
Abstract
Platelet microparticles (PMPs) and function profile in children with congenital heart disease (CHD) have not been widely explored. We investigated platelet aggregation, flow cytometric platelet surface receptors (P-selectin and glycoprotein (GP) IIb/IIIa) and PMPs in 23 children with cyanotic CHD (CCHD), 30 children with acyanotic CHD (ACHD) and 30 healthy controls correlating these variables to hematological and coagulation parameters including von Willebrand factor antigen (vWF Ag) as a marker of endothelial dysfunction. Hemoglobin, hematocrit (HCT),
Introduction
Congenital heart disease (CHD) is the most common type of birth defect and responsible for more deaths in the first year of life than any other birth defects. 1 It has been recognized for decades that patients with cyanotic CHD (CCHD) show significant bleeding tendency and are prone to both thrombosis and hemorrhage, 2 however, patients with acyanotic CHD (ACHD) may also have a mild bleeding disorder. 3 The precise mechanisms of the increased incidence of thromboembolism in patients with CCHD have not yet been determined but endothelial dysfunction, hemostatic abnormalities, and platelet activation may be the underlying factors. 4 –6 On the other hand, the hemorrhagic diathesis is attributed to thrombocytopenia, shortened platelet life-time, suppressed platelet aggregation, and increased vascularity associated with nitric oxide or prostacyclin released from the vascular endothelium, probably triggered by high shear stress due to hyperviscosity. 7
P-selectin is an adhesion molecule found in the secretory α-granules of platelets and Weibel-Palade bodies of endothelial cells, and is mobilized to the plasma membrane on activation. 8 –10 Microparticles (MPs) derived from vascular endothelium or circulating blood cells circulate in the peripheral blood and vary in size from 0.2 to 2.0 μm. They originate from blebbing and shedding from cell membrane surfaces in physiological and pathological conditions. Increased levels are generated by a number of mechanisms including platelet activation. 11
A population of platelet-derived MPs (PMPs) is generated during platelet activation, whereas other PMPs populations are derived from megakaryocytes during megakaryopoiesis or quiescent circulating platelets, or might result from platelet apoptosis. 12,13 Platelet MPs are the most abundant and were originally studied because of their procoagulant activity. 14 The expression of P-selectin on the surface of PMPs provides additional prothrombotic potential. 11
Circulating levels of MPs are augmented in most cardiovascular diseases
15
and increased production of PMPs has been reported in various conditions or modalities, such as patients with disseminated intravascular coagulation,
16
myocardial infarction,
17
unstable angina,
18
diabetes mellitus,
19
sickle cell disease, and β-thalassemia.
20
–22
Platelet MPs level combined with
Because the clinical relevance of PMPs in patients with CCHD has not been widely explored particularly in pediatric age group and platelet activation in those patients is still a subject for debate, this study aimed to investigate PMPs, adenosine diphosphate (ADP)-induced platelet aggregation, and activation using expression of P-selectin (CD62P) and the activated conformation of glycoprotein (GP) IIb/IIIa (PAC-1 binding) in children with CHD correlating these variables to hematological and coagulation parameters including von Willebrand factor antigen (vWF Ag) as a marker of endothelial dysfunction.
Participants and Methods
Participants
This study included 53 Egyptian patients with CHD, randomly selected from those attending the Cardiology Clinic, Pediatric Hospital, Ain Shams University. Thirty age- and sex-matched healthy individuals were enrolled as a control group. An informed consent was obtained from the patients and control participants or their legal guardians before enrollment in the study. The study was approved by the local ethical committee of Ain Shams University. Exclusion criteria were radical operation for a heart defect due to hypoplastic pulmonary arteries or high pulmonary vascular resistance for the Fontan circulation or due to Eisenmenger syndrome, and the intake of antiplatelet drugs within 2 weeks before blood sampling.
The studied patients included 23 patients with CCHD; 13 males and 10 females with a male-to-female ratio of 1.3:1. Their ages ranged from 1.5 to 8.1 years, with a median of 3.5 years. Thirty children with ACHD; 18 males and 12 females (ratio, 1.5:1) were enrolled. Their ages ranged from 1 to 8 years, with a median of 5 years. In CCHD group, 14 patients had tetralogy of Fallot and 9 patients had double outlet right ventricle with pulmonary stenosis while in the acyanotic group, 14 patients had ventricular septal defect (VSD) including 8 with muscular VSD and 6 with perimembranous VSD, and 16 patients had secundum atrial septal defect. The clinical and laboratory characteristics of the studied patients are listed in Table 1. The control group included 17 males and 13 females (ratio, 1.3:1) with a median age of 5.3 (range, 2-9.5 years).
