
Abstract
Prompt, accurate diagnosis of deep vein thrombosis (DVT) is essential. A single, whole-leg ultrasound (whole-leg US) has been used to exclude DVT, but limited data exist for patients with high pretest probability (PTP) for DVT. This diagnostic management study tested the rate of venous thromboembolism (VTE) in patients with a PTP of “DVT likely” per the simplified Wells score when anticoagulation is withheld based on a single, negative whole-leg US. Consecutive patients presenting during coordinator shifts with a PTP of DVT likely were enrolled. Anticoagulation was withheld after a single, negative whole-leg US. The outcome was objectively confirmed VTE in 3 months. All 167 patients completed the follow-up. A single patient death was adjudicated as possibly caused by VTE, resulting in a VTE rate of 0.60% (95% confidence interval: 0.02%-3.29%). Whole-leg US should be further studied in diagnostic algorithms that utilize PTP scoring and
Introduction
Deep vein thrombosis (DVT) is a prevalent disease which, if left untreated, can be complicated by pulmonary embolism (PE) among other associated morbidities.1,2 Prompt and accurate diagnosis of DVT is essential.
Contrast venography, considered the reference standard for the diagnosis of DVT, is invasive and performed infrequently. Compression ultrasonography has become the most commonly used imaging method to evaluate suspected DVT of the leg.3–5 Ultrasound techniques can be divided into 2 groups according to the extent of the venous anatomy assessed. Proximal compression ultrasound (proximal US) reliably assesses the proximal deep veins of the leg from the proximal common femoral vein to the level of the popliteal vein. This technique is highly sensitive and specific for symptomatic proximal DVT but cannot detect DVT in the calf veins–referred to as distal DVT.3,4,6–9 Because undetected distal DVT may extend proximally and increase the risk of PE if an initial proximal US is negative, a second compression ultrasound must be performed 5 to 7 days later.2,10–13 Repeat testing is inconvenient, patient compliance with recommended follow-up is suboptimal, and a large number of repeat tests must be performed to detect relatively few propagated thrombi. 14
Whole-leg compression ultrasonography (whole-leg US) examines the deep veins of the leg from the inguinal ligament to the level of the malleoli. This technique evaluates both the proximal deep veins as well as the deep veins of the calf, allowing a diagnostic conclusion in a single session.
Management studies have demonstrated that both techniques exclude suspected DVT with a high degree of accuracy based on very low rates of 90-day venous thromboembolism (VTE) when anticoagulation was withheld on the basis of negative testing.10,11,15–20 A pooled analysis of 7 management trials using whole-leg US, including 4731 patients suspected of leg DVT, showed a 3-month rate of subsequent VTE of 0.57% when anticoagulation was withheld on the basis of a single negative study. 5 Serial proximal US and single whole-leg US have also been shown to be equivalent for the diagnosis of DVT. 21 Recently published guidelines support the use of whole-leg US for diagnosis of DVT, but note limitations in available evidence for patients at moderate or high PTP. 22
Recently, clinical prediction guides (CPGs) have been developed to identify patients suspected of DVT in whom the diagnosis can be excluded without imaging. These CPGs combine an assessment of pretest probability (PTP) and a sensitive
The aim of the present study is to evaluate the rate of VTE, including death attributed to VTE, in patients with a PTP score rated as “DVT likely” on a formalized scoring system 13 when anticoagulation is withheld based on a single, negative whole-leg US. Participants were followed for 3 months after initial negative whole-leg US. The outcome was objectively confirmed symptomatic VTE.
