
Abstract
In addition to potentially sharing common pathogenesis and clinical manifestations, venous and arterial thromboses might have overlapping risk factors. To evaluate the family history of myocardial infarction (MI) as a risk factor for venous thromboembolism (VTE) among whites and blacks, we analyze data from the Genetic Attributes and Thrombosis Epidemiology (GATE) study. Results indicate that the association between VTE and a family history of MI is statistically significant only among whites (odds ratio [OR] = 1.3; 95% confidence interval [CI] = 1.03-1.8), particularly when they have diabetes mellitus (OR = 3.1; 95% CI = 1.2-8.0). Among blacks, the association between VTE and a family history of MI is not statistically significant (OR = 1.2; 95% CI = 0.89-1.5) either among those with diabetes or those without diabetes. We conclude that a family history of MI is a risk factor for VTE among certain populations stratified by race and comorbid conditions.
Introduction
The clinical link between arterial and venous thrombotic disorders was identified in a case–control study of patients with deep vein thrombosis (DVT) and subclinical atherosclerosis. 1 Subsequently, the first prospective study evaluating the incidence of cardiovascular events after an episode of acute venous thromboembolism (VTE) was conducted and findings indicated a significant association between the incidence of cardiovascular events and acute pulmonary embolism (PE). 2 It was then suggested that venous and arterial thromboses might be part of a continuous spectrum of the same disease, 3 a hypothesis supported by the concept that inflammation and coagulation are interrelated. 4 Further studies have reported a positive association between DVT or PE, or both, and symptomatic atherosclerosis, 5 –7 or markers for risk of arterial thrombosis. 8 There is inconsistent evidence, however, that arterial disease is a risk factor for VTE 9,10 or that venous thrombosis is a risk factor for arterial disease. 9,11
Atherosclerotic disease and VTE potentially share a common pathogenesis and clinical manifestations and additionally might have overlapping risk factors. 9,10,12 Mechanisms implicated in both arterial and venous thrombosis include endothelial injury, platelet activation, elevated levels of intrinsic clotting factors and inflammatory markers, increased fibrinogen, and impaired fibrinolysis, resulting in thrombus formation in both arteries and veins. 9 Other environmental factors associated with arterial and venous thromboses include older age, obesity, smoking, diabetes mellitus, arterial hypertension, dyslipidemia, and hormonal determinants. 9,13,14 There is strong evidence that inflammation and thrombosis are implicated in the complications of diabetes and play a role in the development of its vascular complications. 4,15 Studies have shown that high plasma fibrinogen levels are associated with insulin resistance, a condition characterized by impaired glucose tolerance, and might be risk factors for developing type 2 diabetes in individuals. 16,17
Family history of VTE is an established risk factor for VTE among blacks and whites. 18 –21 To investigate the effects of traditional cardiovascular risk factors and family history of myocardial infarction (MI) on the incidence of VTE, Braekkan et al 22 conducted a prospective, population-based study involving 21 330 adults residing in Tromso, Norway. Their findings indicated that a family history of MI in one or more first-degree relatives with a history of MI before the age of 60 was a risk factor for both MI and VTE. These findings provide evidence of a link between arterial and venous thromboses. Two other prospective studies have investigated the effects of family history of MI on the risk of VTE, one conducted in Norway 23 and one in Sweden. 24 In both studies, there was a slightly increased risk of VTE associated with a family history of MI either among first-degree relatives before the age of 6023 or among parents. 24 Furthermore, in a recent report describing findings from a case–control study, Mili et al 21 found that certain comorbid conditions could further increase the risk of VTE associated with a positive family history of VTE. In addition, it is known that a family history of MI is a risk factor for future MI. 25,26
To examine the association between VTE and a family history of MI among whites and blacks and to confirm the Northern European studies’ findings among whites, 22 –24 we analyzed data from the Genetic Attributes and Thrombosis Epidemiology (GATE) study. 21,27,28 The GATE study is a matched case–control study of VTE designed to evaluate the roles of genetic polymorphisms and environmental factors and their interaction in the etiology of VTE; the study also compares risk factors for VTE between blacks and whites. The objectives of our report were to evaluate a family history of MI as a risk factor for VTE among blacks and whites and to assess whether such an association would be modified by other risk factors for VTE.
