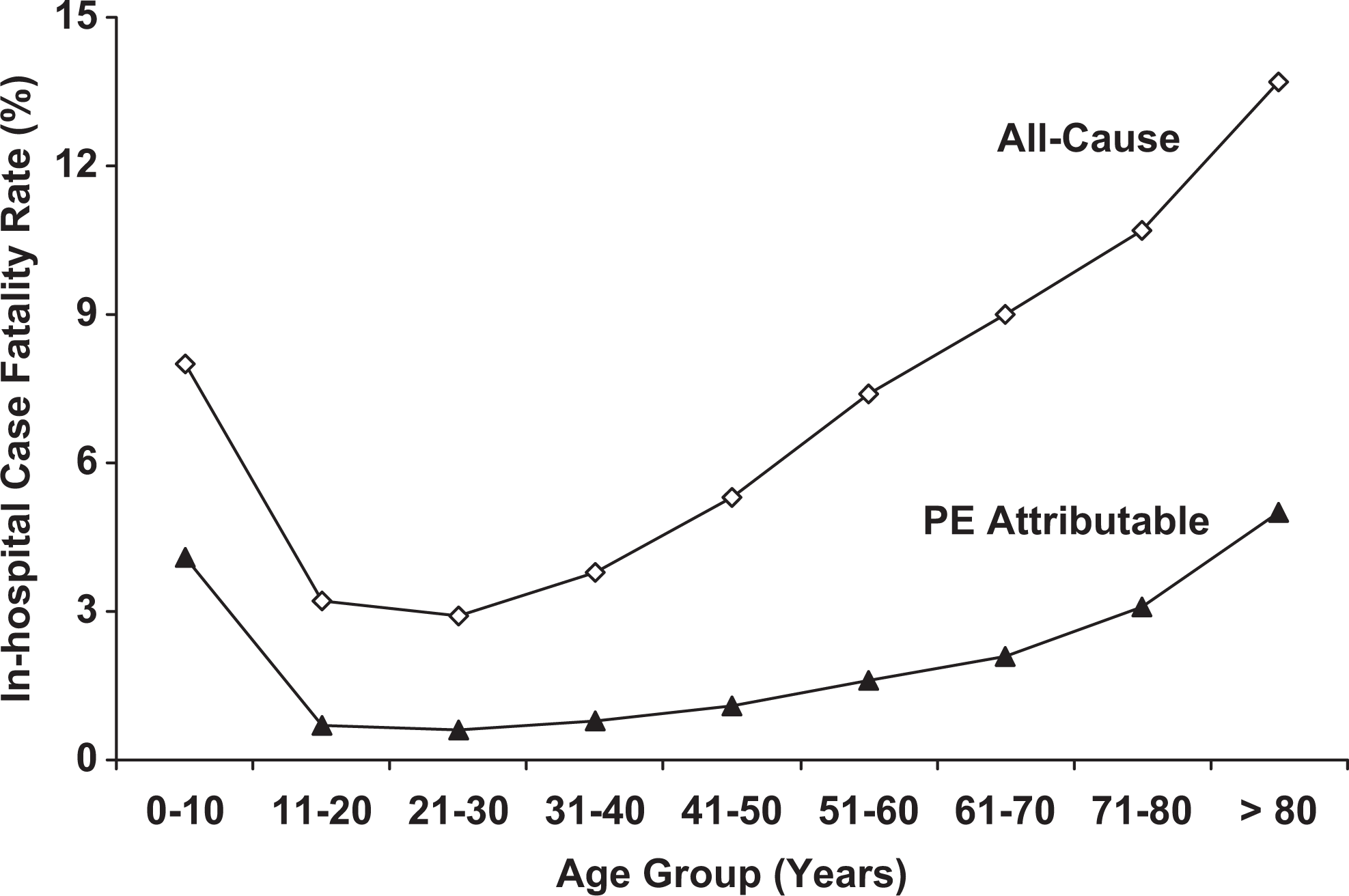
In-hospital case fatality rates according to age. Among patients aged >20 years, all-cause case fatality rate increased linearly with age (r = .9906, P < .0001) as did the case fatality rate attributable to pulmonary embolism (r = .9306, P = .002). The all-cause case fatality rate showed a greater effect of advancing age (slope 1.8 deaths/10 years of age) than death attributable to pulmonary embolism (slope 0.7 deaths/10 years of age; P < .0001).