Materials and Methods
Patients
We screened consecutive adults referred to a tertiary care hospital’s peripheral vascular laboratory suspected of first time DVT from November 2005 through August 2010, during weekdays from 8
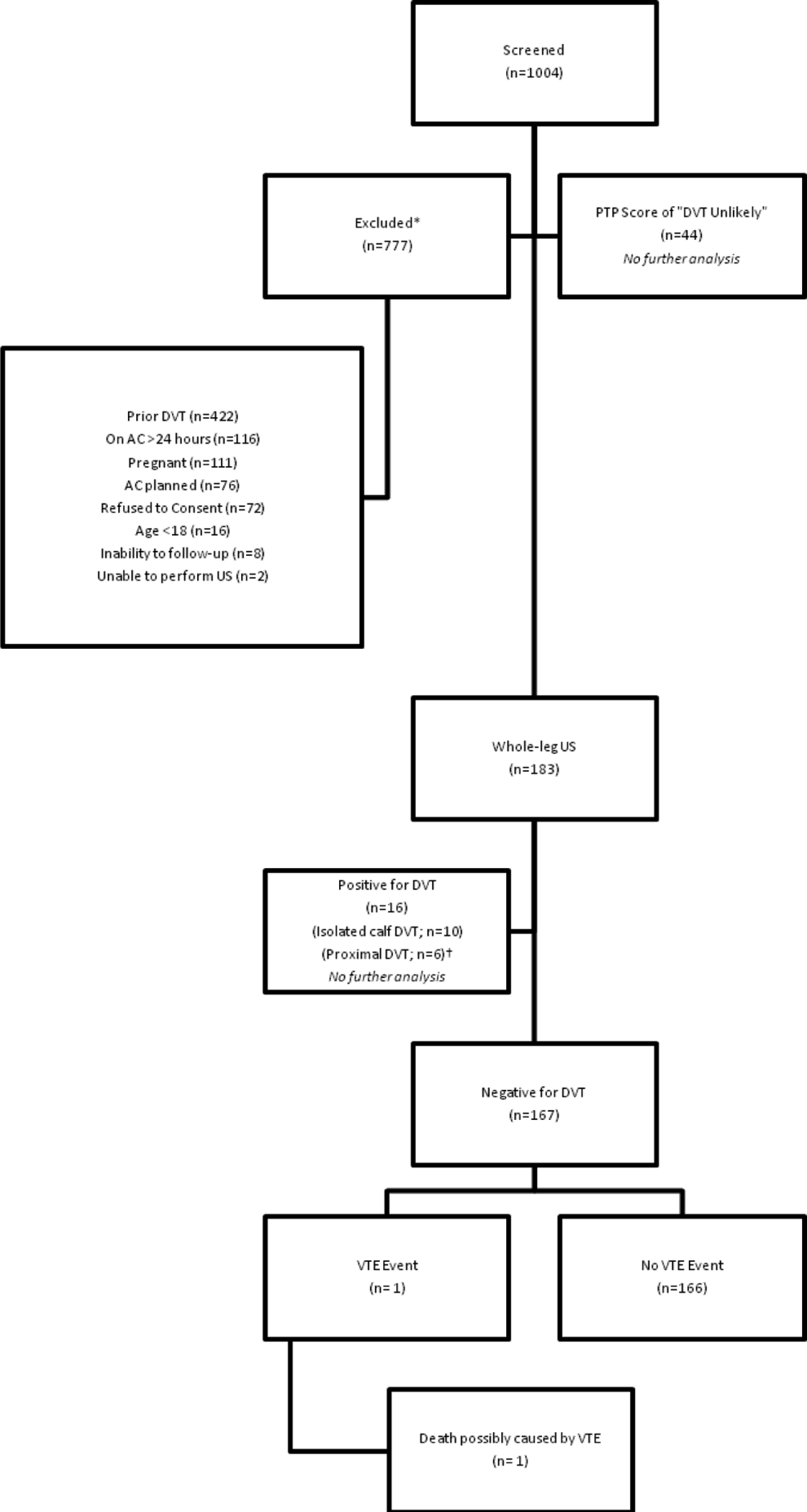
Consort diagram of study. *Participants could be excluded for more than one reason. †All participants with proximal DVT also had calf-vein DVT. DVT indicates deep vein thrombosis; AC, anticoagulation; US, ultrasound; VTE, venous thromboembolism.
