
Abstract
Antibodies to the heparin/platelet factor 4 complex (heparin/PF4) are linked to the pathogenesis of heparin-induced thrombocytopenia (HIT) and to the thrombotic complications. We investigated thrombotic events during early follow-up in a pediatric cardiac surgical population to ascertain whether there is a relation between heparin/PF4 antibody concentration and post-surgical thrombotic complications. One hundred and five consecutive pediatric patients treated by Fontan surgery were studied. The presence of serum heparin/PF4 immunoglobulins IgG, IgA, and IgM (collectively termed HIT antibodies) were measured in preoperative and postoperative blood samples by enzyme-linked immunosorbent assay. On day six after Fontan surgery, HIT-related thromboses was identified in total of 11 patients (10.5%). HIT antibodies were detected in 34 of 105 patients (32.4%). The post-surgical nadir platelet count was significantly lower in patients who developed antibodies (p < 0.001). We found the odds ratio (OR) for this composite endpoint was 4.06 (p < 0.001). Seropositive status for heparin/PF4 antibodies was an independent predictor of thrombotic events (OR 2.28; p < 0.001). Quintile analysis revealed that the median nadir platelet value was significantly lower in patients with higher HIT antibody titers. Patients in the highest quintile of HIT antibody titer all experienced thrombotic events, while only two thrombotic events occurred in patients in the lowest quintile (p < 0.001). Heparin-induced thrombocytopenia is a rare occurrence in pediatric cardiac surgical patients. Patients who develop antibodies to the heparin/PF4 complex have a significantly higher rate of postoperative thrombotic events than patients who lack these antibodies. Within the seropositive group, the risk of developing thrombosis increased with the plasma antibody concentration.
Keywords
Introduction
The Fontan procedure is the last-stage operation for children born with congenital heart disease for whom the 2-ventricle repair would not be effective. Since its original description, many modifications to the procedure have resulted in improved survival, but thromboembolic events are still a major cause of morbidity and mortality. 1 Some clinicians have advocated anticoagulation treatment with heparin for all the patients after the Fontan operation in order to prevent thrombus formation. 2,3 However, heparin may have serious side effects, including heparin-induced thrombocytopenia (HIT). 4,5 The HIT is an immunoglobulin G (IgG)-mediated disorder. Patients with HIT may develop multiple and recurrent arterial and venous thromboembolism. Thus, heparin may paradoxically cause the same complications that it is intended to prevent.
In the previous retrospective studies of adults, the occurrence of HIT after heart surgery was associated with high postoperative mortality and increased incidence of arterial and venous thromboembolic events at short-term follow-up. 6,7 Similarly, patients who developed antibodies against the heparin/platelet factor 4 (PF4) complex following heparin treatment for acute coronary syndrome exhibited a high risk of myocardial infarction. 8 In a previous study of patients with acute coronary syndromes, they found a higher risk of thrombotic events in those patients who developed heparin/PF4 antibodies. 9 The postoperative frequency of HIT varies from 27% to 50% of cardiac surgery patients with heparin/PF4 antibodies, which are detected by enzyme immunoassay. 10 –12 The relationship between the heparin/PF4 antibody serum titer and thrombotic events in Fontan surgery patients has not been studied, although the prognostic significance of these antibodies is well established.
The aim of the present study was to investigate thrombotic events in a pediatric population following Fontan surgery with intraoperative heparin administration and to determine whether there is a significant relationship between HIT antibody concentration and these events.
Materials and Methods
The study protocol was reviewed and approved by the Committee on Human Investigations at Shanghai Children’s Medical Center of China. Informed written consent was obtained from the parents of all the patients.
A total of 105 consecutive patients were studied. Detailed clinical data were recorded for each patient, including type of disease, previous catheterizations, cardiopulmonary bypass time, aortic cross-clamp time, as well as drug treatment during the operation. Patients receiving anticoagulant medications other than unfractionated heparin (UFH) at the time of the study and those with a known history of hematological disorders were excluded. Porcine mucosal UFH was given intraoperatively at an initial dose of 50 U/kg to a maximum of 5000 U as an intravenous bolus followed by a continuous infusion at a dose of 10 U/kg per h while monitoring activated partial thromboplastin time. The choice of background therapy was left to the discretion of the treating physician. Demographic data and surgical details are summarized in Table 1.