Materials and Methods
Study Population
The GATE study has been described in detail elsewhere. 21,27,28 This current analysis used data collected for adults aged 18 to 70 years enrolled in Atlanta, Georgia, from March 1998 through September 2005 and comprised 1145 VTE case and 1309 control patients. Case patients were adults with an objectively confirmed first or recurrent episode of DVT or PE ascertained from anticoagulation clinics at 2 Emory University hospitals. Case patients included people with idiopathic VTE, as well as those who developed a VTE following surgery, pregnancy, prolonged bed rest, or treatment for cancer. Case patients were hospitalized at 1 of the 2 hospitals and interviewed during their hospitalization. Control patients were concurrent with case patients and selected from a list of patients seen by primary care physicians at an Emory Healthcare clinic. The list was sampled to obtain potential control participants frequency-matched with the case patients for race, sex, and age (in 5-year age groups). Control patients with a history of VTE were excluded, as were control patients taking an anticoagulant medication or those with mental impairment. Control patients were invited to the Centers for Disease Control and Prevention (CDC) laboratories to provide a blood specimen and to complete the interview portion of the study.
Family History of MI
Case and control patients were interviewed at the time of enrollment about lifestyle characteristics (eg, oral contraceptive use, smoking, and drinking), general medical history, and family history of thrombosis. Study participants were asked whether their parents, siblings (brothers or sisters), or offspring, or any combination thereof, had had a heart attack, and, if so, the age at which their family members had a heart attack for the first time. Respondents were classified as having a positive family history of MI if they reported a history of a heart attack in at least one first-degree relative. A positive family history of MI could have included relatives with missing information, as long as at least one relative was identified with a positive history. Family history of MI was defined as negative only if all first-degree family members were reported as not having experienced a heart attack. We excluded 123 participants from the analysis who did not identify a relative with a positive family history of MI and were missing information on any first-degree relatives. We also considered 2 additional family history of MI variables that reflected a strong predisposition to VTE. We defined a strong positive family history of MI as a reported history of a heart attack either among any first-degree relatives before the age of 50 or among multiple relatives regardless of age. 18,21
Statistical Analysis
We compared the distributions of selected demographic and behavioral variables for case and control patients using chi-square tests. We computed odds ratios (ORs) to estimate the risk of VTE associated with a positive family history of MI, 95% confidence intervals (CIs) for the ORs, and 2-tailed P values using conditional logistic regression for matched data. The matching variables were race, sex, and age (the latter having 4 categories based on quartiles: 18-39, 40-49, 50-59, and ≥ 60 years). The ORs were interpreted as the risk of VTE for people with a positive family history of MI divided by the risk of VTE for people with a negative family history of MI. We ran the analyses separately for whites and blacks. Also, using conditional logistic regression models, we investigated whether race interacted with a family history of MI in their relationship with VTE. The P value for the product term was used to test for a statistical interaction with a significance level of P ≤ .05.
In addition, we compared the association of VTE and a family history of MI variable by categories of determinants that are known to be associated with DVT or PE, or both, including plasma fibrinogen levels (≥3 vs <3 g/L), 29 and comorbid conditions (obesity [body mass index ≥ 30.0 kg/m2), diabetes mellitus, clinical or self-reported hypertension, and cancer [excluding nonmelanoma skin cancer]). 21 We also examined the association between a family history of MI and the type of VTE, including DVT only or PE only. We assessed potential confounding by education, smoking, physical inactivity, blood type, oral contraceptive use, menopausal status, hormone replacement therapy, obesity, diabetes mellitus, hypertension, cancer, heart disease, kidney disease, lupus disease, and antiphospholipid syndrome. We ran the analyses for each ethnic group using conditional logistic regression models conditioning on age and sex, and adjusted for education because education was a confounder. Statistical analyses were performed using SAS 9.2 (SAS Institute, Inc, Cary, North Carolina).
We used Stata 11.0 (StataCorp LP, College Station, Texas) to estimate the attributable fractions (AFs) of VTE (excess fractions) due to family history of MI and to family history of both VTE and MI, with the 95% CIs adjusted for age, sex, and education 30 –32 among blacks and whites.
Results
The median age of case patients was 50.0 years (5th percentile, 25 years old; 95th percentile, 68 years old), and the median age of control patients was 50.5 years (5th percentile, 27 years old; 95th percentile, 68 years old). The distribution differences between the 2 ethnic groups and between males and females were not statistically significant (Table 1). While case patients with VTE were less educated than were control patients, a family history of MI, obesity, diabetes, hypertension, cancer, and plasma fibrinogen levels ≥ 3 g/L were risk factors for VTE in unadjusted analyses.
