
Abstract
Heparin-induced thrombocytopenia (HIT) remains diagnostically challenging. Immunoassays including PF4/heparin enzyme-linked immunosorbent assay (ELISA) have high sensitivity but low specificity. Whether the heparin neutralization assay (HNA) improves the diagnostic accuracy of the PF4/heparin ELISA for HIT is uncertain. In this study, to assess its clinical utility and evaluate whether it improves the diagnostic accuracy for HIT, we implemented HNA in conjunction with PF4/heparin ELISA over a 1-year period. A total of 1194 patient samples were submitted to the laboratory for testing from December 2015 to November 2016. Heparin neutralization assay alone is a poor predictor for HIT, but it has high negative predictive value (NPV): Cases with %inhibition <70% are always negative for serotonin release assay. It improves the diagnostic positive predictive value (PPV) of ELISA without compromising sensitivity: ELISA optical density (OD) ≥1.4 alone has a sensitivity of 88% (14/16) and a PPV of 61% (14/23); with HNA %inhibition ≥70%, the sensitivity remains 88% (14/16) and PPV is 82% (14/17). 4Ts score correlates with ELISA OD and predicts HIT; the predictive accuracy of 4Ts score is further improved by HNA. Interestingly, HNA %inhibition of <70% correlates with low 4Ts scores. Based on its high NPV, HNA has the potential to facilitate more timely and accurate HIT diagnosis.
Keywords
Background
Heparin-induced thrombocytopenia (HIT) is a complication of heparin therapy caused by antibodies that bind to PF4–heparin complexes on the surface of platelets. 1,2 These antibodies recognize neoepitopes within the heparin–PF4 complex and activate platelets as well as monocytes, 2,3 resulting in the generation of thrombin and platelet–fibrin thrombi. 4,5 Heparin-induced thrombocytopenia affects a significant number of patients, 6 has a high incidence of clinically significant venous and arterial thrombosis, and is associated with high morbidity and mortality. 1,7 Given the widespread use of heparin and the frequency of thrombocytopenia in hospitalized patients receiving heparin, 8 HIT is a common diagnostic consideration in many hospitalized patients. Consequently, timely and accurate diagnosis is crucial. Delayed therapy for patients with HIT can result in a significant risk of thromboembolism, amputation, and death. 9 Alternatively, misdiagnosis exposes patients having thrombocytopenia without HIT to a significant risk of anticoagulation-associated bleeding. 9
Diagnosis of HIT relies upon a careful assessment of clinical findings and laboratory test results. 10 Although the 4Ts score clinical pretest probability model has improved the clinical assessment of patients, 11 laboratory testing is required in many cases to exclude or confirm the diagnosis. The heparin–PF4 ELISA and the serotonin release assay (SRA) are the most widely used assays for laboratory confirmation of HIT. The PF4–heparin ELISA has a rapid turnaround time, but it is hampered by limited specificity. In contrast, the SRA is more specific but it is only available in a few reference laboratories, so results often take several days to return. Therefore, strategies to improve the timeliness and certainty of diagnosis are of significant clinical interest. Heparin-dependent binding is a specific feature of HIT antibodies, which thus should be “neutralized” by a high concentration of heparin. There have been previous studies evaluating the clinical utility of the HNA for HIT diagnosis, 12 –15 but most of them lacked SRA data for comparison or 4Ts scores for clinical correlation. In this study, we implemented a heparin neutralization assay (HNA) in conjunction with the PF4/heparin ELISA and assessed its clinical utility and evaluated whether it improves the diagnostic accuracy for HIT.
Materials and Methods
This retrospective study was approved by the institutional review board at Johns Hopkins Medical Institution. Testing for antiheparin/PF4 immunoglobulin G (IgG) antibodies by ELISA (Immucor-GTI Diagnostics, Waukesha, Wisconsin) was performed per requests from patient’s physicians on 1194 consecutive specimens from December 2015 to November 2016. Clinical data including medical/surgical service, primary diagnosis, baseline platelet count, dates/types of heparin use, dates of platelet count nadir, and dates/types of thromboembolic events were collected when available.
