
Abstract
Three factor VII (FVII) promoter haplotypes are associated with stratified plasma FVII levels. To our knowledge, this is the first study examining the distribution of FVII gene polymorphism and levels in Turkish population. The study population was classified into 3 groups according to the absence of coronary arterial disease and presence or absence of a history of myocardial infarction. It was found that the levels of FVII coagulant activity (FVIIc) were higher in the event group than that of the other groups. Participants with high FVIIc levels were found to have 2-fold increased risk for myocardial infarction. The alleles at the FVII loci in all cases are similar. In conclusion, our results indicate that FVIIc levels have an important predictive role in cardiovascular events. The distribution of FVII gene polymorphisms in the Turkish population shows significant differences when compared with European populations.
Introduction
Factor VII (FVII), a single chain zymogen, is a serine protease that plays a role in initiating thrombosis. The levels of FVII are determined by environmental and genetic factors. 1 –4 In recent years, researchers have investigated the relationship between markers of thrombus formation and acute coronary syndromes; by contributing to a prothrombotic state, elevated levels of FVII may provide a mechanism for acute coronary syndromes. The relationship between plasma FVII levels and risk of coronary artery disease (CAD) has been researched in several studies. Meade et al, in the Northwick Park Heart study, reported a significant association of FVII coagulant activity (FVIIc) with fatal myocardial infarction. 5 In that study, elevation of 1 standard deviation (SD) in plasma FVII was associated with a 62% risk over the first five years. Some studies have suggested these results, 6 –9 but other studies have not confirmed them. 10 –12 The association between FVII levels and risk of CAD is not clear. Differences in FVII level assay methods have been suggested as an explanation for these results. In addition, same factors, such as smoking, age, and gender, affect levels of FVII and risk of CAD. Therefore, the study results may be confusing.
Genetic factors have been shown to affect FVII levels in some studies. Three FVII promoter haplotypes are associated with stratified plasma FVII levels. 4,13 –16 The first haplotype is a decamer insertion at position −323 in the 5′promoter region, where allele A1 corresponds to the absence of the decamer and allele A2 to its insertion. 15,17 The second is in codon 353 in exon 8 of the FVII gene (353R/Q), and the last one is a variable number (5–8) of repeats in the hypervariable region 4 of intron 7 (IVS7). However, the evidence of an association between these polymorphisms and risk of CAD is unclear. Bernardi et al indicated that the IVS7, 353R/Q, and A1/A2 polymorphisms are responsible for up to 5-fold differences in mean FVII levels. 18 In another study, the mean levels were lower in A2A2 and QQ than in A1A1 and RR subtypes. 19 Iacoviello et al found that homozygosity of the Q allele was associated with significant protection from myocardial infarction (MI). 20 In another Italian study, it was reported that higher numbers of repeats were associated with higher messenger RNA (mRNA) expression levels. 3 However, other studies failed to detect a relationship between polymorphisms and the risk of MI. 12,21,22
The present study, therefore, was designed to evaluate and analyze whether FVII levels are affected by intragenic polymorphisms and to assess their association in a normal population and in patients with CAD. To the best of our knowledge, this is the first study to examine the distribution of FVII gene polymorphisms in a Turkish population.
Methods
Patients
Consecutive patients referred to our coronary angiography laboratory between April 2007 and April 2008 were included in this study. The patients were classified into 3 groups according to the absence of CAD and presence or absence of a history of myocardial infarction by combining data from the medical histories after a thorough review of the medical records. Coronary atherosclerosis was defined as plaque or stenosis of at least one major coronary artery. The control group was required to have normal coronary arteries, as documented by angiography and no history of MI. Patients were excluded if they were non-Turkish or had one non-Turkish parent; if they had valvular heart disease, atrial fibrillation, elevated liver enzymes, untreated hypothyroidism, familial hypercholesterolemia, renal failure, or known cancer; or if they used oral anticoagulants or hormone therapy. At the time of blood sampling, a complete clinical history, including the presence or absence of cardiovascular risk factors, was obtained from all the patients. The study was approved by our institutional ethics boards. Either written or oral informed consent was obtained from all the patients.