Baseline Characteristics of Adult Case and Control Patients From the Genetic Attributes and Thrombosis Epidemiology Study, Atlanta, Georgia, 1998 to 2005.a
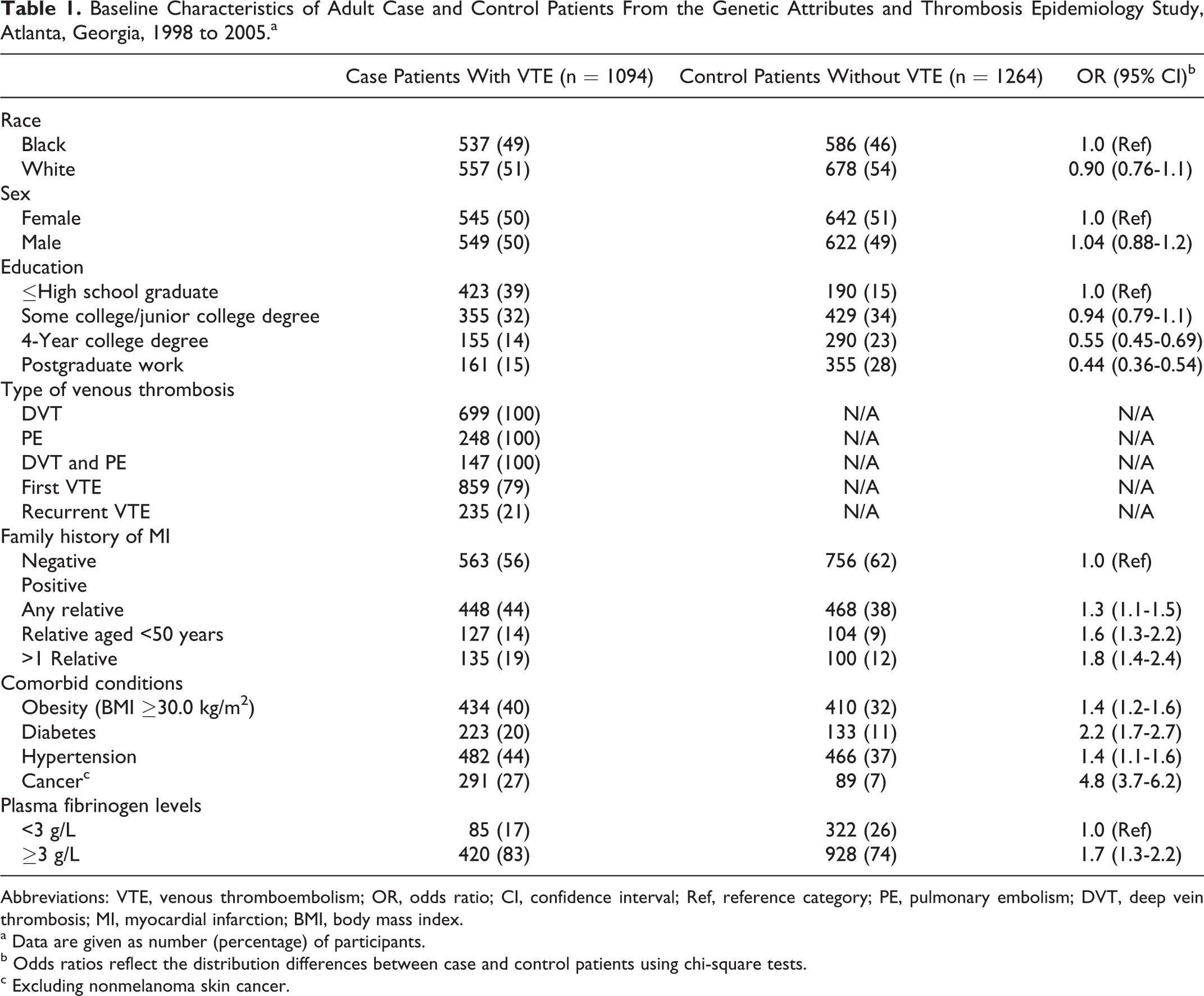
Abbreviations: VTE, venous thromboembolism; OR, odds ratio; CI, confidence interval; Ref, reference category; PE, pulmonary embolism; DVT, deep vein thrombosis; MI, myocardial infarction; BMI, body mass index.
a Data are given as number (percentage) of participants.
b Odds ratios reflect the distribution differences between case and control patients using chi-square tests.
c Excluding nonmelanoma skin cancer.
