
Abstract
Background: We aimed to verify safety and effectiveness of certoparin real-world use and to identify predictors of thromboembolic events or bleeding. Methods: This was a non-interventional study documenting patients at hospital- or office-based physicians. Results: Patients’ (n = 1407) mean age was 53.7 ± 16.1 years. Reason for certoparin use was prophylaxis of venous thromboembolism in 1331 (94.6%) patients and treatment in 76 (5.4%) patients. In only 11.4% of those receiving prophylaxis and 13.2% of those receiving treatment dosing, duration and schedule of certoparin were within label. There were 2 patients with deep venous thrombosis ([DVT], no pulmonary embolism [PE]), and 51 patients (3.8%) with minor (nonmajor) bleeding complications in patients receiving prophylaxis. Two patients treated with certoparin had recurrent DVT and one had PE (one patient with minor bleeding). Conclusions: Certoparin is very effective in real world. This also applies to patients in whom clinical decision making leads to an alteration of recommended application.
Introduction
Certoparin is registered for the prophylaxis and treatment of venous thromboembolism (VTE) in Germany. For this purpose, the recommendation is to use a dose of 3000 IU for a mean of 7 to 10 days for peri- and postoperative prophylaxis, 9 to 20 days in nonsurgical patients and 12 to 16 days in patients with stroke. For the treatment of VTE, a twice daily application of 8000 IU for 10 to 14 days is recommended. The registration further names a number of comorbid disease conditions and concomitant pharmacotherapy that may interfere with the efficacy and safety of certoparin and have to be considered when making a treatment decision to balance benefits and risks.
Because we found no data on a comparison of the recommended use of certoparin as to the summary of product characteristics (SPC) with real-world treatment decisions, we conducted a non-interventional study on office- or hospital-based physicians working in general-, orthopedic-, or trauma surgery, and on cardiologists. To identify predictors and specific real-world situations in which the balance between benefits and risk may be suboptimal, we captured patient characteristics, data on actual certoparin use, and the frequency of thromboembolic or bleeding complications in 1407 patients.
Within this context, there were a number of predefined objectives: (1) to determine the incidence of symptomatic thromboembolic events; (2) to determine the incidence of major bleeding complications; (3) to describe use of certoparin preparations, dosing, and duration of treatment in different indications and its comparison with SPC; and (4) to assess the timing of certoparin use before and after the surgical intervention.
Patients and Methods
Study Design
The PROMEMBER (Prospektive, nicht-interventionelle Studie zu Mono-Embolex in der Thromboseprophylaxe und Therapie) was a non-interventional, noncontrolled, prospective study in patients receiving the low-molecular-weight heparin certoparin for the prophylaxis or treatment of thromboembolic events. Patients were included by office- or hospital-based physicians working in general-, orthopedic-, or trauma surgery, or cardiology. The study was conducted in accordance with the German Medicines Law (§ 67 (6) Arzneimittelgesetz). Ethical approval was obtained by the ethics committee of the University of Ulm on May 22, 2009 and patients had to provide written informed consent.
Patients
Patients of either gender were eligible for inclusion into the study if they were at least 18 years old and the physician had selected certoparin for preventing or treating thromboembolic events. Patients were included on a consecutive basis per center involved aiming at largely preventing a selection bias. No other in- or exclusion criteria applied.
Documentation
Patients were documented at the start (baseline) and at the end of certoparin use. The following variables were collected at baseline: patient characteristics (year of birth, gender, body weight and height, relevant concomitant treatment, and smoking status), expositional and dispositional risk factors, laboratory parameters (hemoglobin, hematocrit, platelets, serum creatinine, activated partial thromboplastin time [aPTT], international normalized ratio [INR],
Statistics
This was a non-interventional epidemiologic study with a descriptive analysis. To estimate the number of patients to be included, we defined that we would like to observe adverse events with an incidence of 0.05% with a power of 80%, resulting in 3000 patients to be included by 300 physicians (10 patients each).
SPSS for Windows (release 18.0) was used for the statistical analysis. For categorical data, absolute and relative frequencies and for continuous variables, means with standard deviations or medians with quartiles were calculated. Continuous variables were tested according to Kolmogorov-Smirnov for normal distribution. Differences were tested for significance with the Student t test and the Mann-Whitney U test in case of 2 independent, normally distributed samples. In case of more than 2 independent, non-normally distributed samples, the Kruskal-Wallis H test was employed. Categorical data were evaluated with the chi-square test or the Fisher exact test. For correlations, Spearman rho was determined. Multivariable analysis was done employing binary logistic regression analyses with forward inclusion using likelihood ratio criteria (P ≤ .05).