Laboratory Tests
The measurement of FVII level was conducted at least 1 month after MI. Fasting blood samples were obtained from the antecubital vein, using a 2-syringe technique to reduce tissue factor contamination. Cholesterol and triglycerides were measured with an enzymatic method. Blood samples were collected in 0.109 mol/L trisodium citrate for the assay of FVII levels and centrifuged at room temperature at 2500 g for 30 minutes. The plasma was kept at −80°C until the examination day. At the end of the study, FVIIc levels were assayed by a one staged method, using FVII-deficient plasma and recombiplastin.
Genomic DNA was isolated according to the instructions of the manufacturer, Dr Zeydanli DZ Isolation System. The primers for polymerase chain reaction (PCR) amplification were as follows: 5′F7 polymorphism (5′-TTTGACTCGCATGATTGCTA-3′ and 5′-GGACAGGAGAAAGGTCAGGT-3′);IVS7 polymorphism (5′-GCAATGTGACTTCCACACCTC-3′ and 5′-GGATGTCTGTCTGTCTGTGGA-3′); 353R/Q (5′-GCGCTTCTCATTGGTCAG-3′ and 5′-CACAGAACATGTACTCCGTGA-3′). The annealing temperatures were 58°C, 60°C, and 58°C, respectively.
The genotypes were established by agarose-gel electrophoresis, as follows: (1) 5′F7 polymorphism, alleles A2 (decamer insertion) and A1 (absence of decamer); (2) variable number of tandem repeats in intron 7 (IVS7), alleles H7 (7 monomers), H6 (6 monomers), respectively. Finally, regarding the 353R/Q polymorphism, restriction digestion with TspGWI enzyme was performed for determining alleles G and A.
Statistical Analysis
Clinical and demographic characteristics were compared among the groups of participants. Differences in means were tested by analysis of variance (ANOVA), and differences in proportions by the chi-square test. The chi-square test was also used to assess the genotype frequencies for Hardy–Weinberg equilibrium. Correlations between risk factors were determined by Pearson correlation analysis. The relationship of FVIIc and the haplotypes to coronary events was evaluated with logistic regression analysis adjusted for age, gender, smoking, diabetes, and hypertension.
Results
Characteristics of Patients
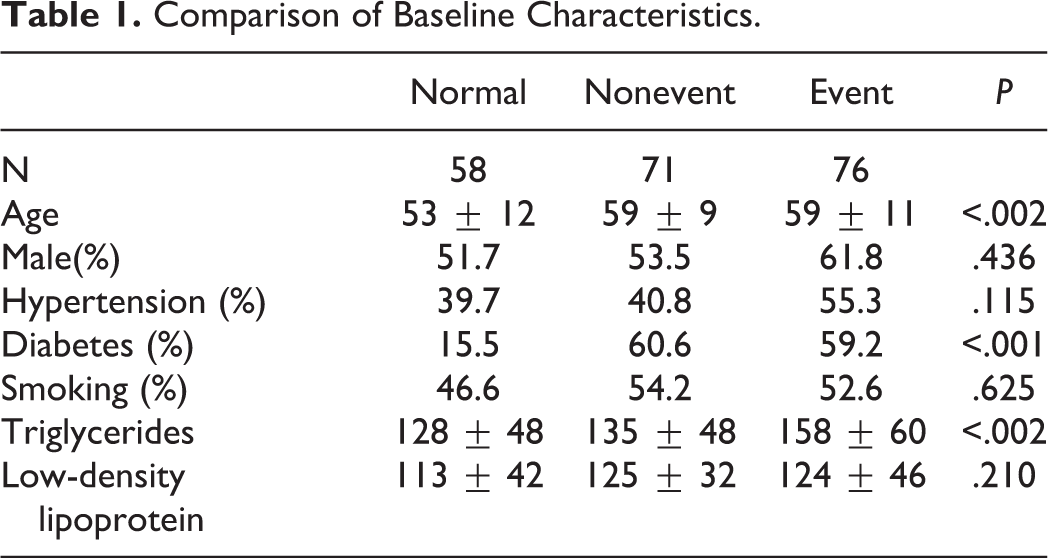
We investigated 58 healthy controls, 71 patients with CAD without previous MI, and 76 survivors of MI. Table 1 shows the cardiovascular risk factors for the patients and the controls. The prevalence of diabetes mellitus was significantly higher in the patients than in the controls. Median values for age and triglyceride levels were significantly higher in the patient groups than in with the control group.
