
Abstract
Background:
Vitamin D deficiency is associated with cardiovascular disease such as coronary artery disease, heart failure, and hypertension. Vitamin D deficiency activates the renin–angiotensin–aldosterone system, which affects the cardiovascular system. For this reason, it could be suggested that there is a relationship between vitamin D deficiency and atrial fibrillation (AF). In our study, we compared 25-hydroxyvitamin D (25-OHD) levels between nonvalvular AF, valvular AF, and control groups in sinus rhythm.
Method:
A total of 102 patients with nonvalvular chronic AF without any other cardiovascular disease (mean age 62.51 ± 5.88; group I) and 96 patients with AF, which is associated with mitral valve disease (mean age 61.51 ± 5; group II) were included in our study. Of all, 100 age-matched healthy people with sinus rhythm were accepted as control groups (mean age 61.35 ± 5.44). Routine biochemical parameters, 25-OHD and parathormone levels were performed.
Results:
Baseline characteristics of the study groups were comparable. Group I patients had a lower vitamin D level than group II and the control group (6.51 ± 4.89, 9.24 ± 7.39, and 11.18 ± 6.98 ng/mL, P < .001, respectively). In groups I and II, the patients’ left atrium diameter and systolic pulmonary artery pressure are higher than the control group.
Conclusion:
As a result, our study revealed a relationship between vitamin D deficiency and nonvalvular AF.
Introduction
Atrial fibrillation (AF) is the most common cardiac rhythm disorder. The estimated prevalence of AF ranges from 0.4% to 1% in the general population and increases by age. Atrial fibrillation is an important public health issue, which increases the risk of mortality, stroke, and cardiac failure. 1 –3
In AF, atrial fibrosis, reduced atrial muscle mass, and atrial dilatation are often encountered. It is thought that the renin–angiotensin–aldosterone system (RAAS) accounts for the majority of these physiopathologic changes. It is also known that calcium plays an important role to initiate AF and in electrophysiologic remodeling. Intracellular calcium overload within the atrial myocytes plays a role in the development and maintenance of AF through shortening the action potential time and atrial refractory period. 4 Angiotensin 2 plays an important role in the development and maintenance of AF by increasing the spontaneous release of calcium from sarcoplasmic reticulum and triggering fibroblast proliferation.
Recently, it was found that the angiotensin II level increases in new-onset AF. 5 It is known that vitamin D affects the cardiac functions via both direct and indirect pathways.
Furthermore, vitamin D ensures blood pressure regulation and prevents cardiac hypertrophy via inhibition of renin activity. 6
Given this information, we thought that vitamin D deficiency could be related to AF.
In our study, we planned to research the association of vitamin D deficiency among the patients with valvular and nonvalvular AF who appealed to our outpatient clinic and its association with AF.
Materials and Methods
Selection of the Patients
Among 198 successive patients aged 50 to 70 years, who appealed to the Cardiology outpatient clinic at Bursa Education and Research Hospital in the period from November 2010 to March 2011, were diagnosed with persistent AF; the study included 102 patients with nonvalvular chronic AF without any other cardiovascular disease (42 male; average age 62.51 ± 5.88; group I) and 96 patients with AF, which is associated with rheumatic mitral valve disease who have moderate or severe mitral stenosis and/or regurgitation (38 male; mean age 61.51 ± 5; group II) were included in our study. Of all, 100 age-matched healthy people with sinus rhythm were accepted as control groups (40 male; mean age 61.35 ± 5.44). According to the study protocol that was approved by the ethics committee of Bursa Education and Research Hospital, the patients were asked to sign the informed written consent. Since the level of 25-hydroxyvitamin D (25-OHD) differs due to seasonal changes (effect of the sunlight), the study was started in the winter season and continued up to the end of March.
Patients with chronic renal failure, chronic liver disease, cardiac failure (ejection fraction [EF] below 50%), coronary artery disease, obstructive sleep apnea and chronic obstructive pulmonary disease, stroke, diabetes mellitus, hypertension, bone disorders, troide disorder, previous gastrectomy, or having intestinal malabsorption and taking medication may have an effect on vitamin D or parathyroid hormone level such as calcium, vitamin D, or antidepressant drugs were excluded from the study. The study did not include male and female patients younger than 50 years or older than 70 years.