All-cause case fatality rate showed comparable changes with age in men and women (Figure 2). Case fatality rates showed similar increments with age in blacks and whites (Figure 2). However, the case fatality rates were higher in blacks than in whites in all age groups older than aged 10 years (Figure 2).
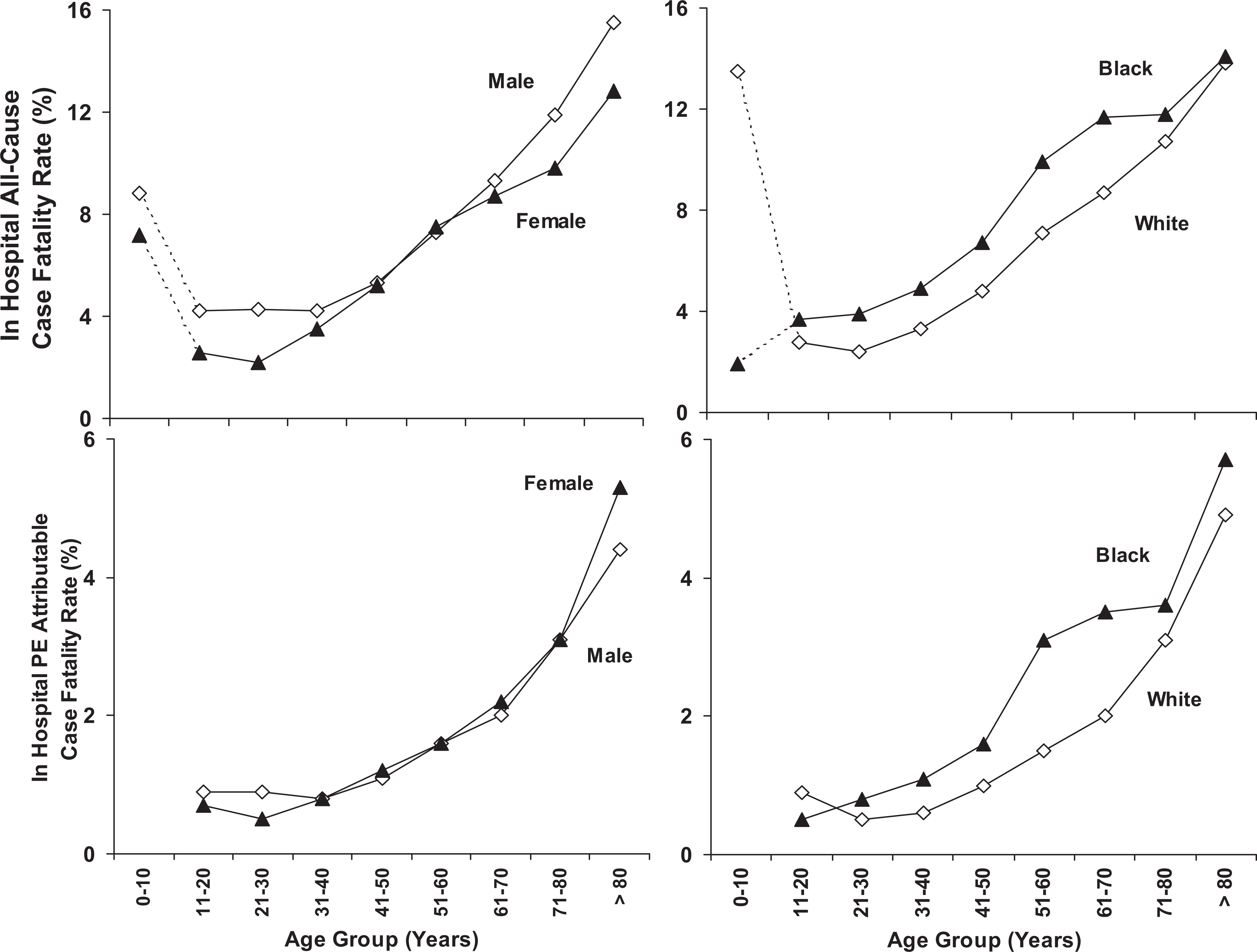
Top. All-cause in-hospital case fatality rate according to age and sex (left) and according to age and race (right). Broken lines indicate that data were sparse in patients aged <11 years. Bottom. In-hospital case fatality rate attributable to pulmonary embolism according to age and sex (left) and according to age and race (right). Data in patients <11 years were insufficient for inclusion.