Clinical and Hematological Data in Patients With Congenital Heart Diseases.a
Abbreviations: CCHD, cyanotic congenital heart disease; ACHD, acyanotic congenital heart disease; IQR, interquartile range; MCV, mean corpuscular volume; MPV, mean platelet volume; PMPs, platelet microparticles; ADP, adenosine diphosphate; Aggmax, maximal platelet aggregation; Agglate, late platelet aggregation; GP, glycoprotein; FEU, fibrinogen equivalent units; vWF Ag, von Willebrand factor antigen.
a Data were expressed as mean ± SD and comparisons were done using Student t test, number (%) where chi-square test was used, or median (IQR) where Mann-Whitney test was used for statistical analysis.
All the studied patients were subjected to (i) detailed medical history including disease duration and drug intake; (ii) full clinical assessment with special emphasis on cardiac examination and monitoring of oxygen saturation by pulse oximetry; (iii) laboratory investigations including complete blood count (CBC) using Sysmex XT-1800i (Sysmex, Japan) and examination of Leishman-stained smears, quantitative
Methods
Sampling
Peripheral blood samples were collected in vacutainer tubes containing potassium EDTA in a final concentration of 1.5 mg/mL for CBC and in vacutainer tubes containing 0.2 mL 3.8% trisodium citrate in a ratio of 9 volumes of blood to 1 volume of citrate for platelet and coagulation studies. Samples collected in both tubes were properly mixed with the used anticoagulant.
ADP-induced platelet aggregation using light transmittance aggregometry
Platelet-rich plasma (PRP) was obtained as a supernatant by centrifugation of citrated whole blood for 10 minutes at 1000 rpm. A second centrifugation was done at 3000 rpm for 10 minutes to obtain platelet-poor plasma (PPP). Platelet count was performed on PRP using Sysmex XT-1800i and counts were adjusted between 200 and 400 × 109/L by dilution with autologous PPP. Platelet aggregation was assayed by the turbidimetric method in a 2-channel aggregometer (Chrono-Log 450 Model; Chrono-Log, Havertown, Pennsylvania), according to other reports. 25,26 Light transmission was adjusted to 0% with PRP (equivalent to 100% absorbance) and to 100% for PPP for each measurement. Platelet aggregation was assessed within 2 hours from blood sampling. Aggregation was assessed in siliconized tubes at 37°C in constant stirring conditions, and was induced by 5 μmol/L ADP (Diamed, Switzerland) as described elsewhere. 27,28 The ADP-induced platelet aggregation was measured at peak (Aggmax), where aggregation was expressed as the maximal percentage change in light transmittance from baseline with PPP from the same patient as a reference, and late aggregation at 5 minutes (Agglate). The Aggmax is considered to reflect the activity of both P2Y1 and P2Y12 receptors, whereas Agglate is indicative of P2Y12 receptor activity. 29
Flow cytometric analysis of platelet receptor expression and PMPs
Evaluation of surface expression of platelet receptors by standard 3-color flow cytometry was performed in citrated whole blood based on other studies 30 –32 with the use of fluorescein isothiocyanate (FITC)-conjugated PAC-1 antibody (Becton Dickinson, Rutherford, New Jersey) which binds directly to the activated GP IIb/IIIa receptor, FITC-labeled anti-CD62P which recognizes expression of the platelet surface antigen, P-selectin reflecting platelet α-granule secretion (Beckman Coulter, Inc., Fullerton, CA), phycoerythrin (PE)-labeled anti-CD41b (Becton Dickinson), and FITC and PE isotypic controls (Beckman Coulter). Briefly, 10 μL of citrated blood were diluted with 490 μL phosphate-buffered saline (PBS); Sigma Chemicals, St Louis, Missouri. A volume of 35 μL of the mixture was added to 5 μL of anti-CD62P FITC or 5 μL of PAC-1 antibody FITC, 5 μL of anti-CD41b PE, and 5 μL of ADP (5 μmol/L) or PBS (for resting samples). A resting sample was performed to ensure the absence of in vitro platelet activation and determine the spontaneous level of CD62P expression. Samples were protected from light and incubated at room temperature for 20 minutes until data acquisition in EPICS-XL PROFILE II Coulter flow cytometer (Beckman Coulter, Inc., Fullerton, CA). Gating was done on CD41b-positive events, which reflect GP IIb/IIIa, and platelet activation was expressed as the percentage of platelets positive for antibody binding. Platelet-derived MPs were differentiated from normal-sized platelets by forward scatter size analysis. Ten thousand positive platelet events were analyzed and PMPs were reported as a percentage of the total platelet events. 7,30,31
Statistical analysis
Analysis of data was done using Statistical Program for Social Science version 15 (SPSS Inc, Chicago, Illinois). Quantitative variables were described in the form of mean, standard deviation (SD), median and range, and qualitative variables were described as number and percentage. Student t, Mann-Whitney, and chi-square tests were used for intergroup comparisons. Correlations between the hematocrit (HCT) value and PMPs, P-selectin, ADP-induced aggregation, and platelet count were analyzed by Spearman rank correlation coefficient. A P values <.05 was considered significant in all analyses.