Clinical Characteristic of Patients
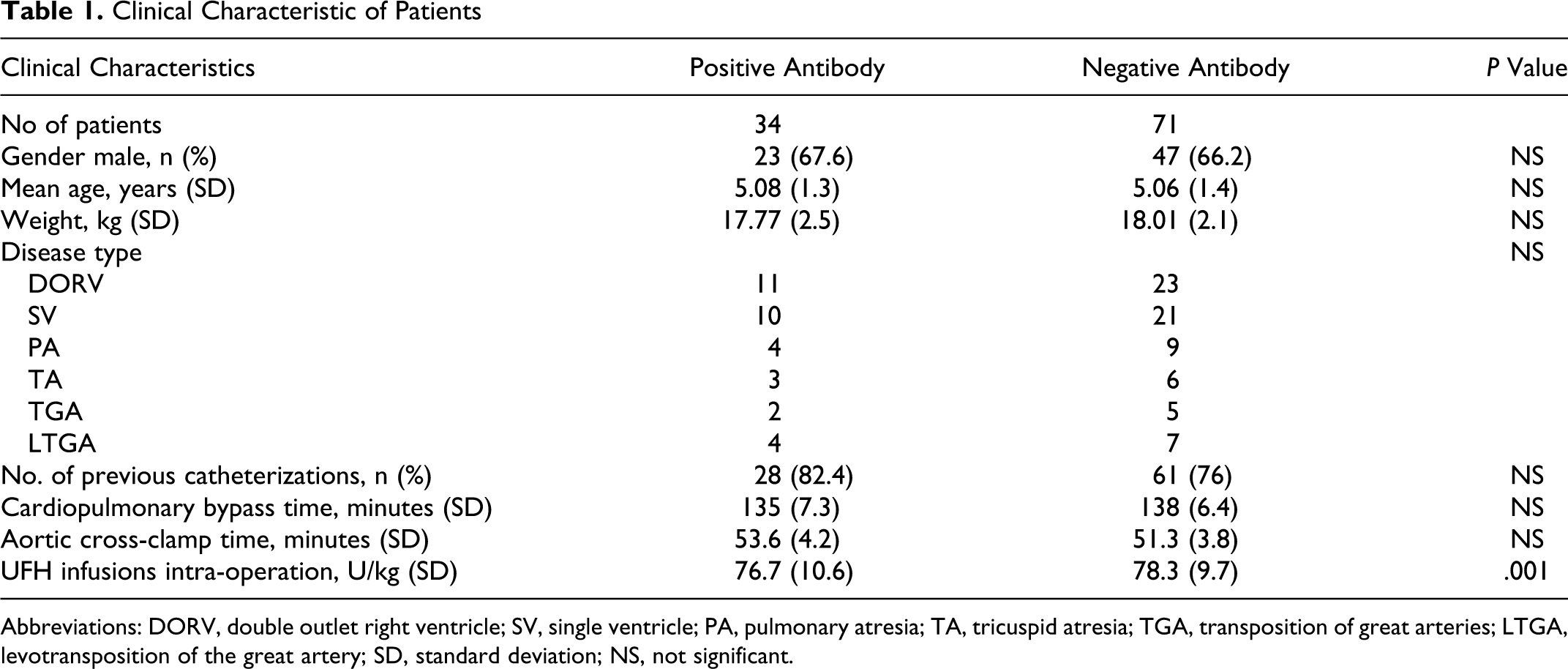
Abbreviations: DORV, double outlet right ventricle; SV, single ventricle; PA, pulmonary atresia; TA, tricuspid atresia; TGA, transposition of great arteries; LTGA, levotransposition of the great artery; SD, standard deviation; NS, not significant.
Platelet counts were measured preoperatively and daily in the postoperative period as part of routine clinical care. Blood samples were taken at the time of hospitalization and 6 days after surgery for the analysis of heparin/PF4 antibodies (IgG, IgA, and IgM antibodies) using a commercially available enzyme-linked immunosorbent assay (ELISA) kit (Asserachrom HPIA kit, Diagnostica Stago, Parsippany, New Jersey), according to the manufacturer’s instructions. Briefly, duplicate samples of plasma from each patient were incubated for 1 hour at room temperature in plastic microwell plates coated with heparin-PF4 complex. Plates were then washed 5 times with a trisodium citrate buffer plus goat serum. Peroxidase-conjugated goat antibodies to human IgG, IgA, and IgM were added to each well and incubated for 1 hour at room temperature. After 5 washes in trisodium citrate buffer, diluted ortho-phenylenediamine dihydrochloride and urea peroxide were added to each well to activate chromogenic peroxidase activity. After 5 minutes, the color reaction was stopped by the addition of sulfuric acid. The optical density (OD) at 492 nm was measured after 10 minutes. A positive test was defined by the manufacturer as an OD of 29% or more than the positive control. Each assay was run with negative and positive controls in duplicate.