A careful record was made of the underlying disorders of the patients that might lead to AF and vitamin D deficiency, accompanying diseases and the medicines used. The blood pressure of the patients was measured. The patients having a systolic blood pressure ≥140 mm Hg and/or a diastolic blood pressure ≥90 mm Hg and those taking antihypertensive drugs were accepted to be hypertensive. The patients using oral antidiabetic drugs or insulin or those having 2 measurements of fasting blood glucose level ≥126 mg/dL were accepted to be diabetic.
Laboratory Tests
Serum parathormone (PTH) measurements were done using an electrochemiluminescence method on an E 170 Modular Analytic System (Roche, Indianapolis, IN, USA) device. The 25-OHD levels were measured using a BioSource 25-OH-Vit.D3-Ria-CT Kit (Biosource Europe S.A. Rue de L’Industrie, 8, B-1400 Nivelles, Belgium). Reference ranges of 25-OHD3 were accepted as 10 to 50 ng/mL for winter season and 20 to 120 ng/mL for summer season. 7
Transthoracic Echocardiography Protocol
Echocardiographic evaluation was done on a Vivid 7 Pro TTE with 3.5 MHz transducer. All echocardiographic examinations were performed according to the criteria of the American Society of Echocardiography and European Association of Echocardiography guidelines. 8 All echocardiographic images were recorded while the patient was lying in the lateral decubitus position. On echocardiographic evaluation, dimensions of the left ventricle (LF) chamber, wall thickness, LVEF (with Teichholz method), diameter of the left atrium (LA), abnormal blood flows due to valve insufficiency and if present, the degree of valvular stenosis were evaluated with 2-dimensional, M-mode, Doppler, and tissue Doppler studies.
Parasternal long axis, apical 2-, 4-, and 5-chamber views were taken.
Thicknesses of the LV septal and posterior-free walls and LV end-diastolic and endsystolic diameters were measured in parasternal long-axis view with M-mode.
The aortic diameter and anteroposterior diameter of the LA were measured on M-mode views at the level crossing over the aortic valve and the LA in parasternal long-axis view, if LA diameter below 40 mm was considered normal in this view.
On apical 4-chamber view, mid-cavity diameter of the right atrium (RA) was measured when the RA cavity was the largest, if below 42 mm was considered normal in this view.
Systolic pulmonary artery pressure was calculated by adding the estimated RA pressure to the right ventricle systolic pressure obtained from the tricuspid insufficiency peak velocity.
Statistical Analysis
Statistical analyses were done using SPSS (Statistical Package for the Social Sciences ver. 13, SPSS Inc, Chicago, Illinois) software and Epi info pack program. Numeric variables were presented as median ± standard deviation, categorical variables were presented as percentage values. The equality of the data to the normal distribution was assessed with the Shapiro-Wilk test. Since the data was not normally distributed, the Mann-Whitney U test, a nonparametric statistical test was used to compare the average values between the groups. Categorical variables were compared using the chi-square test or Fisher exact chi-square test. To determine the independent risk factors for the AF, a forward stepwise logistic regression model was established. For all statistical studies, a P value <.05 was set to be significant. Our study was consistent with Hardy-Weinberg equilibrium.
Results
Evaluating basic characteristics, there was no statistically significant difference between the 3 groups in terms of medications, age, gender distribution, and body mass index ([BMI] Table 1).
Comparison of Clinical and Biochemical Features of Patients With AF and Controls.