Descriptive data and PTP of DVT, calculated using a validated scoring system,13,25 were collected for each patient. Forty-four (19.4%) participants had a PTP score of less than 2 points, categorized as “DVT Unlikely,” 13 and were excluded from further analysis. Characteristics of the patients screened and enrolled are presented in Table 1 and the study flow is presented in Figure 1.
Characteristics of Patients Undergoing Whole-Leg US
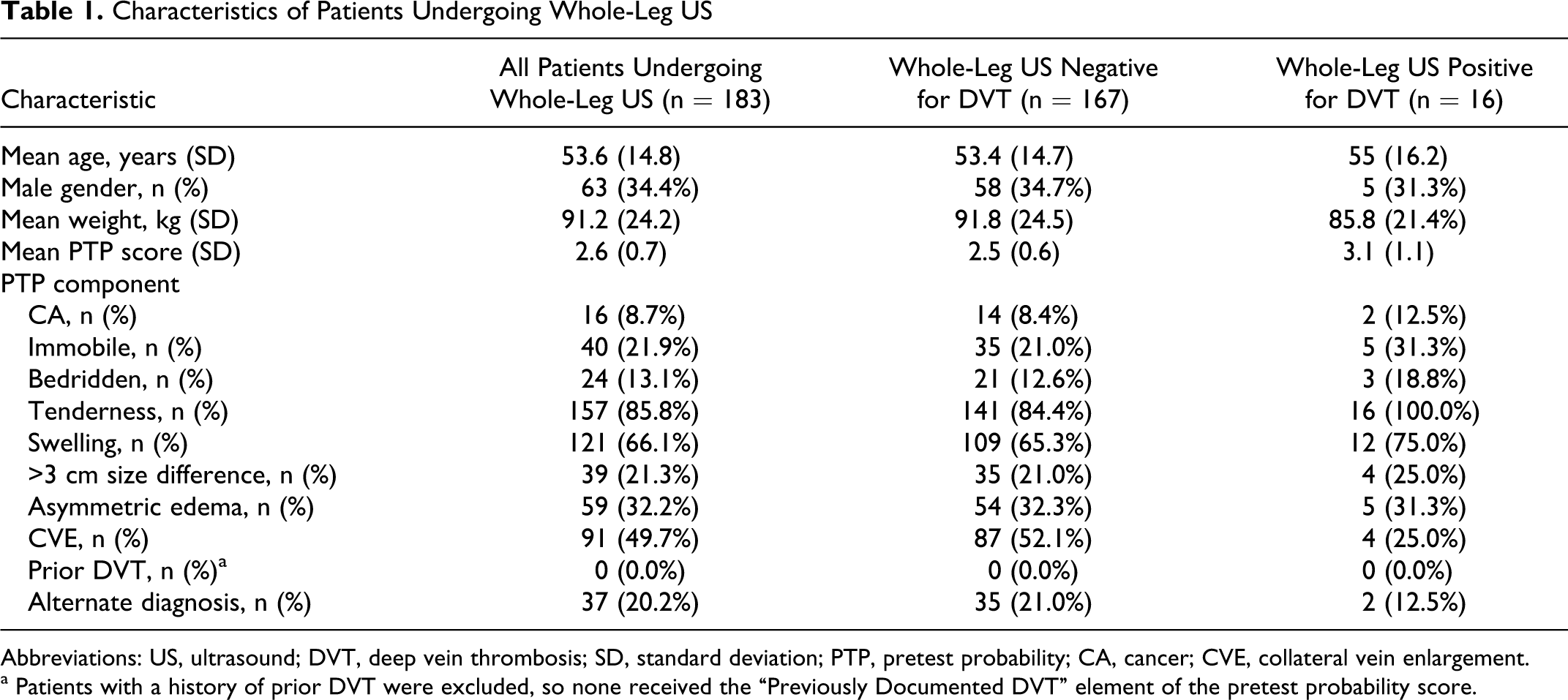
Abbreviations: US, ultrasound; DVT, deep vein thrombosis; SD, standard deviation; PTP, pretest probability; CA, cancer; CVE, collateral vein enlargement.
a Patients with a history of prior DVT were excluded, so none received the “Previously Documented DVT” element of the pretest probability score.