Comparison of Baseline Characteristics.
Factor VIIc Levels
The levels of FVIIc were higher in the event group than in the nonevent and healthy groups (Table 2). Correlation of event history, FVIIc levels, and other risk factors were as follows. Event history was significantly related with age, presence of diabetes, triglyceride levels, and FVIIc (Table 3). In ROC curve analysis, the value for FVIIc levels to detect acute coronary syndrome with a sensitivity of 59.2% and specificity of 60.5% was 98.5. The area under the curve was 0.632 (Figure 1). Participants with high FVIIc levels (>98.5) were found to have a 2-fold increased risk of MI, after correction for possible confounders—age, sex, diabetes, and triglycerides levels—(95% CI, 1.087-3.685; Table 4).
The Levels of FVIIc in Groups.
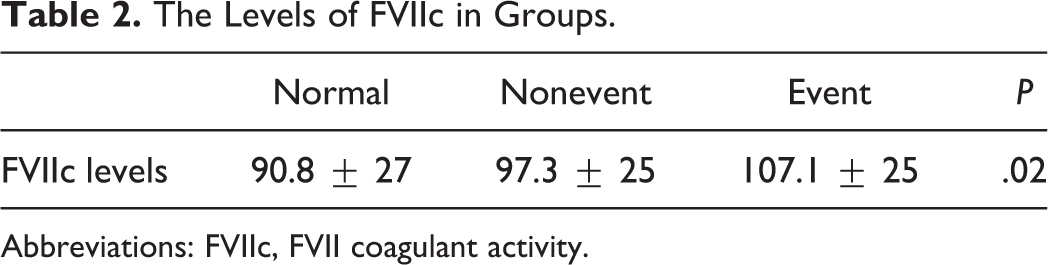
Abbreviations: FVIIc, FVII coagulant activity.
Correlation Between History of Acute Coronary Syndrome and Risk Factors.
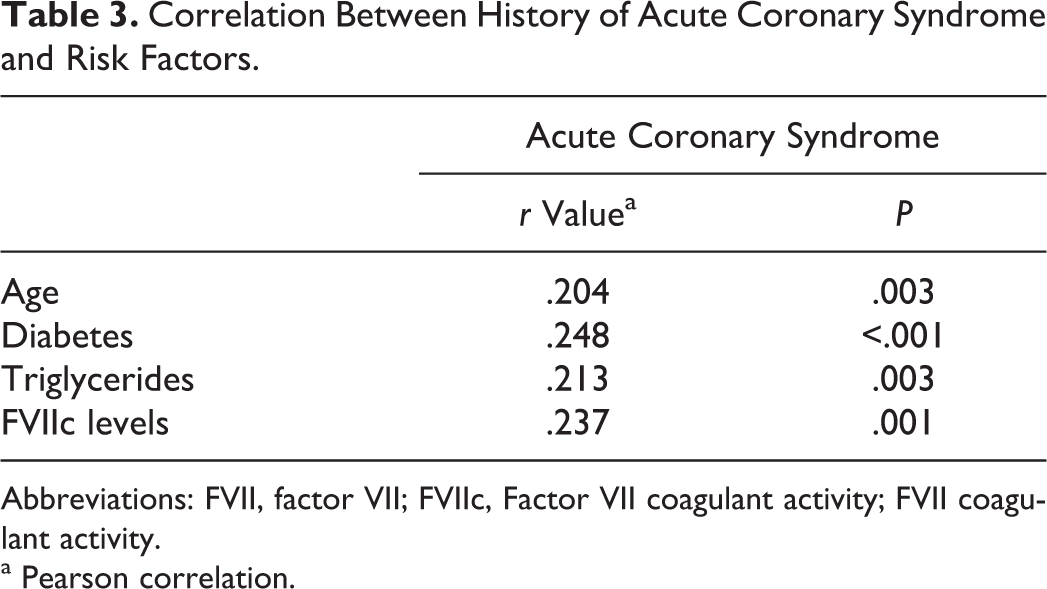
Abbreviations: FVII, factor VII; FVIIc, Factor VII coagulant activity; FVII coagulant activity.
a Pearson correlation.