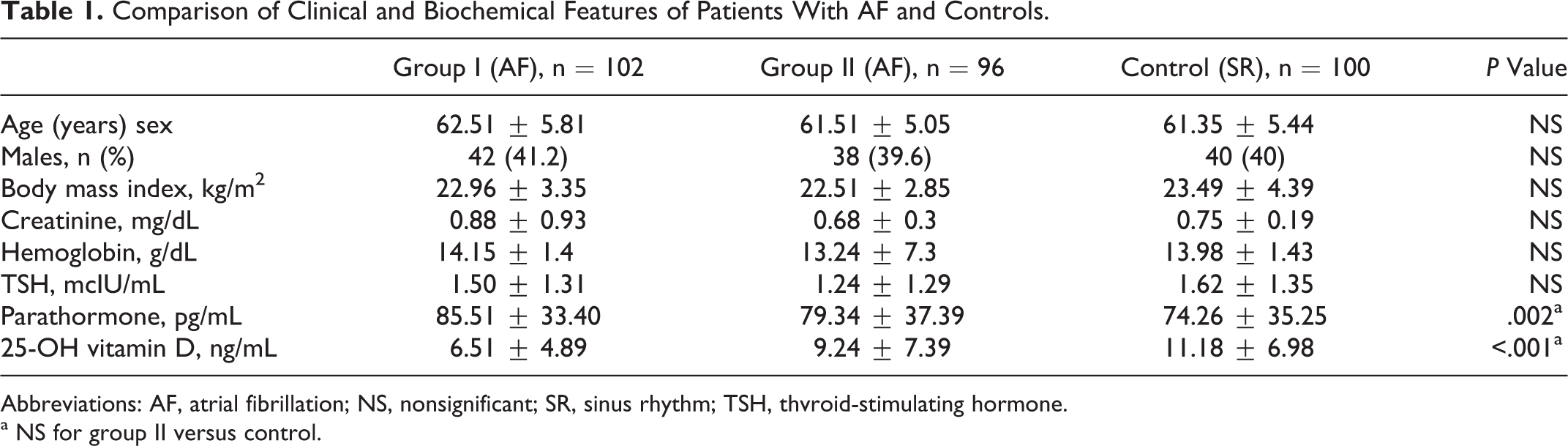
Abbreviations: AF, atrial fibrillation; NS, nonsignificant; SR, sinus rhythm; TSH, thvroid-stimulating hormone.
a NS for group II versus control.
Given the main biochemical parameters, group I patients had a lower vitamin D level than group II and the control group (6.51 ± 4.89, 9.24 ± 7.39, and 11.18 ± 6.98 ng/mL, P < .001, respectively) and group I patients had a higher PTH level than group II and the control group (85.51 ± 33.40, 79.34 ± 37.39, and 74.26 ± 35.25 pg/mL, P = .002, respectively; Table 1).
When the initial conventional echocardiographic parameters of the patients were evaluated, the average LA diameter of the group of the patients with AF (groups I and II) was significantly larger than that of the control group individuals (P < .001). The average systolic PAP of the group of the patients with AF (groups I and II) was significantly higher than that of the control group individuals (P < .001; Table 2).
Comparison of Conventional Echocardiographic Features of Patients With AF and Controls.
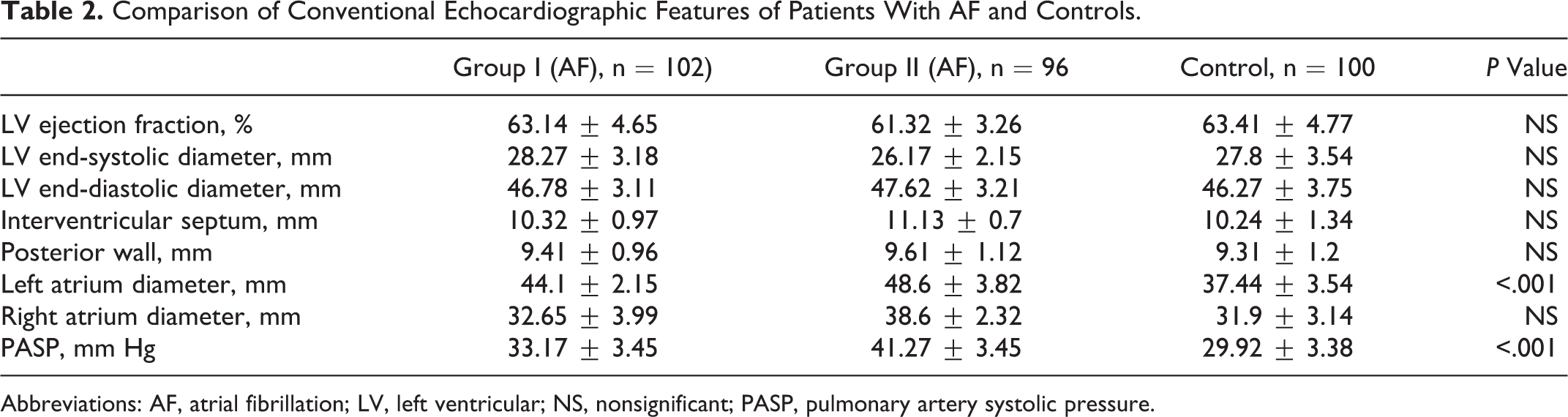
Abbreviations: AF, atrial fibrillation; LV, left ventricular; NS, nonsignificant; PASP, pulmonary artery systolic pressure.