Results
None of the enrolled patients had pulmonary hypertension as shown by echocardiograghy. Their estimated pulmonary pressure ranged from 12 to 23 mm Hg with a mean of 16 ± 3.1 mm Hg. Comparison between clinical and hematological data of cyanotic and acyanotic patient groups (Table 1) revealed significantly higher oxygen saturation, hemoglobin level, HCT, mean corpuscular volume,
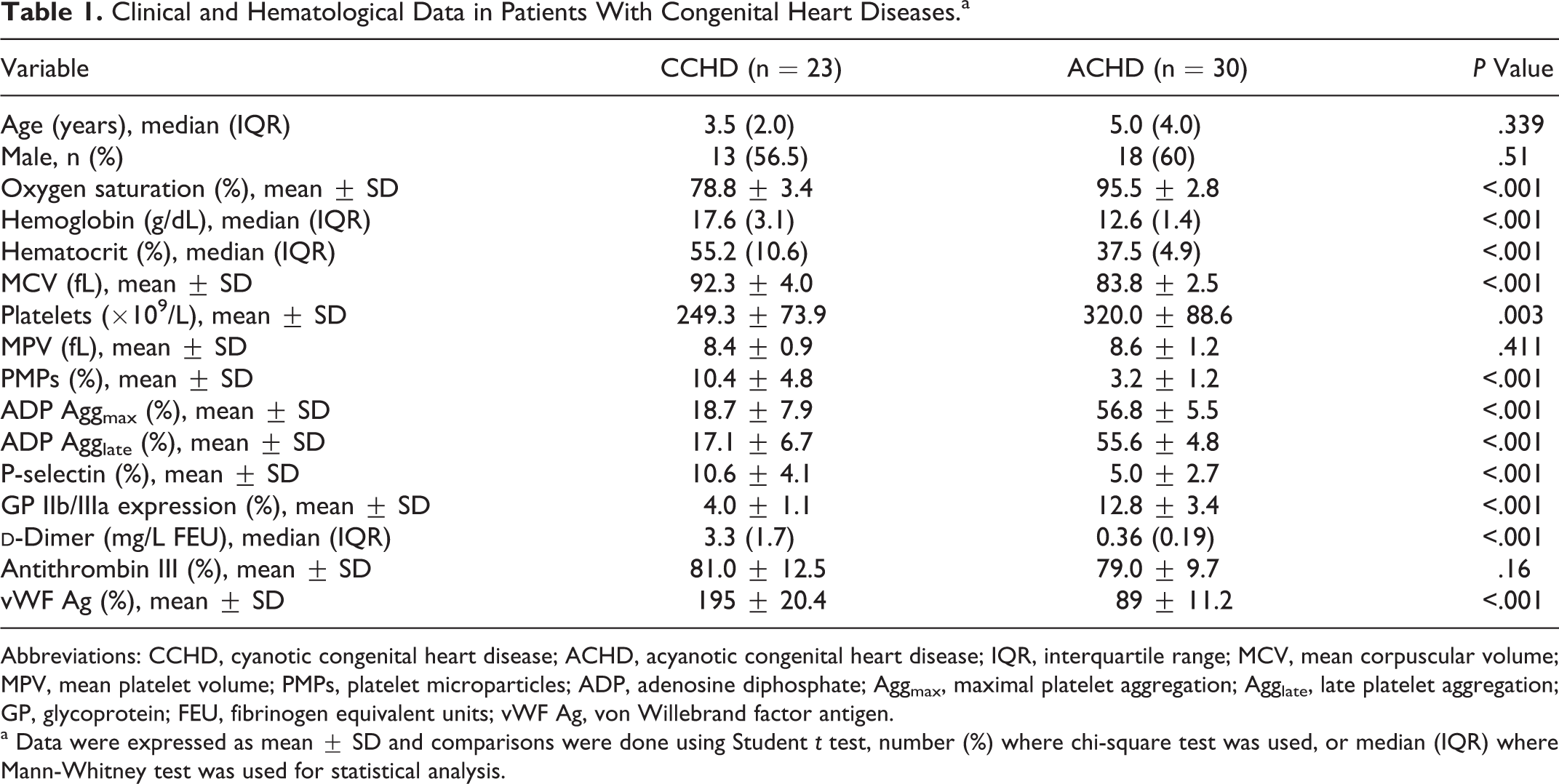
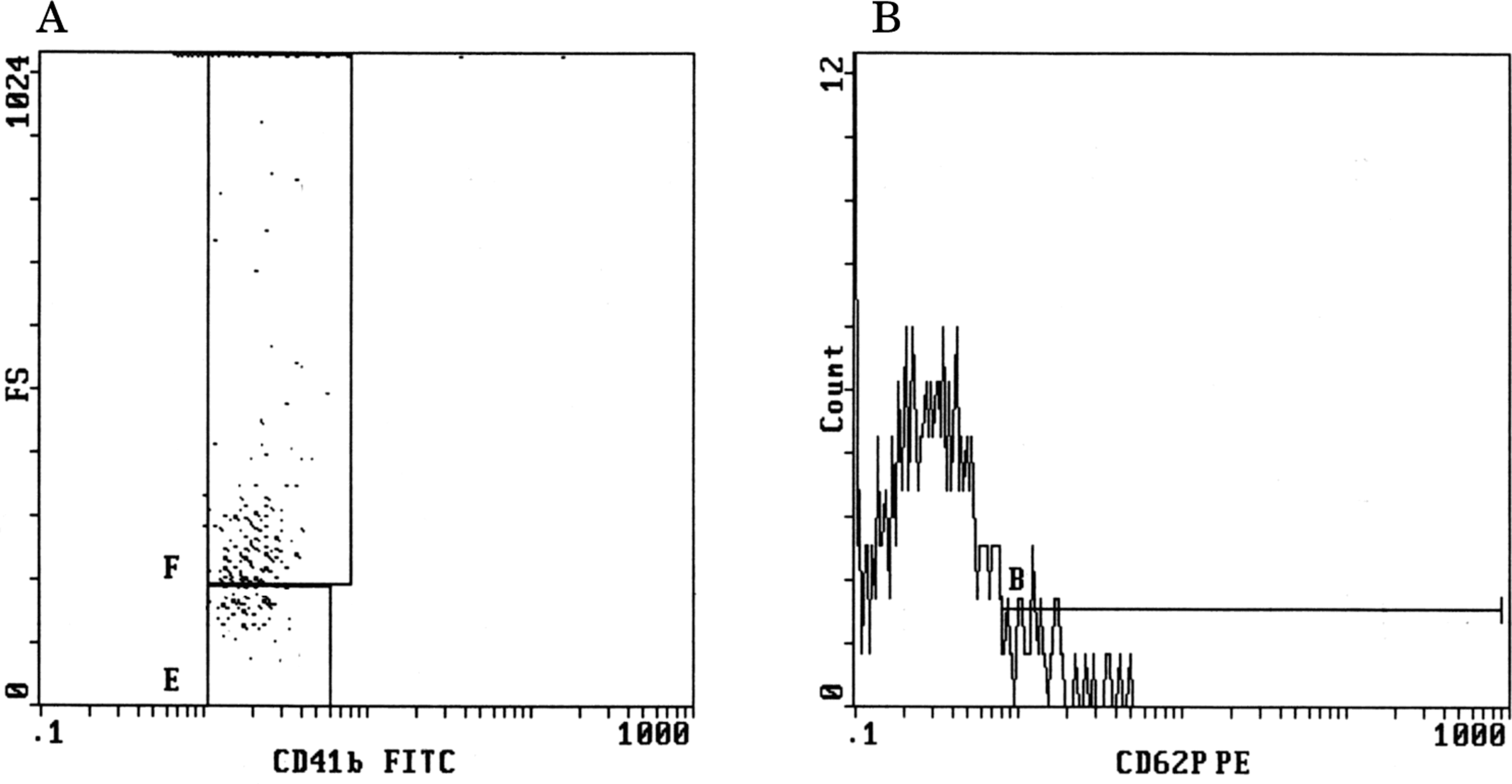
Assessment of PMPs and P-selectin expression showed significant increase in both CCHD and ACHD groups compared with healthy children (mean PMPs in control participants was 1.3 ± 0.6 and mean P-selectin expression was 2.5 ± 1.2; P < .001). However, the elevation of PMPs and P-selectin was more evident in patients with CCHD than ACHD group (PMPs, 10.4 ± 4.8 vs 3.2 ± 1.2 and P-selectin, 10.6 ± 4.1 vs 5.0 ± 2.7, respectively, P < .001; Table 1). Representative examples of flow cytometric detection of PMPs (CD41b+ particles) and P-selectin (anti-CD62P) are shown in Figures 1 and 2. The expression of GP IIb/IIIa (PAC-1 binding) and percentage of platelet aggregation (Aggmax or Agglate) with respect to 5 μmol/L ADP were significantly lower in CCHD than ACHD group (P < .001; Table 1) but levels were similar between acyanotic patients and healthy controls (P > .05). No significant difference was found between the percentage of Aggmax and Agglate within CCHD or ACHD groups (P > .05).