4Ts Score Calculation
Clinical 4Ts score calculation was performed according to the established scoring system, 11 taking into account of typical clinical features of HIT: the magnitude of thrombocytopenia, the timing of the thrombocytopenia after heparin exposures, thrombotic events including skin lesions at heparin injection sites, and the presence or absence of other etiologies of thrombocytopenia. The resulting scores were separated into high (6-8 points), intermediate (4-5 points), and low (0-3 points) probability groups. 11 The clinical information used to calculate 4Ts scores was obtained by 4 physician investigators (GZ, JB, EG, and TSK). The reviewers were not blinded to the ELISA assay results, because all patients included for 4Ts scoring had positive ELISA results.
PF4/Heparin ELISA and HNA
Anti-PF4/heparin, IgG-specific ELISA (Immucor-GTI Diagnostics) was performed according to the manufacturer’s instructions. The HNA was performed by repeating the ELISA assay in the presence of 100 U/mL heparin. The formula for determining the %inhibition is as follows:

The negative control was provided by the manufacturer. Most patient samples that were positive for antiheparin/PF4 antibodies using a threshold OD measurement of 0.40 underwent a repeat ELISA, and an HNA test was performed simultaneously. The HNA %inhibition was calculated with the repeat ELISA OD. For the ELISA, the average OD value of the positive test results was used for data analysis.
Serotonin Release Assay
The SRA was performed at Quest. Patient serum was incubated with donor platelets in the presence of 14C serotonin and different concentrations of heparin. Antiheparin/PF4 antibody in the patient serum activates donor platelets, leading to the release of radiolabeled serotonin from the platelet granules. A positive SRA is expected to have >20% release of the 14C serotonin with low concentration of heparin. High concentration of heparin should reduce the serotonin release by at least 50% compared with low concentration of heparin.
Statistical Analysis
All statistical analysis was performed with the use of Prism 5 software (GraphPad Software, San Diego, California). Receiver–operating characteristic (ROC) curve analysis was used to assess the diagnostic accuracy of the tests, which is a measure of the ability of a test to distinguish between healthy and affected individuals. The Mann-Whitney U test was used to evaluate differences in the antiheparin/PF4 antibody levels, 4Ts scores, and %inhibition in HNA between SRA+ patients and SRA− patients. A P value of <.05 was considered statistically significant. Correlation analysis was performed using Spearman correlation.
Results
Overall HIT Testing Results
From December 2015 to November 2016, a total of 1194 specimens were submitted to The Johns Hopkins Hospital hematology laboratory for HIT testing. Of these samples, 129 resulted in a positive PF4–heparin ELISA (10%), representing 104 unique patients (some patients had the test ordered more than once within a week). Ninety-one unique samples underwent SRA testing, and 71 had an HNA done. Sixty-five specimens had both an HNA and an SRA performed, among which 33 (50%) patients had a low 4Ts score (0-3), 18 (27.7%) had an intermediate 4Ts score (4-5), and 12 (20%) had a high (6-8) probability 4Ts score. There was insufficient clinical information to calculate a 4Ts score in 2 patients. Table 1 summarizes the demographic information for the patients who had both SRA and HNA performed. The ELISA OD and 4Ts scores were significantly higher in the SRA+ group (Table 1), but the 2 groups were otherwise comparable.
Patient Characteristics.