There was no statistically significant difference between the groups in terms of the average end-diastolic and end-systolic LV diameter, LVEF, thicknesses of interventricular septum, and posterior wall (Table 2).
To determine the independent indicators of AF, a forward stepwise logistic regression model was established. In this model, AF was entered as the dependent variable while gender, age, BMI, the diameter of the LA, the diameter of the RA, LVEF, PTH level, and 25-OHD were entered as independent variables. The adjusted R 2 value of the model was 0.714 and P value was <.001.
As a result of the forward stepwise logistic regression analysis, it was found that LA diameter and 25-OHD level were the independent predictors of AF in group I (Table 3). In patients with valvular AF (group II), LA diameter, RA diameter, and systolic PAP were the independent predictors of AF (Table 4).
Logistic Regression Analysis for the Independent Risk Factors for AF (Group I).
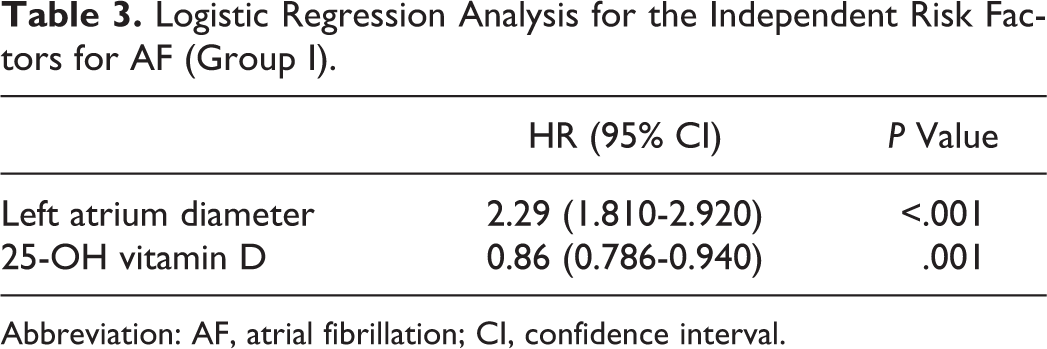
Abbreviation: AF, atrial fibrillation; CI, confidence interval.
Logistic Regression Analysis for the Independent Risk Factors for AF (Group II).
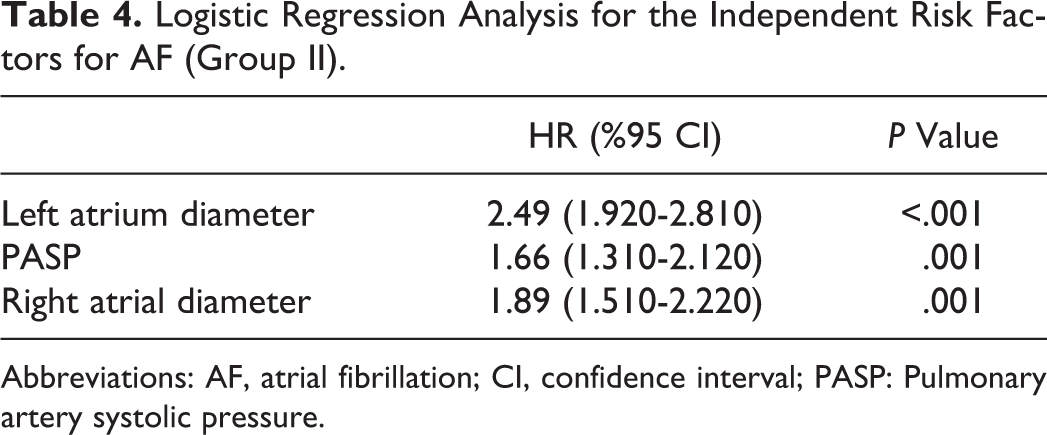
Abbreviations: AF, atrial fibrillation; CI, confidence interval; PASP: Pulmonary artery systolic pressure.