A total of 183 patients then underwent objective testing for DVT, with 1 whole-leg US of the symptomatic leg. The Intermountain Healthcare Urban Central Region Institutional Review Board approved the study, and all enrolled patients provided written informed consent.
Long-Term Follow-Up
All patients were instructed to return to the hospital immediately if they experienced symptoms or signs of VTE. All patients in the study cohort were interviewed at least 3 months after study enrollment and queried for specific symptoms of VTE, whether receiving anticoagulants, diagnostic testing for VTE, hospitalization, surgery, and general health. We also comprehensively reviewed each patient’s electronic medical record, which included all inpatient, outpatient, and diagnostic service records. Follow-up interview and electronic record review were successfully performed on all participants.
Objective Testing for DVT
Whole-leg US was performed immediately after enrollment and assessment of PTP. We used a modified version of the technique of Talbot, 26 which has been described in detail. 17 Registered vascular technologists performed all whole-leg US and certified vascular surgeons on the hospital staff interpreted the results. Vascular technologists and interpreting physicians were unaware of the enrollment clinicians' assessment and the PTP score. A high-resolution, electronically focused linear array transducer with a 3.5- to 10-MHz variable frequency probe (model 5000 scanner, ATL Corp, Bothell, Washington) was used for all studies.
Whole-leg US was performed from the level of the most proximally identified deep vein, distal to the level of the malleoli. Compressibility was assessed at 2-cm intervals in the transverse plane. Interpreting physicians were required by protocol to characterize the study results as negative (DVT absent) if all imaged venous segments were fully compressible or as abnormal (DVT present) if a noncompressible segment was identified. Thus, the sole criterion for the diagnosis of DVT was noncompressibility of the vein. Doppler modes were used for supplemental information and to assist in identifying venous anatomy (eg, to distinguish deep veins from nearby arteries).
Anticoagulation was withheld from the 167 (91.2%) patients whose initial results of whole-leg US were negative, regardless of symptoms or clinical signs. Sixteen (8.7%) patients were found to have DVT on initial whole-leg US; DVT was isolated to the calf veins in 10 patients and proximal DVT was found in 6 patients. These were excluded from further analysis.
Outcomes
The primary outcome measure was VTE (including symptomatic DVT or symptomatic PE) verified by objective testing or by death attributed to VTE. The minimum follow-up period of 3 months was chosen on the basis of previous studies.10,27–29 Patients in whom DVT was suspected because of progressive symptoms were evaluated with repeated ultrasonography and continued long-term follow-up if negative. Those in whom PE was suspected were evaluated with computed tomography pulmonary angiography. 30 A priori, we determined that both the adjudication categories of “death caused by VTE” and “death possibly caused by VTE” would be counted as VTE events for the purposes of analysis.
Statistical Analysis
Descriptive statistics were calculated overall both for the negative and positive cohorts. Continuous variables were summarized using means and standard deviations and percentages and counts were provided for dichotomous variables. For death caused by VTE and death possibly caused by VTE, 95% confidence intervals were calculated using a binomial test. All analyses were conducted using R version 2.12.2. 31
Role of the Funding Source
This study was funded by the Intermountain Research and Medical Foundation, Murray, Utah. The foundation is a nonprofit entity with no financial interest in ultrasound devices and had no role in the design or reporting of this study.
Results
All 167 patients with clinically suspected DVT, a PTP score categorized as DVT likely (≥2), and with initially negative whole-leg US completed the 3-month follow-up. Both interview and record review were successfully achieved in all participants (no patient was lost to follow-up). No patients in the cohort received anticoagulants during the 3-month follow-up.