Flow cytometric detection of increased platelet microparticles (A) and P-selectin (B) in a patient with cyanotic congenital heart disease.
Flow cytometric detection of decreased platelet microparticles (A) and P-selectin (B) in a patient with acyanotic congenital heart disease.
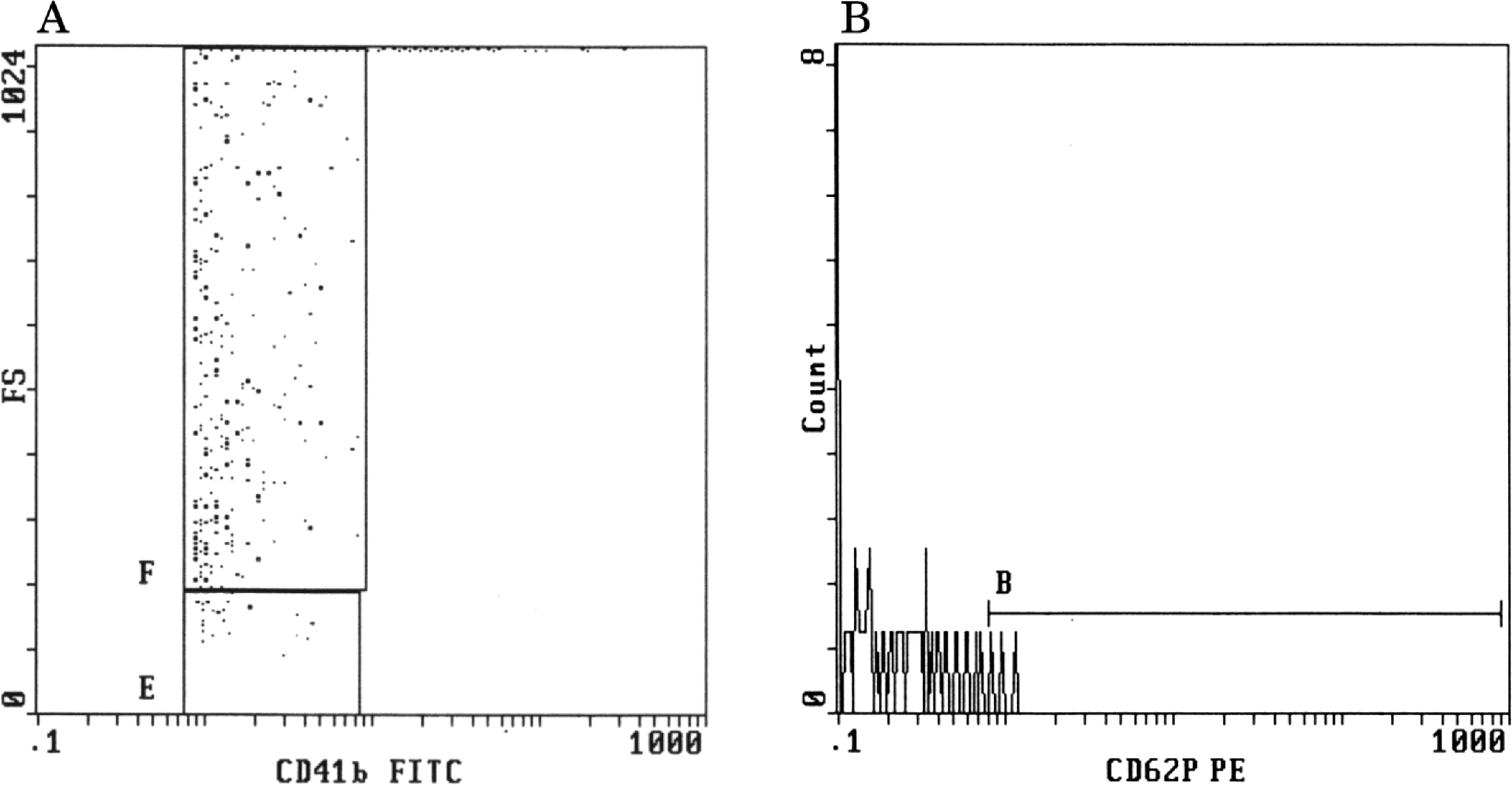
Notably, significant negative correlations were found between both platelet count and aggregation and HCT in patients with CCHD or ACHD (P < .001; Figure 3). A significant positive correlation was observed between platelet aggregation and GP IIb/IIIa (PAC-1 binding) in CCHD (r = .851, P < .05) or ACHD group (r = .812, P < .05). Both PMPs and P-selectin expression were positively correlated to HCT (P < .001; Figure 4),
Negative relationships between hematocrit value and laboratory data; (A) platelet count and (B) platelet aggregation. Solid circles: cyanotic congenital heart disease group; open circles: acyanotic congenital heart disease group.