Influence of a Family History of MI on the Risk of VTE
VTE and a family history of MI
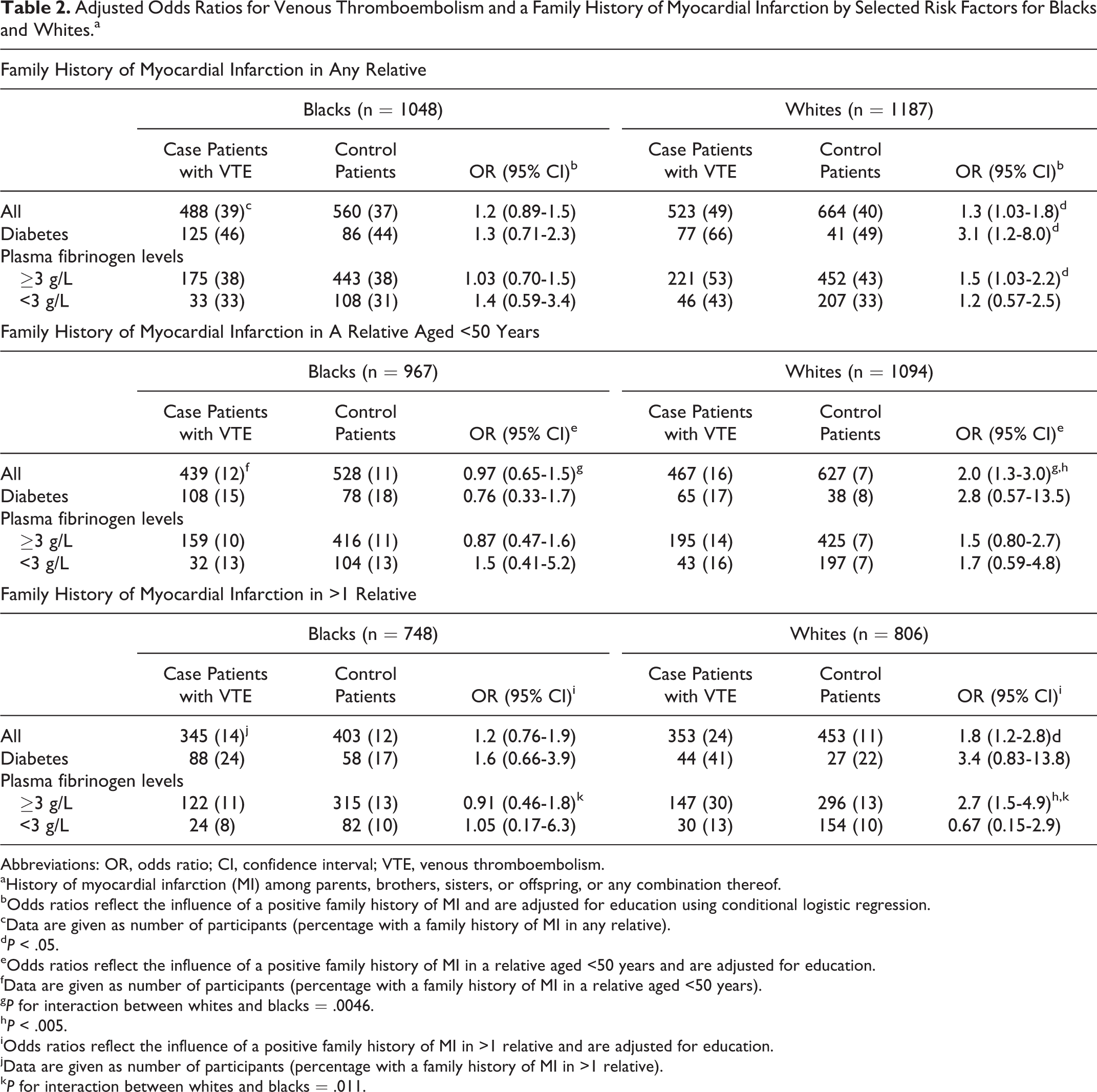
Results for the 3 family history of MI variables among white and black case patients with VTE and control patients are presented in Table 2. We found that the association between VTE and a history of MI in any first-degree relative was statistically significant among whites and the overall risk for VTE was 1.3-fold higher among whites with a family history of MI compared with those without a family history of MI. Among blacks, however, the overall association between VTE and a history of MI in any first-degree relative was not statistically significant. In addition, the association for a family history of MI in a relative before the age of 50 was 2-fold increased and statistically significant among whites, whereas among blacks, this association was close to the null value and not statistically significant (P for interaction between whites and blacks =.0046). Furthermore, the risk of VTE was almost 2-fold higher and statistically significant among whites who had multiple relatives affected by VTE compared with those without a family history of MI, whereas among blacks, this association was slightly increased but not statistically significant (P for interaction between whites and blacks lacked statistical significance).