Over the course of follow-up, 1 patient died and 14 patients underwent 18 studies for suspected VTE. The death was adjudicated as possibly caused by VTE. This yielded an overall 3-month rate of VTE of 1 of 167 (0.60%; 95% confidence interval: 0.02%-3.29%), following a single, negative whole-leg US. Apart from the event mentioned above, all diagnostic studies were adjudicated as negative for VTE (Table 2 ).
Characteristics and Diagnostic Results of Suspected VTE and Deaths During Follow-Upa
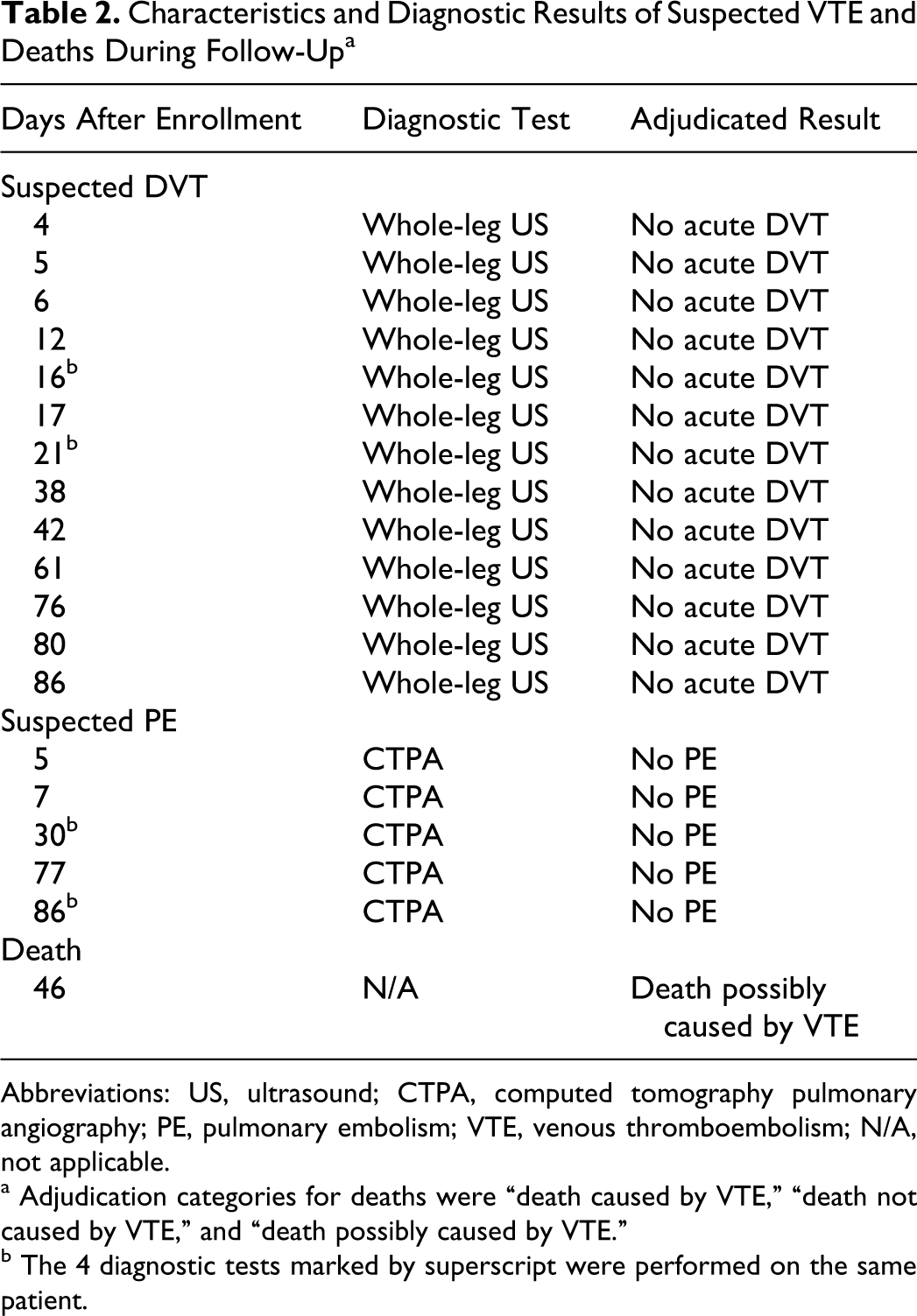
Abbreviations: US, ultrasound; CTPA, computed tomography pulmonary angiography; PE, pulmonary embolism; VTE, venous thromboembolism; N/A, not applicable.