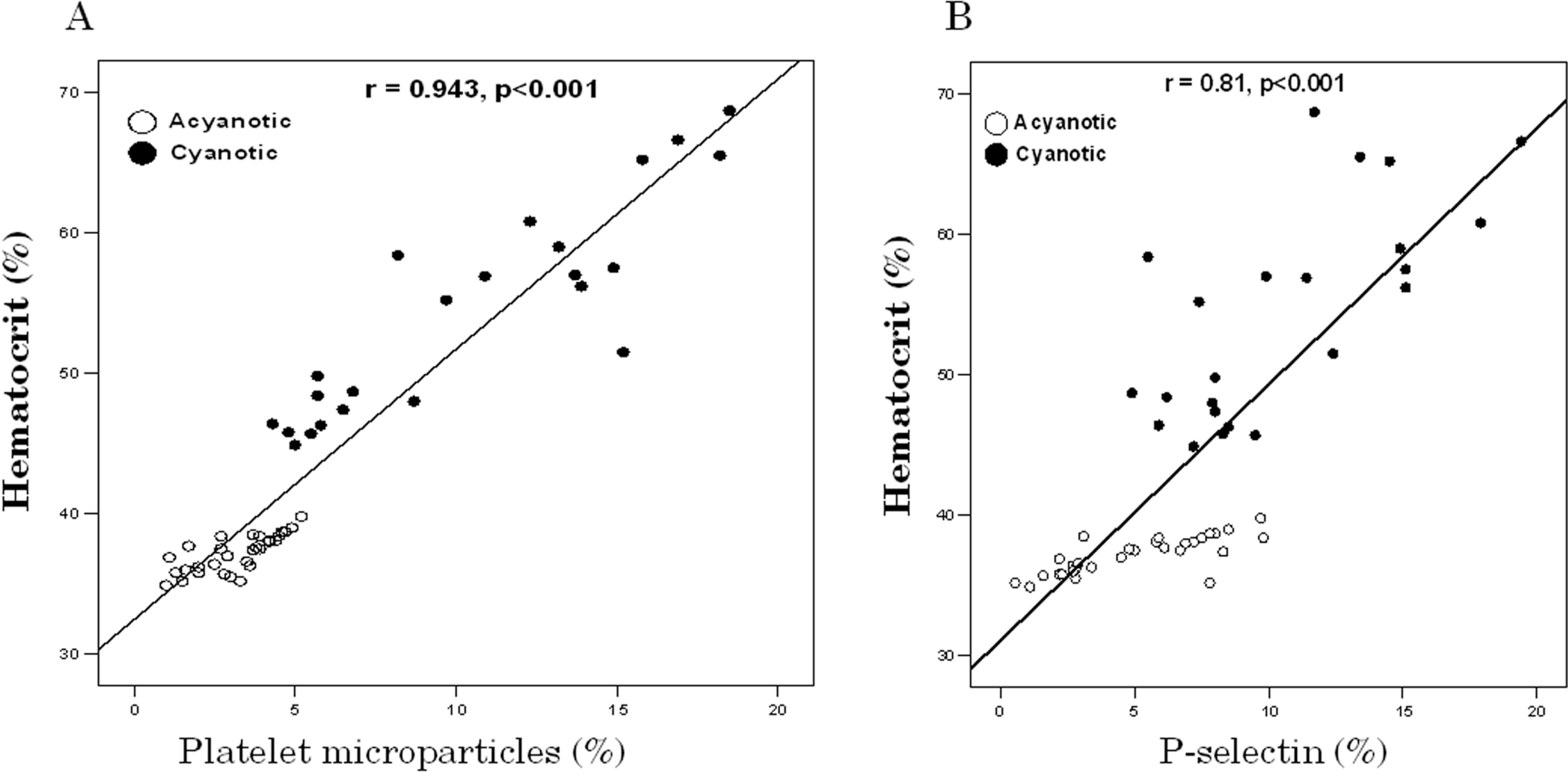
Positive relationships between hematocrit value and laboratory data; (A) platelet microparticles and (B) P-selectin. Solid circles: cyanotic congenital heart disease group; open circles: acyanotic congenital heart disease group.