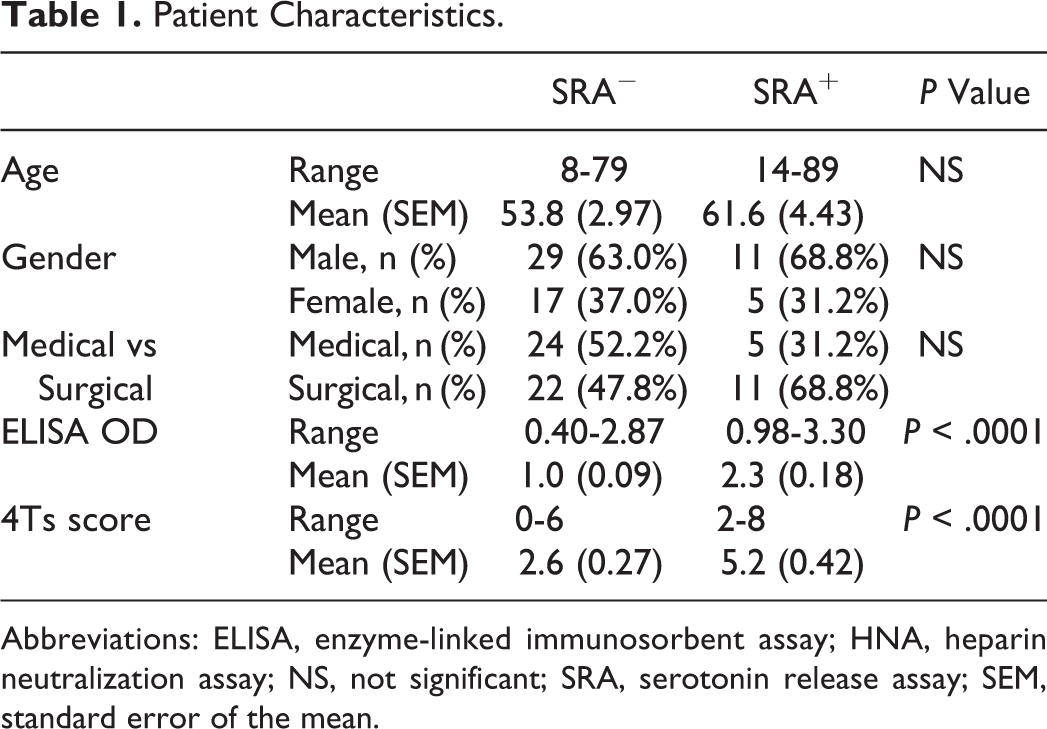
Abbreviations: ELISA, enzyme-linked immunosorbent assay; HNA, heparin neutralization assay; NS, not significant; SRA, serotonin release assay; SEM, standard error of the mean.
Heparin Neutralization Assay Alone Has Poor Diagnostic Accuracy for HIT
The ELISA OD has been shown to have a prediction value for HIT. 16 In our cohort, high ELISA OD correlates with SRA positivity, and the average ELISA OD is significantly higher in the SRA+ than SRA− group (2.2 vs 1.0; P < .001 by Mann-Whitney U test; Figure 1A). With SRA as the “gold standard,” using 0.4 as the recommended cutoff for OD shows low positive predictive value (PPV) of only 25% (16/64). The ROC analysis was performed for ELISA OD on the data set (Figure 1B). Area under the curve (AUC), a measure of “accuracy” reflecting the likelihood that a test will correctly distinguish between patients with and without disease, was 0.90 (P < .001, ROC analysis). In a setting such as HIT where both sensitivity and specificity of a diagnostic assay are important, the point on the ROC curve with maximum sum of sensitivity and specificity can be regarded as a threshold. 17 This point in the ROC curve corresponds to an ELISA OD of 1.49. Of note, all the SRA positive cases had an OD >0.9. With an OD of 0.9 as a cutoff, the sensitivity for HIT diagnosis is 100% with a PPV of 48% (16/33); with 1.4 as a cutoff, the sensitivity for HIT diagnosis is 88% (14/16) with a PPV of 64% (14/25). In contrast, the average %inhibition in the HNA shows no significant difference between SRA− and SRA+ groups (P = .16 by Mann-Whitney U test; Figure 2A). The SRA+ group had an average HNA inhibition of 98% (ranging from 71% to 107%). In comparison, the SRA− group shows a wider variability with an average HNA inhibition of 81% (ranging from −30% to 344%). It is noted that some specimens had HNA %inhibition of >100%, which is caused by ELISA ODs with heparin lower than the negative control and/or borderline positive ELISA. The ROC analysis was performed for HNA %inhibition on the data set (Figure 2B). The AUC was approximately 0.62 (P > .05, ROC analysis). With 70% as the cutoff, HNA %inhibition has a sensitivity of 100% and a PPV of only 36% (Figure 2B). There was no correlation between ELISA OD and %inhibition in HNA (P = .23 by Spearman correlation; Figure 3). The cases with ELISA OD ≥1.4 and HNA %inhibition ≥70% are shown in Figure 3.