Adjusted Odds Ratios for Venous Thromboembolism and a Family History of Myocardial Infarction by Selected Risk Factors for Blacks and Whites.a
Abbreviations: OR, odds ratio; CI, confidence interval; VTE, venous thromboembolism.
aHistory of myocardial infarction (MI) among parents, brothers, sisters, or offspring, or any combination thereof.
bOdds ratios reflect the influence of a positive family history of MI and are adjusted for education using conditional logistic regression.
cData are given as number of participants (percentage with a family history of MI in any relative).
d P < .05.
eOdds ratios reflect the influence of a positive family history of MI in a relative aged <50 years and are adjusted for education.
fData are given as number of participants (percentage with a family history of MI in a relative aged <50 years).
g P for interaction between whites and blacks = .0046.
h P < .005.
iOdds ratios reflect the influence of a positive family history of MI in >1 relative and are adjusted for education.
jData are given as number of participants (percentage with a family history of MI in >1 relative).
k P for interaction between whites and blacks = .011.
Diabetes and a family history of MI and VTE
When we assessed the association between VTE and a family history of MI by diabetes status, we found that this association was 3-fold higher and statistically significant among whites with diabetes but not among those without diabetes (OR = 1.2; 95% CI = 0.92-1.6); P for interaction between whites with diabetes versus whites without diabetes was statistically significant at .004 (data not shown). Among blacks, however, the association between VTE and a family history of MI was not statistically significant, either among those with diabetes (Table 2) or those without diabetes (OR = 1.1; 95% CI = 0.83-1.5; data not shown).
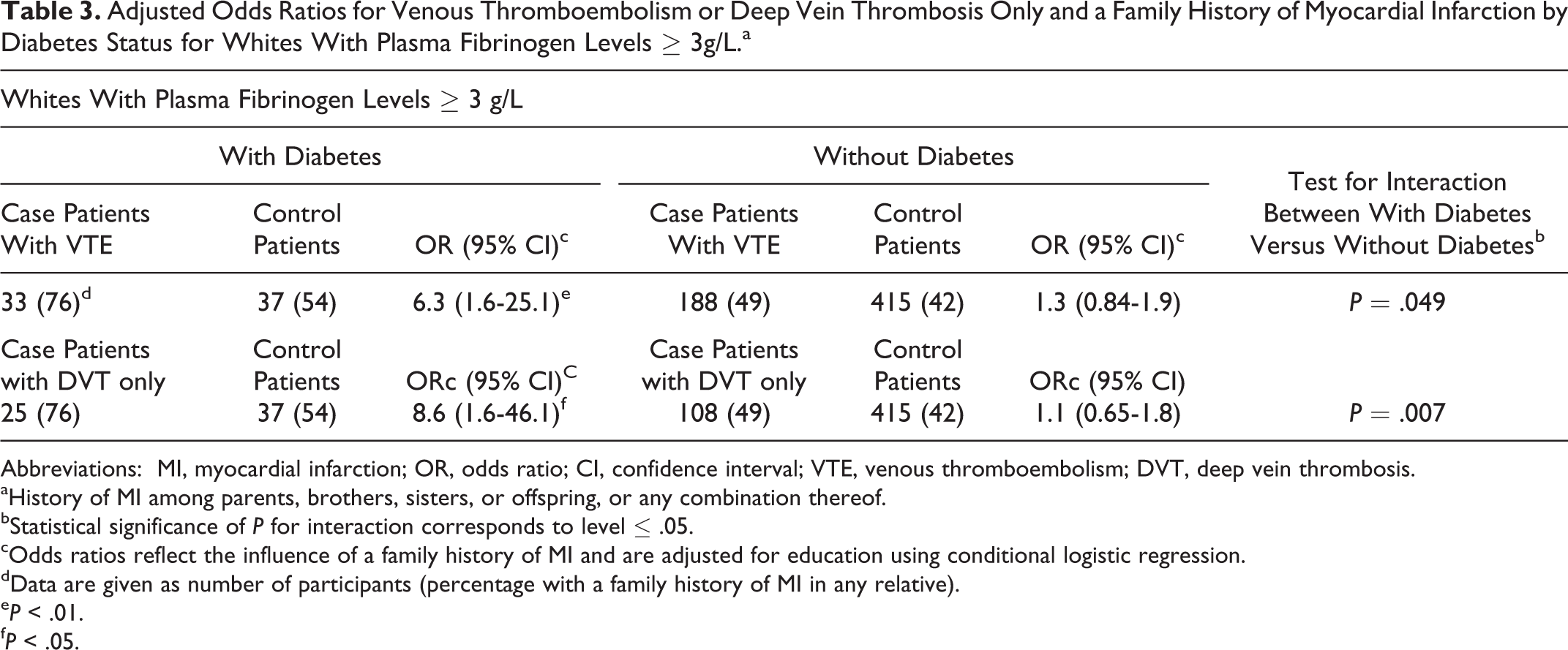
We further explored the effects of a family history of MI on the risk of VTE by diabetes status among whites with plasma fibrinogen levels ≥3g/L. As displayed in Table 3, among whites with plasma fibrinogen levels ≥3 g/L and diabetes, the risk of VTE was more than 6-fold stronger among those with a family history of MI compared with those without a family history of MI. Among whites with plasma fibrinogen levels ≥3 g/L and without diabetes, however, the risk of VTE was slightly increased but was not statistically significant among those with a family history of MI compared with those without a family history of MI; the P for interaction between whites with diabetes and those without diabetes was significant at .049.