Discussion
Congenital heart conditions are different in adults than in children. Platelet dysfunction, thrombocytopenia, disseminated intravascular coagulation, and decreases in coagulation factors are prevalent in pediatric patients with either CCHD or ACHD. 33,34 These qualitative and quantitative abnormalities are more prominent in the cyanotic population and greatly exaggerated in infants. 34,35 Considerable interest for cell-derived MPs has emerged, pointing out their essential role in hemostatic response and their potential as disease markers. 36 Given that the field of pediatric coagulation/hemostatic disorders continues to evolve, understanding the pathogenesis of these abnormalities in such patients would be necessary to determine their impact on clinical outcomes and response to therapy.
In this study, platelet count and the percentage of ADP-induced platelet aggregation were decreased in patients with CCHD compared with ACHD group and inversely correlated to HCT. Several lines of evidence indicate shortened life span and suppressed aggregability of platelets in patients with CCHD. 4,7 Platelet count correlates negatively with the HCT value in these studies. 4,7,37
Four pathogenetic mechanisms are encountered in CCHD (1) decreased megakaryocyte production, (2) decreased platelet production, (3) increased platelet destruction, and (4) increased platelet activation. It has been hypothesized that the pathogenesis of thrombocytopenia in CCHD reflected the right-to-left shunts that deliver whole megakaryocytes into the system arterial circulation, bypassing the lungs where megakaryocytic cytoplasm is fragmented into platelets, thus reducing platelet production. 38 However, mean platelet counts in our studied patients with CCHD were within normal range, although decreased than those with ACHD, and MPV values were comparable between the CCHD and ACHD groups suggesting that the cause of suppressed platelet aggregation in those patients does not originate from the process of platelet production (fragmentation of megakaryocytes). This is in agreement with Horigome et al. 7
We found a nonsignificant difference between the percentage of Aggmax and Agglate within CCHD and ACHD groups denoting that P2Y12 receptor was able to induce full and irreversible platelet aggregation. P2Y12, 1 of the 2 platelet receptors for ADP, plays a central role in platelet function and defects of P2Y12 should be suspected when ADP, even at high concentrations is unable to induce full, irreversible platelet aggregation. 39 Signaling events downstream of the P2Y12 receptor mediate thromboxane A2 production, α-granule release and subsequent expression of P-selectin on activated platelets. 40
In our study, higher PMPs and P-selectin expression levels were found in children with CCHD and ACHD compared with healthy controls, although this elevation was more prominent in CCHD with polycythemia than ACHD group and significant correlations were observed between these 2 variables and HCT in both patients’ groups. A similar increase in PMPs has been reported in adult patients with coronary artery disease. Although it is a different disease, yet, the presence of vascular stenosis generated turbulent flow and high shear stress of the platelet surface, resulting in overproduction of MPs. 24
Only Horigome et al 7 evaluated the role of PMPs in those patients and in line with our findings; PMPs were overproduced in patients who have CCHD with polycythemia, probably due to a high shear stress derived from blood hyperviscosity. However, they found that surface P-selectin levels in patients with CCHD were comparable with those in ACHD group and not correlated with HCT value.
Platelet activation in CCHD has been previously addressed with controversial results. Some studies reported increased platelet activation in CCHD. 3,6,34,41 Olgun et al 3 reported that platelets positive for surface P-selectin were increased in patients with CHD, even in patients with no evidence of clinical thrombosis. Plasma levels of P-selectin were also elevated in CCHD. 42 Kajimoto et al 6 demonstrated that P-selectin expression on the platelets is elevated, although many patients were receiving antiplatelet or anticoagulant drugs, indicating that platelet activation does exist in CCHD. However, they could not find a significant correlation between the HCT and platelet P-selectin. 6
The platelet activation observed in patients with CCHD may be due to increased shear stress resulting from hyperviscosity and/or endothelial dysfunction but the precise mechanisms remain unclear. 43 Our findings in children with CCHD further supported these data and the significant relation between P-selectin expression and HCT levels suggests that increased shear stress due to hyperviscosity may be a major factor causing platelet activation. Additionally, we found increased vWF Ag in patients with CCHD compared with ACHD group and levels were positively correlated with PMPs and P-selectin suggesting a relationship between endothelial damage/dysfunction and platelet activation. von Willebrand Ag is a widely used marker of endothelial dysfunction in vascular disease. 44 Endothelial dysfunction has been shown in the systemic circulation of adults with CCHD because of the chronic hypoxic environment and secondary erythrocytosis resulting in increased shear stress and modification of the balance between vasodilators and vasoconstrictors. 45
In contrast to our results, some studies failed to demonstrate elevated platelets P-selectin in patients with CCHD. 7,46 The reason for that is not clear but the difference may be partly attributed to the method used for blood sampling as it has been reported that the blood extraction maneuver itself might have activated platelets in patients with polycythemia. 7 Therefore, in addition to gentle withdrawal of blood samples, we performed flow cytometric analysis of a resting blood sample to ensure the absence of in vitro platelet activation.