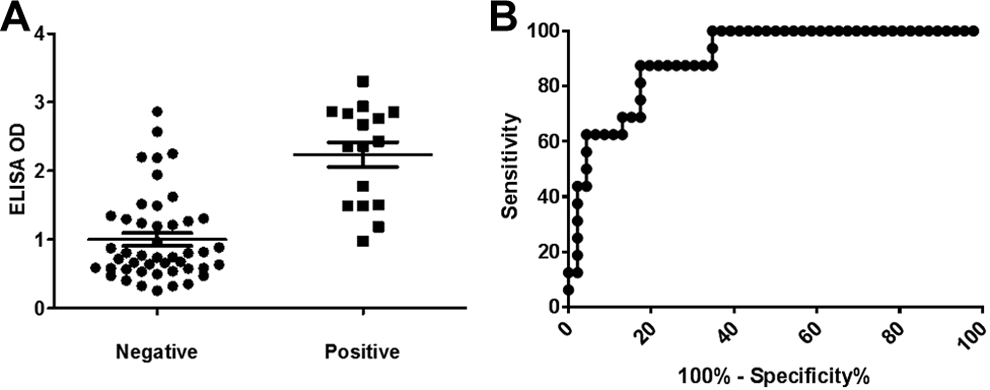
Heparin/PF4 enzyme-linked immunosorbent assay (ELISA) OD correlates with serotonin release assay (SRA) positivity. A, Dot plot of ELISA OD for SRA− and SRA+ patients shows SRA+ patients have significantly higher ELISA OD (P < .001). Mean ± standard error of the mean (SEM) was shown as horizontal lines. B, Receiver–operator characteristic (ROC) curve analysis for ELISA OD was performed, designating patients with positive SRA as “disease positive.” Area under the curve (AUC) was 0.90, P < .001.
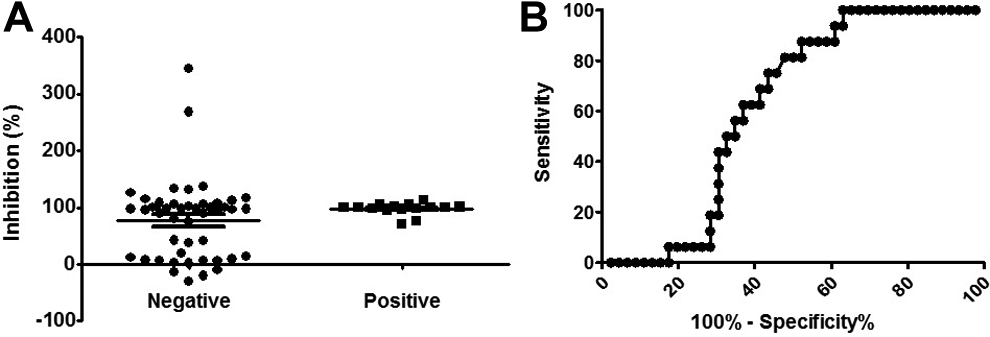
Heparin neutralization assay (HNA) result is a poor predictor for heparin-induced thrombocytopenia (HIT). A, Dot plot of %inhibition in HNA for SRA− and SRA+ patients shows no significant differences between the 2 groups (P > .05). Mean ± standard error of the mean (SEM) was shown as horizontal lines. (B) Receiver–operator characteristic (ROC) curve analysis for HNA %inhibition was performed, designating patients with positive SRA as “disease positive.” Area under the curve (AUC) was 0.62, P > .05.