Results
After the inclusion of 1407 patients, the study was stopped premature because of slow recruitment. Patients had a mean age of 53.7 ± 16.1 years (range 18-95 years), 50.4% being male and 23.4% smokers were included through 244 physician offices into this non-interventional study between September 16, 2009 and February 28, 2010. Patients had a mean body weight of 80.1 ± 15.2 kg and a body mass index (BMI) of 27.0 ± 4.6 kg/m2. Of these, 75.8% had dispositional risk factors, 49.2% expositional risk factors, and about half of patients reported to receive comedication potentially interfering with coagulation. In this study, we found factor V Leiden mutation in 3 patients (42.9%), hyperhomocysteinemia in 1 patient (14.3%), protein C deficiency in 1 patient (14.3%), antiphospholipid syndrome in 1 patient (14.3%), and other not specified defect in 1 patient (14.3%). Overall, we found 7 (100.0%) molecular thombophilias.
The reason for the initiation of certoparin was the prophylaxis of VTE in 1331 patients (94.6%) and the treatment of VTE in 76 (5.4%).
Certoparin for VTE Prophylaxis
A total of 1331 patients received certoparin prophylaxis because of orthopedic surgery (50.2%), general surgery (22.2%), and abdominal surgery (3.6%). A total of 24% of patients had other including nonsurgical reasons for prophylaxis. Anamnestic trauma or surgical intervention within the last 12 weeks (25.2%), obesity (22.0%), varicosis (20.1%), and age ≥ 70 years (13.5%) were the most frequent dispositional risk factors. Of all, 50.4% had expositional risk factors such as a surgical intervention >1 hour (23.8%); 21.5% received nonsteroidal anti-inflammatory drugs (NSAIDs; Table 1).
Patients Characteristics and Risk Factors in PROMEMBER (Expositional and Dispositional) for Thrombosis

Abbreviations: BMI, body mass index; NSAIDs, nonsteroidal anti-inflammatory drugs; SD, standard deviation; VTE, venous thromboembolism.
The mean duration of certoparin prophylaxis was 14.1 ± 16.5 days (Figure 1). Prophylaxis was started at a mean of 4.5 ± 8.2 hours before surgery (median 1 hour) and reintroduced at a mean of 13.0 ± 12.0 hours after the intervention. The majority of patients (n = 1203; 90.4%) received the 3000 IU prophylactic dose of certoparin. Of all, 9.6% received a higher dose (>3000 IU), 39.6% and 25.6% for a reduced duration in surgical and nonsurgical patients, respectively (Table 2).

Duration of prophylaxis depending of the surgical field. Interventions were classified as general- (varicosis, hernia, thyroid gland surgery, etc), abdominal- (abdominal interventions only), neuro-, orthopedic-, or other surgery or because of a medical reason. Boxes illustrate medians with interquartile distance (median; 25/75 percentile), lines include all values (minimum to maximum). Outliers are illustrated as circles (1.5×-3× length of the box) or stars (>3× the box length).
Certoparin Preparations, Dosing, and Duration of Prophylaxis and Treatmenta

a11.4% of patients had a recommended dosing, duration, and schedule of certoparin prophylaxis throughout; 13.2% of patients had a recommended dosing and duration of certoparin treatment throughout.
A total of 2 patients had confirmed thromboembolic events (DVT no PE) despite certoparin prophylaxis. Both patients underwent orthopedic surgery. With regard to the Wells score, the criteria of edema, pain, swelling of the lower leg, and surgical intervention <12 weeks—each of them—were found in 50% of the patients. None of these patients received further investigations to verify the findings. Two patients had an ischemic stroke (Table 3). While there was no case of major bleeding, 51 patients (3.8%) had any minor bleeding complication. None of the 7 contemplated patients with thrombophilia had bleeding complications.
Thromboembolic Events and Bleeding Complications

aTwo patients had ischemic stroke.
Certoparin for VTE Treatment
A total of 76 patients received certoparin treatment because of DVT (n = 75) and PE (n = 2); 1 patient had both DVT and PE. A history of VTE (44.7%), obesity (34.2%), aged ≥ 70 years (32.9%), and varicosis (19.7%) were the most frequent dispositional risk factors, stroke was the most frequent expositional risk factor (15.8%). Of all, 15.8% received platelet inhibitors as concomitant pharmacotherapy (Table 1).
The mean treatment duration was 14.1 ± 16.5 days (median 9 days and maximum 163 days). Treatment was initiated at a mean of 4.5 ± 8.6 hours (the majority of which <3 hours) after first diagnosis and a maximum of 48 hours. Of all, 50% of patients (n = 38) received a half-therapeutic dose of 8000 IU and 50% a full-therapeutic dose of 2 × 8000 IU. Of all, 26.3% received treatment for duration of less than 10 days (Table 2).