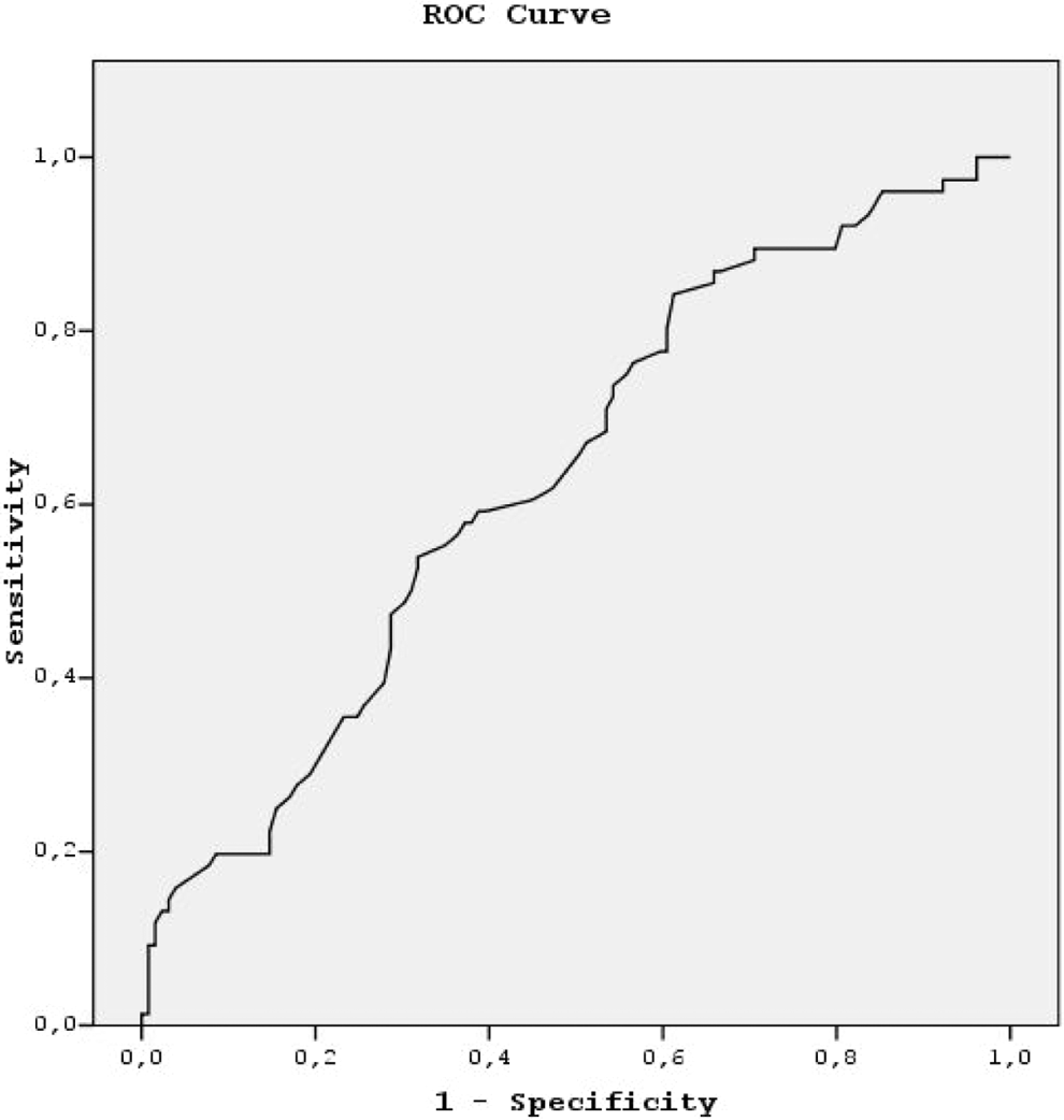
Receiver–operating characteristic (ROC) curve for FVII coagulant activity (FVIIc) levels.