Thrombocytopenia was defined by at least 2 consecutive platelet counts below 150 × 109 per L or a decrease below 50% of the initial value at hospitalization. 9,10 The HIT was defined when a patient with thrombocytopenia was also positive for HIT antibodies by immunosorbent assay.
Data were analyzed using Stata 7.0. Continuous variables are presented as mean (±standard deviation [SD]) and group means were compared using Student t tests. The cumulative proportion of patients who had a thrombotic event over time was estimated by the Kaplan-Meier method, and statistical comparisons were made using the log-rank test. Categorical data (proportions) were compared statistically using the McNemar test. Cox proportional hazards regression was used to relate HIT antibody titer to the primary outcome all-cause mortality. We also evaluated the correlation between antibody titer (OD of the ELISA assay) and thrombosis, and the P value for the trend was calculated from regression with continuous variables. Pearson correlations were calculated to examine the univariate relationship between antibody titer and continuous variables. Differences in thrombotic events among antibody titer quintiles were compared by the analysis of variance (ANOVA). Multiple logistic regression analysis was performed to identify independent predictors of thrombotic events. Candidate variables included age, gender, weight, disease type, previous catheterizations, cardiopulmonary bypass time, aortic cross-clamp time, UFH infusions, positive status for heparin/PF4 antibodies on postoperative day 6, and admission platelet counts in the ranges 150-200 × 109 per L, 200-250 × 109 per L, and more than 250 × 109 per L. A P < .05 was considered statistically significant.
Results
At day 6, after Fontan surgery, heparin/PF4 antibodies were detected in 34 patients (32.4%) by ELISA assay. Mean baseline platelet count at hospitalization was similar in patients who eventually developed antibodies compared with those who did not (185 (51) × 109 per L vs 200 (49) × 109 per L; P = not significant [NS]). The mean nadir platelet count was significantly lower in patients who developed antibodies (76 (29) ×109 per L vs 100 (50) × 109 per L, P < .001). There are 24 patients with HIT. The HIT-related thromboses were identified in a total of 11 patients. Hence, the overall prevalence of thrombus formation in our population was 10.5%. The vascular location for all HIT-related thromboses was evenly distributed between arterial (2 patients, 18%) and venous (9 patients, 82%) systems.
Global analysis of incidence of events in patients with and without HIT antibodies revealed significant difference between the 2 groups in composite mortality and embolic events as determined by the log-rank test. We found an increased risk of embolic events and death in patients positive for HIT antibodies; the odds ratio (OR) for this composite end point was 4.06 (95% confidence interval [CI]: 1.85-9.37; P < .001).
Multiple logistic regression analysis revealed that antiheparin/PF4 positive status was an independent predictor of thrombotic events (OR: 2.28; 95% CI: 1.96-4.31 P < .001). The presence of HIT antibodies predicted thrombotic events independently of baseline platelet count.
In patients with a positive ELISA test at 6 days after Fontan surgery, OD at discharge averaged 0.817 (0.526) OD units compared with 0.129 (0.141) OD units in the antibody-negative patients. Patients were then stratified in quintiles according to their OD value. Median OD was 0.211 units and the 25th and 75th percentiles were 0.001 and 1.189 OD units, respectively. By quintile analysis, the median nadir platelet value decreased significantly with increasing OD quintile (Figure 1). Mean OD was 0.909 (0.668) units in individuals with thrombosis versus 0.209 (0.226) units in patients who remained free of thrombotic complications (P < .001). By quintile analysis, patients with higher OD values were at significantly greater risk of thrombosis; using quintiles of OD, the ORs (95% CI) for the risk of thrombosis were 1.03 (0.24-2.48) in the second quintile, 2.25 (1.89-3.69) in the third quintile, 5.08 (2.37-7.13) in the fourth quintile, and 7.63 (3.98 to 9.15) in the fifth quintile (P < .001 for the trend). All patients in the highest quintile experienced 8 thrombotic events, compared with only 2 patients in the lowest quintile (P < .001; Figure 2).