a Adjudication categories for deaths were “death caused by VTE,” “death not caused by VTE,” and “death possibly caused by VTE.”
b The 4 diagnostic tests marked by superscript were performed on the same patient.
Discussion
We observed a low rate of symptomatic VTE when anticoagulation was withheld from patients with a PTP score of DVT likely on the basis of a single, negative whole-leg US. Limited prior study has been performed evaluating whole-leg US in this select patient group. 5
Our observed rate of VTE is similar to that noted by Gibson et al
24
in a population of patients with a PTP score of DVT likely and/or a positive sensitive
Use of whole-leg US in this group improves efficiency and may lower cost when compared with serial proximal US. Whole-leg US provides a diagnostic conclusion in a single setting, whereas a negative proximal US must be followed by another proximal US in 5 to 7 days.10,11 In our facility, both whole-leg US and proximal US carry a combined study and professional interpretation charge of $576 per leg (US dollars, based on 2011 facility pricing). Had our study population undergone serial proximal US, 177 patients would have required a second proximal US (167 cases negative for DVT and 10 cases in which initial proximal US would not have detected isolated calf vein thrombosis). Avoiding these repeat US studies represents a savings of approximately $100 000 in imaging fees.
Strengths of our study include 90-day follow-up for 100% of the study cohort and requisite objective diagnosis of VTE during follow-up to define outcome. Additionally, we minimized selection bias by enrolling consecutive patients who presented during coordinator shift and we did not attempt to retrospectively enroll patients who presented outside these hours. Verification bias 32 was avoided because all patients were contacted for clinical follow-up for VTE at 3 months. Previous studies have verified that repeated ultrasonography is a highly sensitive technique for detecting DVT missed on initial ultrasonography.10–12,33 This makes the potential incorporation bias 34 introduced by repetition of the diagnostic method less relevant. Experienced vascular surgery staff interpreted whole-leg US studies according to predefined criteria for negative and positive results. Interobserver variability was limited using a priori criteria for the presence and absence of DVT. 26 Only physicians certified to interpret vascular ultrasound read whole-leg US studies. A previous study found that interobserver agreement is high for this technique. 35
An independent adjudication committee unaware of the PTP score, original US result, and treatment status of the participants reviewed all cases of suspected VTE and deaths. Deaths were characterized as caused by VTE, not caused by VTE, or possibly caused by VTE. All the records and diagnostic test reports of patients in whom VTE was suspected during the follow-up period were reviewed by adjudicators with experience in VTE clinical trial research. Studies were interpreted as positive (DVT present) negative (DVT absent) or indeterminate. A simple majority resolved disputes. Adjudicators were not involved in the care of any patients in the study and were provided with de-identified hospital and physician records, death certificates, and imaging study reports.