Risk of Myocardial Infarction for FVIIc Levels and Other Factors.
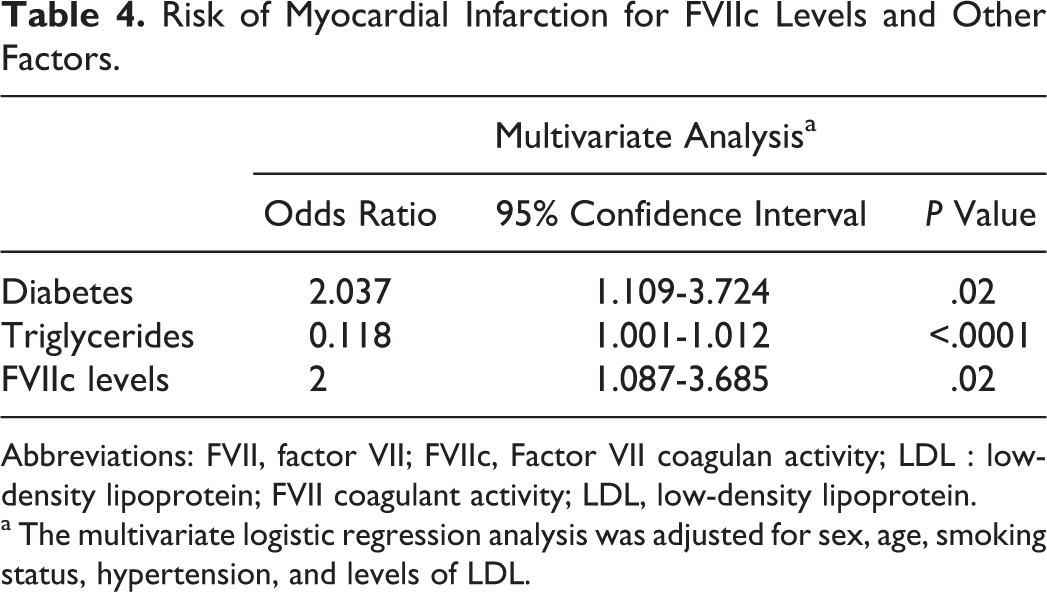
Abbreviations: FVII, factor VII; FVIIc, Factor VII coagulan activity; LDL : low-density lipoprotein; FVII coagulant activity; LDL, low-density lipoprotein.
a The multivariate logistic regression analysis was adjusted for sex, age, smoking status, hypertension, and levels of LDL.
Prevalence of FVII Polymorphisms
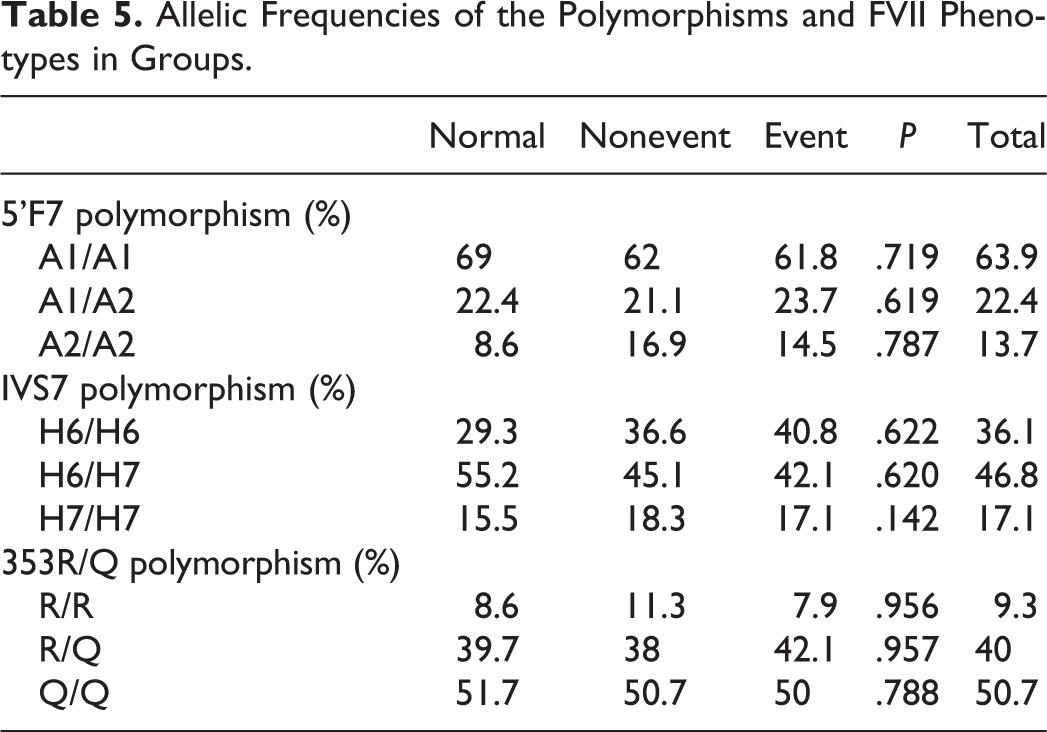