All-cause case fatality rate in patients aged >20 years was affected more by advancing age in unstable patients than in stable patients (5.3 deaths/10 years of age vs 1.7 deaths/10 years of age; P < .0001; Figure 3). In both stable and unstable patients, age-related case fatality rate increased similarly in men and women and in blacks and whites.
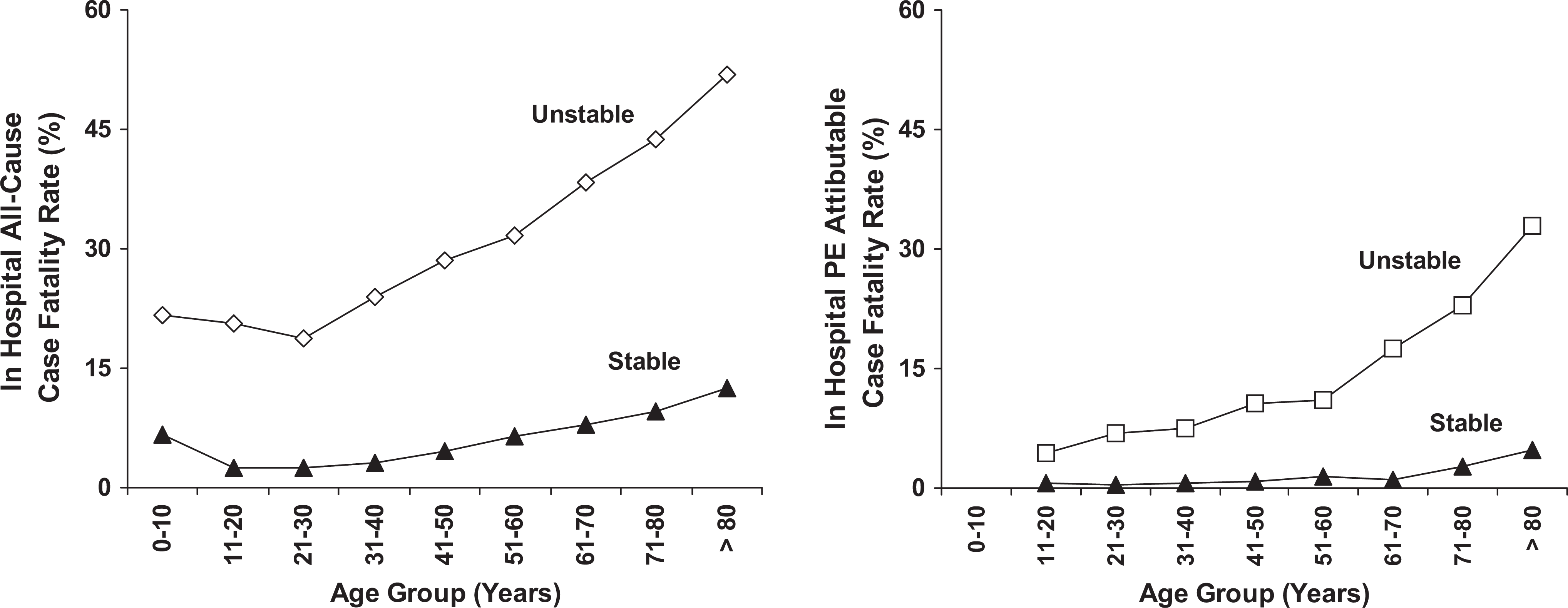
Left. All-cause in-hospital case fatality rate according to age and stability. Among unstable patients aged >20 years, the all-cause case fatality rate increased linearly with age (r = .9928, P < .0001) as did case fatality rate in stable patients (r = .9862, P < .0001). Unstable patients showed a greater effect of advancing age on all-cause case fatality rate (slope 5.3 deaths/10 years of age) than stable patients (slope 1.7 deaths/10 years of age; P < .0001).