Discussion
Atrial fibrillation is a commonly encountered arrhythmia, which reduces the quality of life of the patients and negatively affects the prognoses of the present diseases. Therefore, impeding the development of AF and protective treatments become more popular today.
Epidemiologic studies have demonstrated that cardiac failure, valvular heart diseases, hypertension, and ischemic heart disease are the most common causes of AF. 2
Recent studies have revealed the functions of vitamin D other than those in bone metabolism. It was reported that it is involved in autoimmune disorders, such as inflammatory bowel disease, rheumatoid arthritis, multiple sclerosis, psoriasis, diabetes, certain types of cancer, hypertension, heart failure, atherosclerosis, peripheral artery disease, and in several infectious diseases. 9
Vitamin D has direct and indirect cardioprotective effects. Vitamin D directly leads to vitamin D receptor (VDR) and CYP27B1 expressions in the vascular smooth muscle cells and in endothelial cells, it enhances the proliferation of vascular smooth muscle cells and expression of vascular endothelial growth factor within these cells and inhibits the proliferation of cardiomyocytes. 6
Indirect cardioprotective effects of vitamin D are explained by certain mechanisms. Vitamin D ensures blood pressure regulation and prevents cardiac hypertrophy by inhibiting the activation of renin, hinders the formation of vascular calcification by reducing the production of matrix metalloproteinases 2 (MMP2) and MMP9, provides glycemic control, leads to pro inflammatory cytokine suppression and an increase in interleukin (IL)-10 levels, and has cardioprotective effects through hindering secondary hyperparathyroidism. 6
Several mechanisms have been proposed for AF development. One of these mechanisms is the atrial wall tension. The atrial wall tension activates RAAS and the levels of angiotensin II and transforming growth factor β1 (TGFB1) increase due to the wall tension. Angiotensin II causes fibrosis formation in the tissue through leading to fibroblast proliferation, therefore, it is thought to be responsible for the pathoanatomic changes found in AF.
Moreover, RAAS has a remarkable role in structural atrial remodeling, as it increases oxidative stress and inflammation; and it predisposes to AF development. 10 –12 The RAAS is associated with hypertensive cardiac disorder, heart failure, myocardial infarct, and myocardial fibrosis seen in cardiomyopathy. The incidence of AF increases in primary hyperaldosteronism. 13 Angiotensin II, which is produced locally in primary hyperaldosteronism, is associated with apoptosis of the myocytes and the fibrosis within the reactive tissues. 14
It has been demonstrated that angiotensin-converting enzyme inhibitors and angiotensin II receptor blocker, which are RAAS blockers, are protective from AF with this mechanism. These drugs reduce new-onset AF by a rate of 18%. That rate is as high as 43% among the patients with cardiac failure. 15 The RAAS blockage diminishes the failure rates after cardioversion and the probability of AF recurrence. 16
The short effective refractory period and slower atrial impulse velocity seen in AF eases the reentry cycles. The decrease in L-type calcium channels in both the short- and long-term causes a shortened plateau time of action potential, duration of action potential, refractory period, and wavelength that is the distance traveled by the electrical impulse during the refractory period. These changes are characteristic for AF. Recently, it has been recognized that there are functions of vitamin D other than those in the bone metabolism. It has been demonstrated in the studies conducted that vitamin D deficiency may play a role in the development of autoimmune diseases, inflammatory bowel disease, rheumatoid arthritis, psoriasis, multiple sclerosis, diabetes, certain types of cancer, cardiac failure, stroke, and infectious diseases, such as tuberculosis and pneumonia, and that vitamin D treatment is efficacious in these patients. 17 –31
Vitamin D ensures blood pressure regulation by inhibiting RAAS and PTH. 32,33 The studies showed that the levels of renin and angiotensin II could be diminished with vitamin D and its analogues. 34 Calcium plays an important role in initiating AF and in electrophysiological remodeling. Intracellular calcium overload within the atrial myocytes plays a role in the development and maintenance of the AF through shortening action potential time and atrial refractory period. 4
Considering the importance of RAAS in the pathophysiology of AF and the negative regulatory role of vitamin D for renin, we thought that vitamin D deficiency could be related to AF.