The genotypes and alleles at the FVII loci in all cases were similar (Table 5). There was no association between genotype and history of MI, but there was a significant association between the FVII Q allele and lower FVII levels (Table 6). No association was found for the 5′F7 and IVS7 polymorphisms.
Allelic Frequencies of the Polymorphisms and FVII Phenotypes in Groups.
Factor VIIc Levels in All Groups According to Polymorphisms.
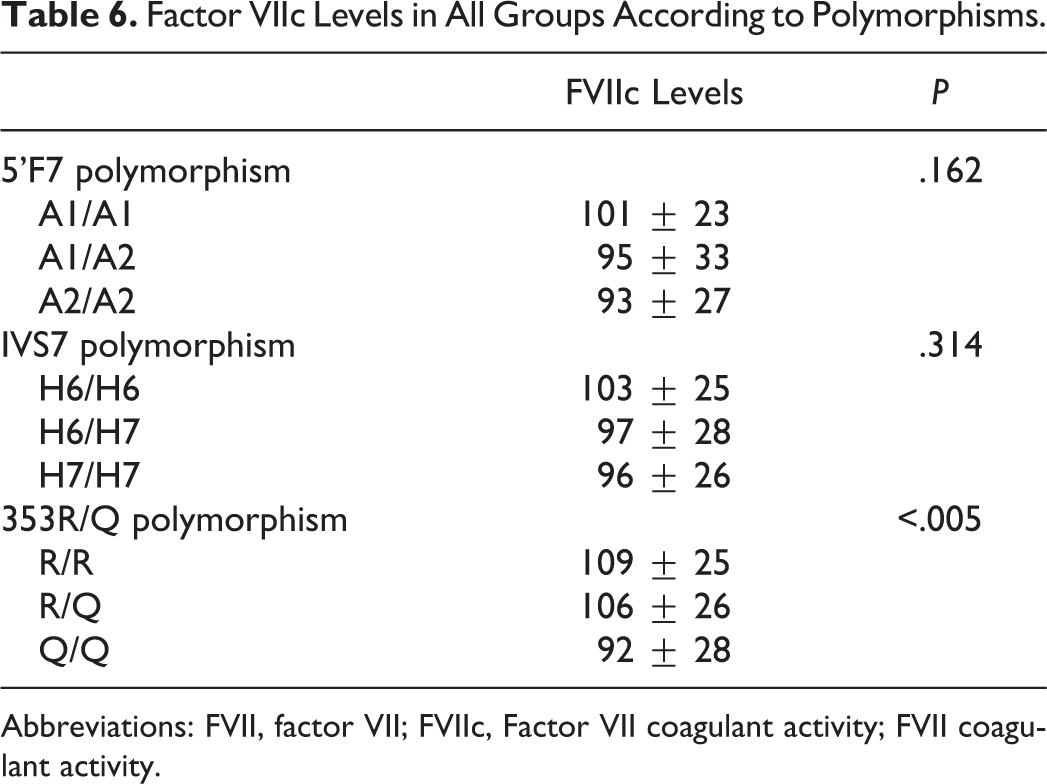
Abbreviations: FVII, factor VII; FVIIc, Factor VII coagulant activity; FVII coagulant activity.