Our study has several limitations. First, it should be noted that our study was small, resulting in a relatively wide confidence interval around our observed rate. A larger number of participants may have allowed us to report a more precise rate. We did however observe that the upper 95% confidence interval for recurrent VTE in our study exceeded 3%, a threshold that has often been accepted as clinically important. However, the single adjudicated VTE event in our study was classified as “possibly related to VTE.” No adjudicator classified the event as “caused by VTE.” The single death, which occurred in a 62 year-old female with cryptogenic cirrhosis, was adjudicated as death possibly caused by VTE. Limited information regarding the time and circumstances of death was available as the patient died at home; no autopsy or medical examiner review was performed. The immediate cause of death according to the death certificate was “cardiopulmonary arrest.” The patient had been receiving palliative paracentesis procedures for refractory ascites in the weeks prior to death. No diagnostic studies for suspected VTE were performed in this patient after her enrollment whole-leg US. Analyzing the VTE rate without this event would yield a result of 0 of 167 (0.00%; 95% confidence interval 0.00% to 2.18%). Notably, a venography-based strategy, which did not classify participants based on PTP, has reported a 90-day VTE rate with an upper limit to the confidence interval of 4.0%. 36
Initial whole-leg US showed DVT in only 16 (8.7%) of 183 patients. This rate is lower than that reported in other studies. 5 We chose to exclude patients with a prior history of DVT in order to avoid mis-ascertainment of the study outcome, which would be expected to reduce the rate of DVT on initial ultrasound. However, even studies which excluded patients with prior DVT reported higher rates than we observed. 13 It is possible that our population differs or that clinicians who refer patients to our vascular laboratory have a different threshold of diagnostic suspicion. Our results, therefore, should not be applied to patients with a history of prior DVT. Likewise, our results do not apply to pregnant patients, who were also excluded.
Of 1004 patients screened, only 227 were enrolled in the study, a higher rate of exclusion than in similar studies.17,24 Prior DVT and pregnancy accounted for over two thirds of exclusions; however, 72 persons approached for enrollment refused consent. Had these patients consented, it is possible that the observed rate of VTE would have differed, although there is no reason to expect that those who refused consent would be more or less likely to experience VTE during follow-up. Additionally, patients receiving more than 24 hours of therapeutic anticoagulation, or those for whom anticoagulation was planned for another purpose, constituted a quarter of excluded cases. While these criteria are common exclusions in management studies of suspected DVT,10,17,21 inclusion of such patients may have changed results.
Enrollment periods were defined as weekday business hours, during coordinator availability, rather than 24 hours a day; resources did not allow us to pursue around-the-clock screening. We did consecutively screen patients during these times and made no attempt to enroll patients retrospectively who reported outside these hours. Nonetheless, we cannot exclude the possibility that patients presenting during nights, weekends, holidays, and periods of coordinator unavailability have different characteristics. Therefore, had we been able to enroll these patients, our results may have been different.
During the course of the study, only 2 clinicians performed the PTP assessment, which could limit generalizability. Interobserver reliability has been shown to be high with the Wells 3-level PTP system, although the modified 2-level Wells PTP system has not been studied in this manner. 37 Our study was executed in a single health care system, with substantial expertise in whole-leg US. However, studies of whole-leg US have been reported across more than 200 centers,15–21 suggesting that the technique is generalizable.
The use of whole-leg US lead to the diagnosis of isolated calf vein DVT (ICDVT) in 10 cases. The best treatment of ICDVT remains controversial. The ICDVT carries a risk of complications, including propagation, PE, and the postthrombotic syndrome. Studies using ultrasound surveillance suggest than one quarter to one third of cases of ICDVT will propagate to the proximal deep veins; however, many such cases are asymptomatic. 38 A prospective 3-year study done among patients with first episode DVT evaluated the consequences of ICDVT when anticoagulation is withheld. Outcomes were significantly different at 3-month follow-up between patients with and without calf DVT. Isolated calf DVTs were diagnosed in 15.3% of outpatients, with a rate of symptomatic extension into proximal veins of 3.1% and one PE.
Conclusions
There is a low rate of VTE when anticoagulation is withheld following a single, negative whole-leg US in patients with a PTP of DVT likely suspected of a first symptomatic DVT of the leg. Further studies are needed to assess the utility of whole-leg US and define its role in the evaluation of suspected lower extremity DVT in other patient populations. Our study excluded pregnant patients and those with prior DVT and results should not be generalized to these patient groups.
Footnotes
Acknowledgments
We wish to thank Drs Clive Kearon, Shannon Bates, and James Douketis who served as adjudicators for suspected VTE events and deaths.
Declaration of Conflicting Interests
The author declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Ms Aston and Dr Snow received salary support for conducting this research.