Adjusted Odds Ratios for Venous Thromboembolism or Deep Vein Thrombosis Only and a Family History of Myocardial Infarction by Diabetes Status for Whites With Plasma Fibrinogen Levels ≥ 3g/L.a
Abbreviations: MI, myocardial infarction; OR, odds ratio; CI, confidence interval; VTE, venous thromboembolism; DVT, deep vein thrombosis.
aHistory of MI among parents, brothers, sisters, or offspring, or any combination thereof.
bStatistical significance of P for interaction corresponds to level ≤ .05.
cOdds ratios reflect the influence of a family history of MI and are adjusted for education using conditional logistic regression.
dData are given as number of participants (percentage with a family history of MI in any relative).
e P < .01.
f P < .05.
Other comorbid conditions and a family history of MI and VTE
The association between VTE and a history of MI in any first-degree relative was not statistically significant among whites with obesity (OR = 1.1; 95% CI = 0.65-1.8), hypertension (OR = 0.82; 95% CI = 0.52-1.3), or cancer (OR = 1.1; 95% CI = 0.57-2.3) nor among blacks with obesity (OR = 1.3; 95% CI = 0.87-1.9), hypertension (OR = 1.04; 95% CI = 0.72-1.5), or cancer (OR = 0.64; 95% CI = 0.27-1.5; data not shown).
The DVT Only or PE Only and a Family History of MI
When we focused the analysis on case patients with DVT only compared with control patients, we found that whites had a statistically significant positive association between DVT only and a history of MI involving several first-degree relatives (OR = 1.9; 95% CI = 1.1-3.2; data not shown).
When we assessed the association between DVT only and a family history of MI by diabetes status, we found that this association was almost 4-fold higher and statistically significant among whites with diabetes (OR = 3.8; 95% CI = 1.4-10.5) but was not increased among whites without diabetes (OR = 1.05; 95% CI = 0.74-1.5); P for interaction between whites with diabetes versus whites without diabetes was statistically significant at .0004 (data not shown). Among blacks, however, the association between DVT only and a family history of MI was not statistically significant either among those with diabetes (OR = 1.2; 95% CI = 0.64-2.4) or among those without diabetes (OR = 1.04; 95% CI = 0.73-1.5).
We further explored the effects of a family history of MI on the risk of DVT only by diabetes status among whites with plasma fibrinogen levels ≥3 g/L. As displayed in Table 3, among whites with plasma fibrinogen levels ≥3 g/L and diabetes, the risk of DVT only was almost 9-fold stronger among those with a family history of MI compared with those without a family history of MI. Among whites with plasma fibrinogen levels ≥3 g/L and without diabetes, however, the risk of VTE was slightly increased but was not statistically significant among those with a family history of MI compared with those without a family history of MI; the P for interaction between whites with diabetes and those without diabetes was significant at .007.
When we focused the analysis on case patients with PE only compared with control patients, we found that whites had a statistically significant positive association between PE only and a history of MI in a first-degree relative younger than 50 years of age (OR = 2.5; 95% CI = 1.3-4.6), whereas among blacks, this association was not statistically significant (OR = 0.97; 95% CI = 0.47-2.0); P for interaction between whites and blacks significant at .048 (data not shown).
Adjusted AFs for a Family History of Thrombosis
Results related to adjusted AFs for a family history of MI or VTE, or both, among whites and blacks are displayed in Table 4. The proportion of case patients with VTE that could be attributed to having a family history of MI (adjusted AF) was 4.5% (95% CI = 0.0%-13.7%) among blacks and 11.0% (95% CI = 0.0%-21.3%) among whites. Moreover, the joint effect of a family history of VTE and a family history of MI was 16.4% (95% CI = 6.4%-25.3%) among blacks and 22.0% (95% CI = 11.0%-31.7%) among whites.
Adjusted Attributable Fractions for Family History of Myocardial Infarction or Venous Thromboembolism, or Both, Among Whites and Blacks.