When 3 groups were compared in our study, 25-OHD levels of the patients having nonvalvular AF were significantly lower than 25-OHD levels of the patients without AF and valvular AF (P < .001). Our present data show that vitamin D deficiency may be related to nonvalvular AF in the Turkish population. The atrial biopsy specimens of patients with lone AF revealed inflammatory cell infiltration and fibrosis signs. Oxidative stress and inflammation play an important role in atrial remodeling. The relationship between the inflammation and AF was researched using C-reactive protein (CRP) levels. The CRP levels were found to be significantly high in the situations in which AF is common. It is thought that CRP plays a role in the complement-mediated inflammation. 9 Frustaci et al 35 evaluated the atrial biopsies of patients with AF and found inflammatory infiltration, myocyte necrosis, and fibrosis. Similar findings were found in animal models developed by Nakamura et al; active atrial peri-myocarditis, inflammatory infiltration, lipid degeneration, and fibrosis were found in the dogs with AF. 36 In a retrospective, case–control study conducted by Chung et al with 131 patients with AF and 71 healthy individuals, it was found that AF was associated with doubled CRP levels. In that study, independent predictors of AF were found to be age, hypertension, dilated cardiomyopathy, female gender, and less powerfully high CRP levels. 37
The statins have anti-inflammatory effects, and presumed association of AF with inflammation has accelerated the researches about their effects on AF. Siu et al, in a retrospective study with patients with lone AF, showed that AF recurrences were lower among the patients given simvastatin or atorvastatin treatment before cardioversion in comparison with the patients who did not receive lipid-lowering medications (42% vs 84%, P = .032). 38
It is known that vitamin D suppresses pro-inflammatory cytokines and causes an increase in IL-10 levels. 6 Because of that effect, it is thought that vitamin D deficiency might be related to the development of and sustaining AF. Transforming growth factor β1 increases atrial fibrosis under normal atrial action potential and under normal ventricular structure and function. It also enhances conduction heterogeneity and increases the vulnerability to AF. It has been thought that vitamin D deficiency increased the vulnerability to AF by causing an increase in TGFB1 expression, enhancing atrial fibrosis, and conduction heterogeneity. Calcium plays an important role in initialization of AF and electrophysiological remodeling. It is known that PTH causes an increase in intracellular calcium levels via diminishing cellular calcium intake in the cardiomyocytes and reducing calcium reuptake to the sarcoplasmic reticulum. 39 Recently, Rienstra et al 40 suggested that vitamin D status was not related to incident AF, and in contrast, our study revealed a relationship between vitamin D deficiency and nonvalvular AF.
In our study, it was found that the LA and RA diameter was associated with AF, consistent with the literature data. When 3 groups were compared, PTH levels of patients with AF were significantly higher than PTH levels of the patients without AF (P = .002). This result suggests that hyperparathyroidism, secondary to vitamin D deficiency, plays a role in AF resulting in intracellular calcium overload.
As a result our study revealed a relationship between vitamin D deficiency and nonvalvular AF. But the vitamin D levels were found to be similar in patients with valvular AF with mitral valve disease and the control group. This situation suggests that the cause of AF is valvular heart disease in these patients. Additionally, vitamin D deficiency maybe cause of AF in the patients with nonvalvular AF.
In conclusion, it was found in our study that there might be an association between nonvalvular AF and vitamin D deficiency. The most important restriction of our study is the limited number of patients. There is a need for large-scale research into this issue.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.