Two patients had confirmed recurrent DVT and one PE. With regard to the Wells score, the criteria of edema was found in 50% of the patients. Of all, 50% received duplex sonography and 50% received compression ultrasound. The patient with both DVT and PE received lung scintigraphy. Of the 76 patients, 1 had minor bleeding complications (none major; Table 3).
Predictor Analysis for Minor Bleeding Complications
Upon univariable analysis of all 1407 patients for risk factors influencing the risk of (minor) bleeding, we identified a BMI <29 kg/m2 (odds ratio [OR] 2.858), NSAID use (OR 3.477), and major surgery >1 hour (OR 3.827) to predict bleeding complications (Figure 2). In a multivariable analysis, the association with NSAID use (P = .001) and major surgery >1 hour (P = .006) remained significant and a hematocrit at baseline lesser than or equal to the median became significant (P = .039).
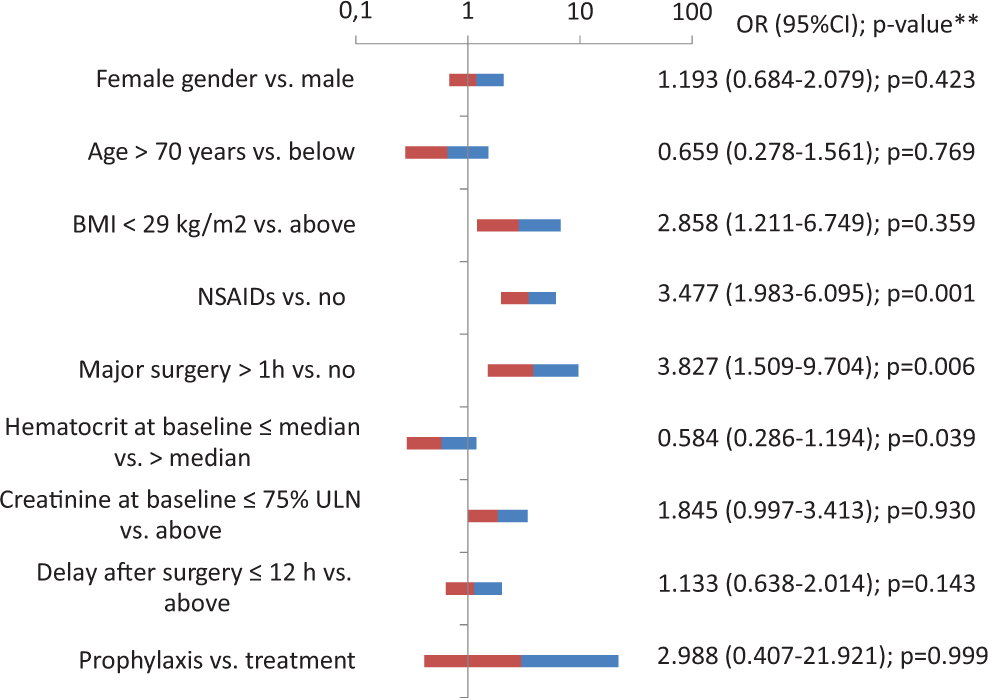
Predictors of bleeding complications (only patients with minor bleeding were considered because there was no patient with major bleeding). Odds ratios with confidence intervals >1 that, for example, NSAID use confers a higher risk of bleeding complications than no NSAID use; **from binary logistic regression analysis for which only 292 of 1407 patients were available; BMI indicates body mass index; NSAID, nonsteroidal anti-inflammatory drugs; ULN, upper limit of normal; OR, odds ratio; CI, confidence interval.
Discussion
The present analysis of 1407 patients receiving certoparin for the prophylaxis or treatment of VTE demonstrates that there is a difference between the patient population studied and the dosing or duration used in clinical trials (determining the recommendation in the SPC) as compared to a real-world situation. This may be exemplified by the high proportion of patients with concomitant medication interfering with coagulation (which is not forbidden by the SPC but warrants caution and is much higher in real world than in clinical trials), the high proportion of surgical patients receiving less than 7 days of certoparin prophylaxis (39.6%), and the quarter of nonsurgical patients receiving less than 9 days of prophylaxis (25.6%). On the other hand, prophylaxis is prolonged (beyond the SPC defined treatment duration) in a substantial proportion of patients which is appropriate as to the guidelines 1 has been demonstrated to be effective for certoparin in surgical patients 2 but is not covered by the label of certoparin. Against this background, it is reassuring for clinicians to see that thromboembolic events are the exception (2 patients with DVT of 1331 patients) and that there were only minor bleeding complications (51 of 1331 patients).