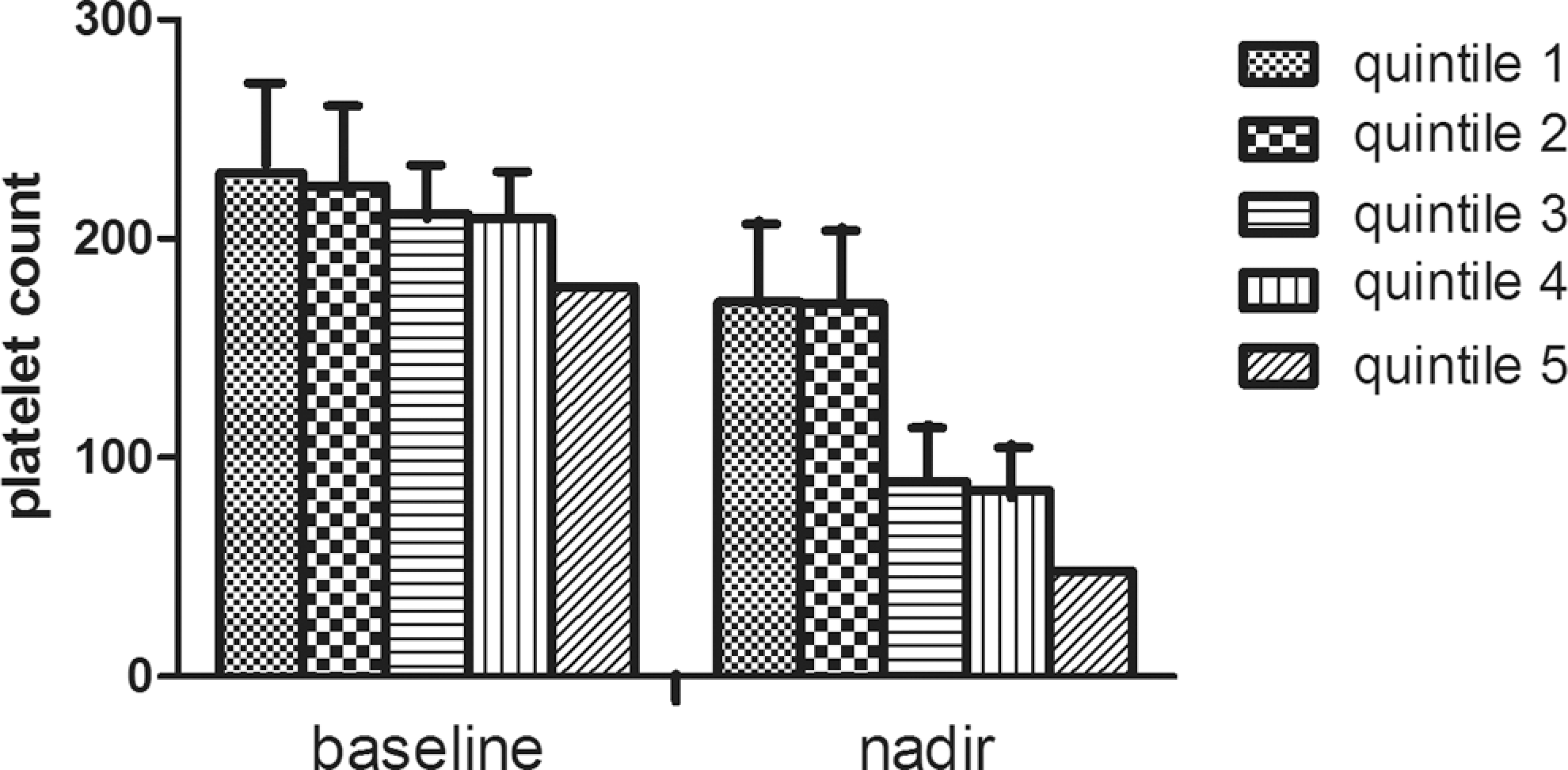
Distribution of platelet count in patients categorized according to quintiles of optical density. The nadir platelet counts decreased with increasing optical density value.