Discussion
The main finding in this study was that FVIIc levels were strong predictors of MI, independent of other cardiovascular risk factors. The 353R/Q polymorphism in the FVII gene was significantly associated with lower FVIIc levels, but no association was found for the 5′F7 and IVS7 polymorphisms. To our knowledge, this is the first study to examine the distribution of FVII gene polymorphisms in a Turkish population.
Our main finding was a strong and independent association between high FVIIc levels and MI. The levels of FVIIc were significantly elevated in the patients, compared with the controls (Table 2). Participants with FVIIc levels >98.5 had a 2-fold increased risk of MI. These associations remained significant after adjustment for possible confounders (Table 4). Meade et al found that high levels of factor VII coagulant activity and plasma fibrinogen were associated with increased risk, especially for events occurring within 5 years of recruitment. These associations seemed to be stronger than cholesterol. 5 Consistent with that study, we found FVIIc levels to be more powerful than triglyceride and LDL levels for predicting risk of MI. Campo et al. found similar results in their study. 23 However, we did not find a relationship between FVIIc level and presence of CAD. Similar findings were observed in another study. 24 Domanic and his colleagues found that FVII level is not an independent risk factor for the progression or severity of CAD. 25 As understood from these results, FVIIc levels may be associated with only thrombotic complications of atherosclerosis.
The results of our genetic association analyses suggest that haplotype Q/Q is associated with decreased FVIIc levels, but no association was found for the 5′F7 and IVS7 polymorphisms. There are similar results in the literature on this subject. Girelli et al found that the Q/Q, H7/H7, and the A2/A2 genotypes were associated with significantly lower FVIIc levels. 19 In another Italian study, similar results were found. 20 Unlike many studies, our results indicate that a genetic propensity for low FVII levels is not associated with the risk of MI. The patient and control groups were similar in terms of the distribution of genotypes (Table 3). The genotypes were not related to each other in terms of the risk of MI. Doggen et al found that a genetic propensity for high FVII levels is not related to the risk of MI in men. 12 Similar results were obtained in an Italian study. 26 The ECTIM study was to assess the impact of genetic polymorphisms on risk of MI and the extent to which conventional and genetic risk factors explain the differences in MI risk between the four centers 27 This study found that the FVII 353R/Q genotype strongly determines FVIIc, although neither factor has a strong impact on MI risk. On the contrary, many studies have reported that certain FVII genotypes have a role in protection against MI. 19,20,23
There are probably several reasons that may explain the different results. The first is that the 353R/Q polymorphism is a functionally different FVII molecule. It is possible that the charge changed, thus having an indirect effect on plasma levels and cleavage of the inactive single-chain zymogen to FVII. 12 The failure to detect interactions between genotype and risk of MI is probably compounded by the lack of statistical power, due in part to the high frequency of the QQ genotypes and survivors of MI in our study. The prevalence of the Q allele was found to be 70.5%, compared to 14.2% in European populations. 28 The relatively small number of patients in our study may explain this situation. In addition, distributions of different genes may vary in different geographical regions. On the other hand, the frequency of MI is higher in Turkey than in Italy. 29 Therefore, the Q allele may not be a protection against MI. This result was also observed in other studies. 12,26,30 . However, genetic protection may be suppressed because of differences in sociocultural and environmental factors.
There were some limitations to this small clinical study that looked at FVII levels, FVII gene polymorphisms, and their association with MI. Because the sample size was small, future randomized trials are needed. In addition, control group selection was a problem, as angiographies were conducted on all the participants, so there was not really a “normal” population. Finally, we did not measure the markers of the coagulation system.
In conclusion, our results indicate that FVIIc levels have an important predictive role in cardiovascular events. Even the 353R/Q polymorphism in the FVII gene is significantly associated with lower FVIIc levels; however, a preventive effect against MI was not observed with any genotypes. The distribution of FVII gene polymorphisms in the Turkish population shows significant differences when compared with European populations.
Footnotes
Acknowledgment
This research was supported by the Gazi University Scientific Research Projects Unit.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.