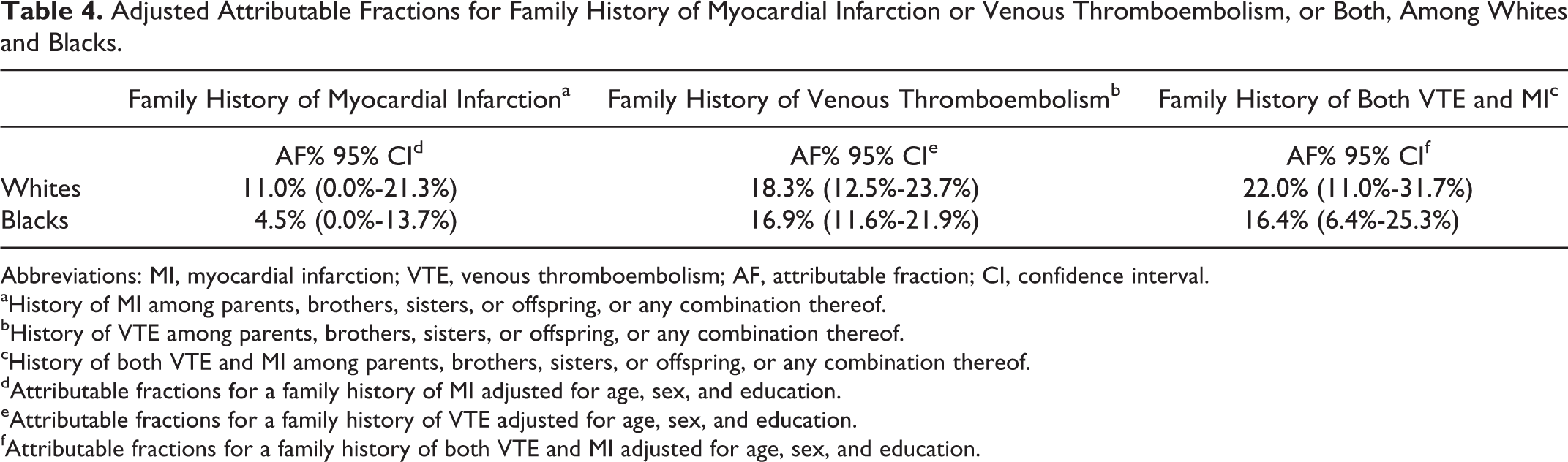
Abbreviations: MI, myocardial infarction; VTE, venous thromboembolism; AF, attributable fraction; CI, confidence interval.
aHistory of MI among parents, brothers, sisters, or offspring, or any combination thereof.
bHistory of VTE among parents, brothers, sisters, or offspring, or any combination thereof.
cHistory of both VTE and MI among parents, brothers, sisters, or offspring, or any combination thereof.
dAttributable fractions for a family history of MI adjusted for age, sex, and education.
eAttributable fractions for a family history of VTE adjusted for age, sex, and education.
fAttributable fractions for a family history of both VTE and MI adjusted for age, sex, and education.
Discussion
Overall results from our case–control study provided evidence that a family history of MI was a risk factor for DVT or PE, or both, among certain subgroups. Specifically, a family history of MI was associated with VTE among whites but not among blacks. In addition, a family history of MI in a relative younger than 50 years was a stronger risk factor for VTE among whites than among blacks. A family history of MI was also associated with VTE among whites who had diabetes and plasma fibrinogen levels ≥3 g/L. When we assessed the risk of DVT only or PE only among whites, we found a difference in the pattern of a family history of MI between these 2 conditions compared with those without a family history of MI; the risk of DVT only was almost 4-fold increased among whites with diabetes and a history of MI in any relative, whereas for PE only, the risk was 2.5-fold increased among whites with a history of MI in a first-degree relative younger than 50 years. Obesity, hypertension, or cancer did not further increase the magnitude of the association between VTE and a family history of MI among whites or blacks.
Our case–control study confirmed findings reported previously by Braekken et al 22 and Quist-Paulsen et al 23 that a family history of MI in a first-degree relative was a risk factor for VTE among whites. Although both of those studies 22,23 and our study differed in study design (prospective vs retrospective, respectively), the order of magnitude of measures of association between VTE and a family history of MI among whites was very comparable between these studies. On the other hand, in a nationwide family study conducted in Sweden, Zöller et al linked data from the nationwide Swedish Cause of Death Register and hospital discharge records for the period 1964 to 2008 and those from the Swedish Muti-Generation Register. 24 They observed positive—although very weak—associations between VTE and a family history of MI among offspring whose parents had a history of MI, as well as between VTE and a history of MI among spouses of those with VTE. The risk of VTE, however, was not statistically significant among individuals who had siblings with a history of MI.