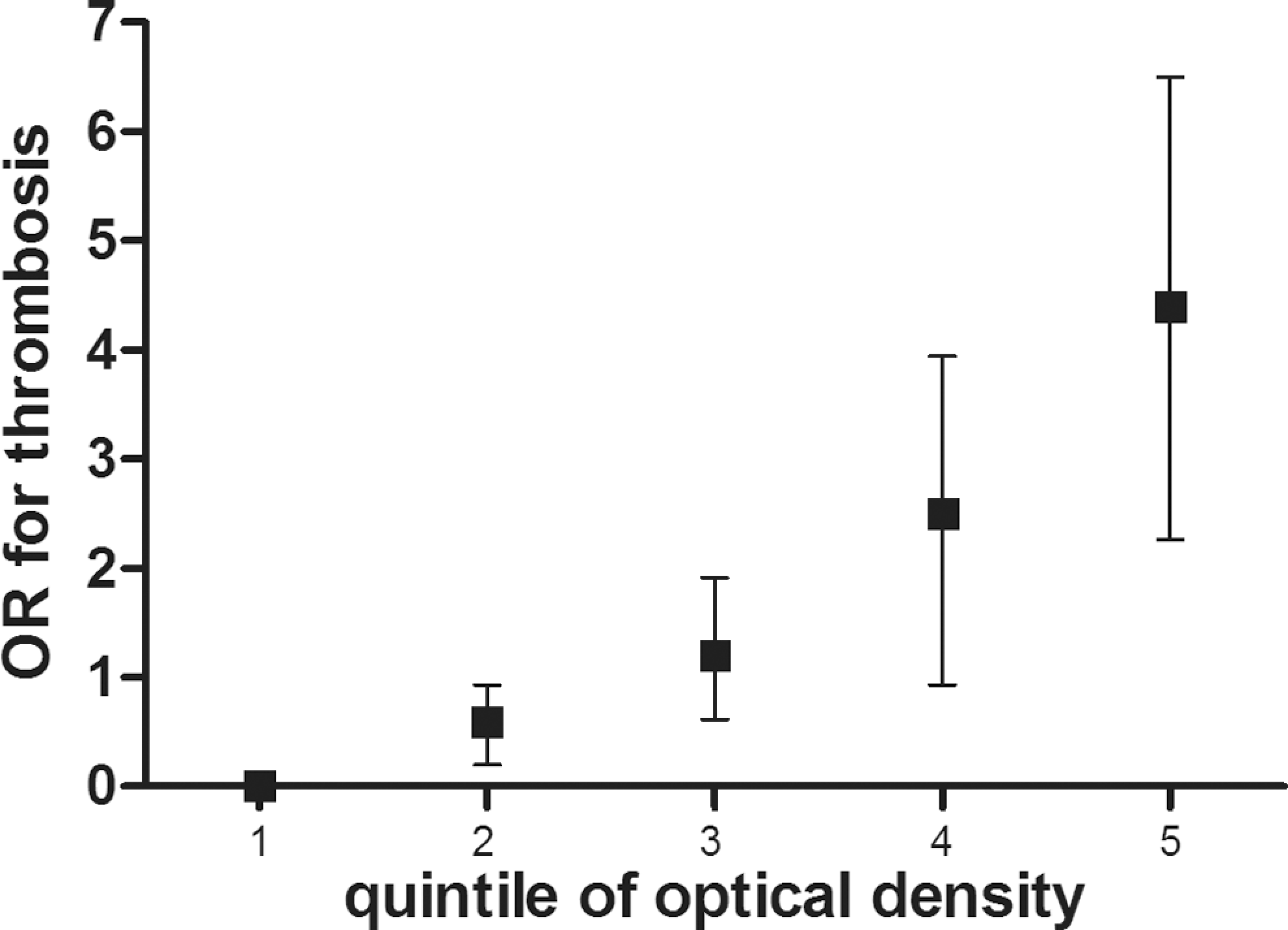
Risk of thrombosis in patients categorized according to quintiles of OD. The risk of developing thrombosis increased with increasing OD of antibodies. OR indicates odds ratio; OD: optical density.
Discussion
Thrombocytopenia is a serious complication in patients with cardiac disease. Patients with HIT have an increased rate of bleeding complications, ischemic events, and early mortality. 13 Vanderschueren and coworkers evaluated the prognostic significance of thrombocytopenia in adult patients admitted to an intensive care unit and found that it was a powerful predictor of adverse events. 14 A similar finding was reported by Overgaard et al in adult patients referred for percutaneous coronary interventions. In this case, baseline thrombocytopenia was an independent predictor of in-hospital mortality. 15
This prospective analysis suggests that HIT is a rare event in pediatric cardiac surgical patients. The incidence of antiheparin/PF4 antibody seroconversion in older pediatric cardiac surgical patients is approximately 50% at 10 days postsurgery, similar to that reported in adult cardiac surgical patients. 16 Both the age and the previous exposure to UFH are correlated with the rate of seroconversion in adult patients. In contrast, the rate of seroconversion in the neonatal population was substantially lower.