Horigome et al 7 also speculated that it is not easy to recognize platelet activation by the flow cytometric technique for α-granule secretion (anti-P-selectin), because the process is ongoing in this specialized condition of slowly progressing or stable polycythemia. It has been reported that circulating degranulated platelets rapidly lose surface P-selectin to the plasma pool but continue to circulate. 47 These findings lead to the assumption that platelets that continue to circulate after degranulation, a kind of “incompetent platelets” after activation, might account for suppressed platelet aggregation in CCHD. Circulation of incompetent platelets after activation by high shear stress might be interpreted as a physiologic adjustment, so that formation of massive thrombi is precluded. 7
However, because degranulated platelets that have lost surface P-selectin to the plasma pool would have a smaller MPV in CCHD compared with ACHD group while in our study; MPV was consistent among the 2 groups and additionally, we found decreased expression of GP IIb/IIIa (PAC-1 binding) in patients with CCHD compared with ACHD, therefore, we could assume that suppressed aggregation in our patients with CCHD may be due to a defect in platelet GP IIb/IIIa receptor, the fibrinogen receptor that represents the final common pathway of platelet aggregation, and not circulating incompetent platelets. Moreover, the circulation of P-selectin negative platelets was only observed in murine models or baboons and it was unclear whether or not this phenomenon occurs in humans or what the timescale of shedding can be. 48
Some studies have also showed abnormalities of aggregation and decreased expression of GP IIb/IIIa while P-selectin expression remained unchanged or increased. 49 –51 It has been found that P-selectin stabilized initial platelet aggregates formed by GP IIb/IIIa–fibrinogen interactions, allowing the formation of large platelet aggregates. This defines the role of P-selectin in platelet aggregation. 52 Furthermore, “platelet activation” is a collective term used to describe quite different phenomena that may be regulated differently and not even occur simultaneously or in concert. For example, binding of the monoclonal antibody PAC-1 and the antibody against P-selectin of the platelet surface represents 2 totally different phenomena: a conformational change in the GPIIb-IIIa complex versus secretion from the intracellular located α-granules. Thus, results of assays of platelet activation may differ somewhat between clinical disorders involving different activation processes. 53,54
Increased PMPs and platelet activation with suppressed aggregation may have clinical implications. It has been shown that the combination of increased platelet activation with decreased function was associated with increased mortality in patients with severe injury and trauma. 51 Therefore, patients with CCHD with similar findings should be thoroughly followed-up and further studies are needed to assess the relation between PMPs overproduction and platelet activation with decreased function on the clinical outcome of those patients.
In addition, we found that
Nevertheless, Horigome et al
7
found that
Study Limitations
One limitation of the present investigation deserves consideration is the relatively small number of patients within subgroups with CHD. Although PMPs and platelet function profile differed strikingly between the 2 groups, making a false-positive finding extremely unlikely, yet, further analysis including larger number of children would help to verify our findings. It is worth to note that although we showed directly that platelet activation exists in CCHD, assessment of platelet factor 4 and β-thromboglobulin would provide additional information in those patients.
In conclusion, this study provides further insights on the role of platelets in the pathogenesis of abnormal coagulation in children with CHD. The overproduction of PMPs and platelet activation with suppressed aggregation may be implicated in the pathogenesis of prominent coagulation/hemostatic abnormalities observed in children with CHD, particularly those with CCHD and are linked to high HCT levels suggesting that increased shear stress due to hyperviscosity may be a major factor causing platelet activation. Endothelial dysfunction is evident in children with CCHD and related to increased PMPs and platelet activation. Although the prognostic potential of circulating PMPs is still in its infancy, their detection and quantification is a potentially valuable tool in CHD to identify patients at increased risk. However, prospective studies are needed to assess the potential impact of platelet activation markers on the clinical outcome of those patients and response to therapy. Further investigations are also needed to fully explore the relation between platelet function profile and endothelial dysfunction, using other markers as soluble adhesion molecules.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.