In our study, we found black–white differences in the association between VTE and a family history of MI, with a positive and statistically significant association among whites but not among blacks. These ethnic differences might be explained to some extent by genetic thrombophilia. For example, factor V Leiden and prothrombin gene mutation are much more common among whites than blacks and could account in part for the differences in VTE risk. Black–white differences might also be explained by a higher incidence of MI among whites than among blacks, as reported by Alderman et al 33 when describing results from a cohort study of 3382 male participants enrolled in a work-site hypertension control program. In addition, our study revealed that a family history of MI was a risk factor for DVT among whites with diabetes and plasma fibrinogen levels at ≥3 g/L but not among whites who did not have diabetes. This finding might reflect underlying pathophysiologic mechanisms associated with hyperglycemia, inflammation, and coagulation involved in the development of atherothrombotic disease and venous thrombosis. 4,15
From a public health perspective, we found that the adjusted AF for a family history of MI was 4.5% among blacks versus 11.0% among whites. These proportions can be interpreted as the proportion of all case patients with VTE among the study population who were excess case patients, that is, case patients with VTE who would not have had VTE had a family history of MI been absent. 34 As anticipated, the AFs for a family history of MI were smaller than the AFs for a family history of VTE in our study (16.9% among blacks vs 18.3% among whites). 21 We estimated that the AF for the joint effect of a family history of VTE and a family history of MI was 16.4% among blacks versus 22.0% among whites. So, for whites, adding information on family history of MI to a family history of VTE increased the AF by about 4%, whereas for blacks, the increase in the AF was negligible. Because a family history of VTE and MI were correlated, information on either one was predictive of VTE, but the association was stronger for a family history of VTE. Nonetheless, a family history of MI added marginally to the AF, at least among whites.
Strengths and limitations of the GATE study have been described previously. 21 For this report, the strength of our study was that it included a large sample of black study participants and, therefore, had the capability for the first time to report measures of association between VTE and a family history of MI among this ethnic group. Our study, however, had several limitations. First, because a family history of MI was self-reported and many participants might not have had recalled MI in their family members, misclassification of exposure might have occurred. Case patients with VTE might have been more likely than control patients to recall having relatives with MI. In this instance, we would have overestimated the familial risk of VTE. Second, our subset analysis focusing on the effect of plasma fibrinogen included only about half of case patients with VTE. The remaining half was excluded because plasma for the fibrinogen assays was not available for them. We believe, however, that case patients who returned for a blood draw did not differ from those who failed to return with respect to their family history status and plasma fibrinogen levels. Third, we were unable to include a family history of stroke in our analysis because information collected for a blood clot in the brain in family members had a 50% or higher rate of missing data (ie, at least half of participants did not know if their relatives’ stroke was caused by a blood clot). Therefore, we were not able to assess the risk of VTE among participants with a family history of arterial thrombosis reflected by both MI and ischemic stroke. Future research could include epidemiologic studies in which a family history of both MI and stroke will be collected in participants to better understand the relationship between arterial and venous thromboses. Finally, our analysis did not include a family history of diabetes because the GATE study was not designed to assess specifically the effects of a family history of diabetes on the risk of VTE and, therefore, a history of diabetes among first-degree relatives was not collected from the study participants during the interviews. Future research could integrate a family history of diabetes to assess the joint effect of a family history of arterial thrombosis and a family history of diabetes on the risk of VTE, especially among whites.
In summary, our study revealed a racial difference in the risk of VTE among participants with a family history of MI. Specifically, a family history of MI appeared to be a risk factor for VTE among whites and diabetes could have further increased the risk of VTE associated with a positive family history of MI, especially among whites with plasma fibrinogen levels ≥3 g/L. Our overall results among whites confirmed those from 2 Norwegian prospective studies, 22,23 providing further evidence of the link between arterial and venous thromboses. In addition, our study was the first report of the association between a family history of MI and the risk of VTE among blacks and suggested that a family history of MI was not a risk factor for VTE in this ethnic group. The white–black differences in the familial risk of VTE observed in our study might in part be due to genetic thrombophilia.
We concluded that a family history of MI might be an instrumental tool to detect at-risk family members of patients with VTE among certain populations when it is used in conjunction with a family history of VTE 21 and to decrease VTE occurrence among family members of case patients with VTE.
Footnotes
Authors’ Note
Presented in part at the 12th International Congress of Human Genetics, October 12, 2011, Montreal, Canada.
Acknowledgment
We thank members of the CDC Laboratory Research Branch and the Division of Blood Disorders for playing a role in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Centers for Disease Control and Prevention through the Associations of Schools of Public Health/CDC Cooperative Agreement mechanism.