The major finding of the present study is that the children who develop antibodies against the heparin/PF4 complex had a significantly higher rate of postoperative thrombotic events than those who lacked these antibodies, and the risk of thrombosis increased with antibody titer. Antibodies to heparin/PF4 were detected in 32.4% of our patients treated with UFH during Fontan surgery. Cardiopulmonary bypass is known to induce strong platelet activation and the release of a large amount of PF4 into the plasma. This is one possible reason for the high frequency of HIT IgG detection after cardiac surgery. Bauer et al found that 50% of adult patients undergoing cardiopulmonary bypass had HIT antibodies postoperatively as detected by antigen assay. 12 However, Selleng et al have prospectively screened 581 cardiac surgery patients for heparin-dependent antibodies by PF4-heparin immunoassay and platelet activation test and performed daily platelet counts (until day 10) with 30-day follow-up and suggested that early-onset and persisting thrombocytopenia in postcardiac surgery patients are rarely due to HIT, even when antibody tests are positive. 17 One possible reason is that the typical onset of HIT coincides with the time period in which the platelet count typically falls to thrombocytotic levels due to perioperative hemodilution. In fact, recent guidelines suggest that clinicians should consider a fall in the platelet count to 50% of baseline between postoperative days 5 and 14 to represent potential HIT and should order prompt laboratory investigations for HIT antibodies. 18
In the present study, antibodies to the heparin/PF4 complex were detected using an antigen assay. Both the functional platelet activation assays and the antigen assays are very sensitive detection methods for HIT antibodies. Antigen assays detect all antibody classes (IgG, IgA, and IgM) to the heparin/PF4 complex but are less specific than functional assays for detecting clinically relevant antibodies. 19 In contrast, platelet activation assays, such as the serotonin-release assay, exclusively detect platelet-activating antibodies of the IgG class. Therefore, platelet activation assays have much higher specificity for detecting clinically relevant antibodies. The accurate performance of these functional assays, however, requires experienced staff and is restricted to only a few laboratories. 20 The test we used detects antibodies of all 3 Ig classes, but mainly the platelet-activating IgG class. 21 , 22 The diagnostic interpretation of the test was performed in the context of platelet counts, however, as both a 50% drop in platelet count and heparin/PF4 antibody positive status were required for a HIT diagnosis. Prospective data indicate that an increased risk of thrombosis occurred in adult patients whose platelet count had fallen in relation to HIT antibody formation. 23
The specificity of this assay for clinical HIT increases in relation to the magnitude of the OD of the ELISA test, especially when OD >1.0. 24 We found a significant relationship between the OD of the ELISA reaction and thrombosis. In vitro studies have demonstrated that platelet aggregation in HIT patients is dependent on the relative quantity of heparin/PF4 antibodies, which is consistent with our observation that patients with higher ODs had a significantly higher number of thrombotic events. 25
More recently, Chan et al suggested that further reliance on the OD value may not allow one to reliably exclude HIT in adult patients undergoing cardiac surgery when OD is already known to be >0.4. However, their results should not infer other populations because of some significant limitations. 26 To our knowledge, a few retrospective studies from adult patients have also evaluated the relationship between HIT antibody concentration and the risk of thrombosis. Pena de la Vega and coworkers found that higher concentrations of HIT antibodies were associated with increased cardiovascular complications and pooled mortality in chronic hemodialysis adult patients. 27 Higher antibody levels were also associated with elevated circulating markers of thrombin generation in patients with suspected HIT. 28 A retrospective study by Zwicker and coworkers found that the thrombosis in adult patients had higher ELISA OD values (a higher HIT antibody titer). 24 They identified a threshold OD and found a near 6-fold increase in the risk of thrombosis in those with OD values >1.0.
On the basis of these earlier observations, we hypothesized that antibody titer could predict which Fontan surgery patients were at higher risk of postoperative thrombosis. A sensitive and specific ELISA assay to detect heparin/PF4 IgG antibodies was used. Our results demonstrated that HIT-related thromboses were identified in a total of 11 patients (10.5%) and that the risk of thrombosis increased with higher quintile of ELISA OD (antibody titer). Indeed, all the patients in the highest quintile experienced thrombotic events, representing a near 7-fold increased risk of thrombosis compared with patients in the lowest quintile.
In conclusion, exposure to heparin is associated with a substantial risk of developing antibodies to the heparin/PF4 complex (HIT antibodies). Appearance of HIT antibodies predicts lower postoperative platelet counts (thrombocytopenia) and the frequency of thrombotic events. Detection of HIT antibodies after cardiopulmonary bypass surgery suggests that reexposure to heparin should be avoided in these patients and that they should be managed as a high-risk group for thrombotic events.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.