Clinical Effectiveness of Certoparin Prophylaxis
The efficacy of certoparin to prevent VTE has been documented for patients undergoing orthopedic surgery, where the rates of thromboses ranged from 10% to 32%, 2 –4 abdominal surgery (0.0% and 10.8% 5 –8 ), and ambulatory interventions (arthroscopy; 0% and 0.15% 9,10 ). Against this background, we documented 2 patients with VTE corresponding to 0.15% and this is compatible with the later reports mostly in ambulatory patients. 6,7,9,10
There are a number of aspects that might put into perspective the low thrombosis rates seen in our study. First, the patient population in PROMEMBER was very heterogeneous because patients were recruited in the hospital as well as in the ambulatory setting. Second, the interventions covered a range from trauma surgery to less invasive procedures such as arthroscopy or coronary interventions. Third, we only documented symptomatic thromboembolic events and performed no systematic evaluation with respect to asymptomatic events as has been the case in controlled trials. Taken together, this might implicate that we have documented a lower bound estimate of the true event rate in a mixed population given that we had less severe interventions and partially asymptomatic events.
Rates of any bleeding in clinical studies ranged around 3.4%. 6 There were no major bleeding complications in our documentation but 3.8% had minor bleeding.
Clinical Effectiveness of Certoparin Treatment
The evaluation of certoparin for the treatment of VTE in PROMEMBER is limited when the less number of patients were included (n = 76). These patients were older, had a higher BMI, and a considerable risk of VTE. Two of these patients had recurrent DVT (2.6%), 1 patient PE (1.3%), and 1 patient had minor bleeding (1.3%; no major bleeding). Thromboembolic event rates were higher than results of the EASTERN study, in which no patients out of 273 had a recurrent thrombosis with certoparin. 11 Bleeding rates were low compared with prior randomized controlled trials as the one by Harenberg in which 3.5% of 893 patients with acute symptomatic proximal DVT had major bleeding. 12 It was also low compared with a prior study in 11 LMWH-treated patients where 1.5% experience major bleeding. 13 However, the results have to be considered with caution. The total patient number results in a wide confidence interval and thus, the true event rates might differ considerably. Further 50% of patients received a reduced dose of <2 × 8000 IU and 26.3% had their certoparin applied for less than the recommended duration of 10 to 14 days.
Real-World Use of Certoparin
A further important finding from PROMEMBER is that a substantial proportion of patients receiving certoparin for the prophylaxis or treatment of thromboembolic events in real world were not treated within the recommendations of the current labeling.
When conducting a predictor analysis for the occurrence of any bleeding complications, we identified major surgery >1 hour and NSAID use to be associated to an increased risk. While prolonged major surgery usually cannot be avoided, this is less so for NSAIDs (ibuprofen, etc) which might be temporarily discontinued when anticoagulation becomes necessary.
Actual certoparin dosing and duration of prophylaxis were different in real world than in the SPC with about 10% of patients receiving higher than recommended doses, 25% to 40% receiving less than recommended duration, and 30% to 39% receiving a prolonged prophylaxis. This is likely based on the physician’s assessment as to the type of intervention/surgery and the assumed thromboembolic risk: patients receiving a reduced duration of prophylaxis might have undergone less severe interventions (such as arthroscopy) and one might question whether or not the particular patient should have received any prophylaxis. On the other hand, a prolonged prophylaxis (30%-39% of patients) has been, while not being covered by the labeling, documented to be effective in clinical studies 2 and recommended in current guidelines 1 because of the persistently elevated thromboembolic risk.
Limitations
PROMEMBER is a prospective, non-interventional study on the real-world use of certoparin in daily practice. It benefits from a large patient number although initial recruitment targets were no met. It does, however, have limitations inherent to many real-world studies, for example, no perfect completeness of patient data, the potential of unknown bias, no control group, and no end point validation. While these limitations may quantitatively influence the results, we expect no qualitative changes. Whether or not patients with thrombophilia are any different than other patients cannot be answered from the present data set because 95% confidence intervals are wide and overlap with each other.
On the other hand, the real-world approach allows to investigate issues such as compliance of use with indications that are not possible in more stringent study designs such as randomized controlled trials.
Conclusion
Taken together, it appears that certoparin, used for the prophylaxis and treatment of thromboembolic events, is very effective in a real-world situation. This finding is even more important because it also applies to patients in whom clinical decision making leads to an alteration of the recommended dosing schedule.
Footnotes
Acknowledgments
The support of the participating physicians, their staff, and patients is acknowledged.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Michael Spannagl, Peter Bramlage, and Ralf Eisele have received research support and honoraria for consultancy from Novartis. Cornelia Englert was paid consultant for the analysis of the data during her employment at the Juwi MacMillan Group. Nima Melzer is an employee of the sponsor.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the study was sponsored and conducted by Novartis Pharma GmbH, Nürnberg, Germany.