Impact of Age on Case Fatality Rates Attributable to Pulmonary Embolism
In-hospital case fatality rate attributable to PE from 1999 to 2008 was 12 600 of 590 000 (2.1%). In adults aged
Advancing age resulted in a smaller effect on death attributable to PE than on all-cause case fatality rate (0.7 deaths/10 years of age vs 1.8 deaths/10 years of age; P < .0001; Figure 1).
Case fatality rate attributable to PE showed comparable increments with age in men and women and in blacks and whites (Figure 2). Case fatality rates attributable to PE, however, were higher in blacks than in whites (Figure 2).
Case fatality rate attributable to PE was affected more by advancing age in unstable patients than in stable patients (4.1 deaths/10 years of age vs 0.6 deaths/10 years of age; P = .0005; Figure 3). In both stable and unstable patients, age-related case fatality rates attributable to PE increased similarly in men and women and in blacks and whites.
Discussion
Children had case fatality rates comparable to elderly individuals. Among adults, case fatality rate was affected more by advancing age in unstable patients than in stable patients. This was shown with all-cause case fatality rate and case fatality rate attributable to PE. All-cause case fatality rate was affected more by advancing age than by case fatality rate attributable to PE. These results may influence the prognostic value of risk assessment tools for patients with PE.
All-cause case fatality rates based on the present data from 1999 to 2008 closely correspond to data from the National Hospital Discharge Survey combined with the US Bureau of the Census Compressed Mortality File from short-stay hospitals throughout the United States from 1979 to 1998.
1
The present data show an all-cause case fatality rate of 2.9% among patients aged 21 to 30 years, and previous data showed a case fatality rate of 3.6% among patients aged 25 to 34 years.
1
The present data show an all-cause case fatality rate of 13.7% among patients aged >80 years, and previous data showed case fatality rate 17.4% among patients aged
Our data showed a biphasic curve descriptive of the effects of age on case fatality rate. The lowest case fatality rates were in patients aged 21 to 30 years, with higher case fatality rates with advancing age and higher case fatality rates in children <11 years of age. Data, however, were sparse in patients aged <11 years. A similar biphasic curve relating age to case fatality rate was shown by Hermann et al in 1961. 6 They too showed a nadir in patients aged 20 to 30 years.
We previously showed higher case fatality rates among blacks than whites
1
based on the data from the National Hospital Discharge Survey combined with the US Bureau of the Census Compressed Mortality File.
1
The present data confirm this and show higher case fatality rates in blacks, irrespective of age. Among patients aged
Strengths of this investigation include the large number of patients. This permitted the assessment of the impact of advancing age on case fatality rates according to whether patients were stable or unstable and whether deaths were due to any cause or attributable to PE. The large number of patients permitted further assessment of the effects of advancing age according to sex and race.
A limitation of the investigation is that data were “sparse” for patients aged <11 years. Additional limitations are an imperfect sensitivity of coding. However, sensitivity for significant procedures, including mechanical ventilation, exceeds 90%. 15 Fisher et al reported a sensitivity of coding for major procedures that ranged from 88% to 95%. 16 Among the comorbid conditions in the Charlson Index 12 on which data are available, sensitivities ranged from 88% to 100%. 15
The discharge code for shock does not require a strict definition. If the physician recorded a discharge code for shock, it is likely that the patient had some manifestation of it. The coding is likely, therefore, to be specific, but it may not be sensitive.
The positive predictive values for the first-listed diagnosis included in the Charlson index, based on ICD-10 codes in the Danish National Registry of Patients, were 98.0% to 100%. 17
Specificity for significant procedures was 100% 15 and specificity for diagnoses was over 94% and generally over 99%. 16 The data ranged from 99.4% to 100% for the specificities of the comorbid conditions included in the Charlson Index. 15
Review and reabstraction of a sample of Medicare hospitalizations from late 1986 to early 1989 showed that 92% of codable cases for PE were on the abstract.
18
A 0.4% prevalence of PE in hospitalized patients
In conclusion, all-cause case fatality rate in adults is affected more by advancing age than case fatality rate attributable to PE. Both all-cause case fatality rate and case fatality rate attributable to PE are affected more by advancing age in unstable patients than in stable patients. Limited data suggest that the case fatality rate of children is comparable to that of the elderly individuals.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.