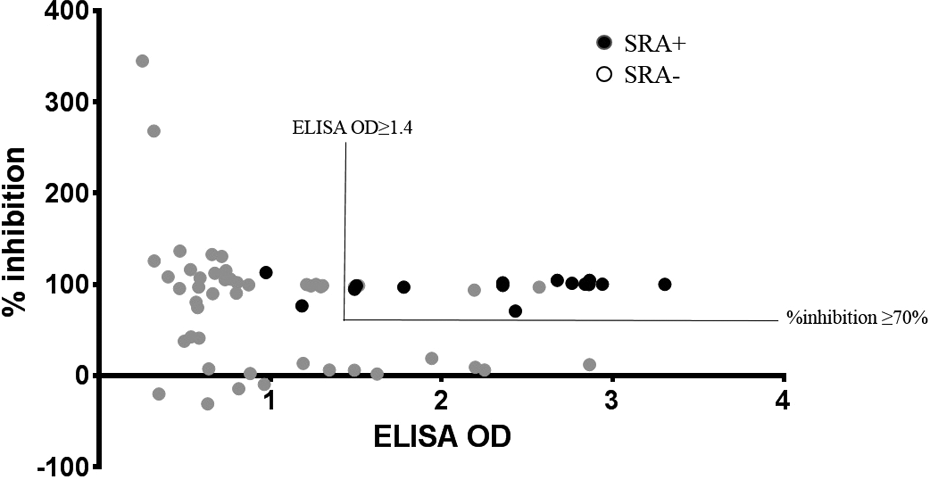
Enzyme-linked immunosorbent assay (ELISA) OD has no correlation with heparin neutralization assay (HNA) %inhibition. Dot plot shows there is no correlation between ELISA OD and HNA %inhibition (P > .05). Serotonin release assay (SRA)–positive cases are highlighted as black. The region with ELISA OD ≥1.4 and HNA %inhibition ≥70% is shown.
The HNA Improves the Diagnostic Accuracy of the PF4/Heparin ELISA
We then tested whether the HNA improves the diagnostic accuracy of the ELISA. Since the %inhibition in the HNA is more than 70% in all SRA+ cases, we include only cases with HNA %inhibition ≥70%, and an ROC analysis was performed on ELISA OD with the data set (Figure 4). The test accuracy was improved, as the AUC was 0.94 (P < .001, ROC analysis), compared to the AUC of 0.90 with ELISA OD alone. With ELISA OD ≥0.9 and HNA %inhibition ≥70%, the sensitivity of the test combination is 100% (16/16) with a PPV of 66% (16/24). With ELISA OD ≥1.4 and HNA %inhibition ≥70%, the sensitivity of the test combination is 88% (14/16) with a PPV of 82% (14/17). Three cases with OD ≥1.4 and HNA %inhibition ≥70% but negative SRA are listed in Table 2, which summarizes their clinical and laboratory characteristics. The first patient had a low clinical 4Ts score, and the other 2 lacked sufficient clinical information for 4Ts scoring.
Clinical and Serological Characteristics of Patients With Inconsistent SRA and ELISA/HNA Results.

Abbreviations: ELISA, enzyme-linked immunosorbent assay; F, female; IgG, immunoglobulin G; M, male; NA, not applicable; Neg, negative; SRA, serotonin release assay.
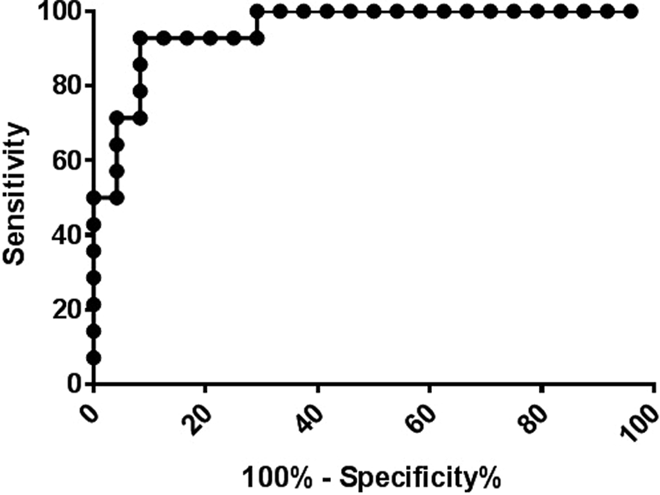
Heparin neutralization assay (HNA) significantly improves the diagnostic accuracy of enzyme-linked immunosorbent assay (ELISA). Receiver–operator characteristic (ROC) curve analysis for ELISA OD was performed for patients with HNA %inhibition ≥70%. Patients with positive SRA were designated as “disease positive.” Area under the curve (AUC) was 0.94, P < .001.
The HNA Improves the Predictive Accuracy of the 4Ts Score for HIT
We calculated the 4Ts scores for all 65 cases that had both SRA and HNA results. The ELISA OD values correlated with 4Ts scores (P = .017 by Spearman correlation; Figure 5A). The average ELISA OD was 0.98 in the low 4Ts score group, 1.55 in the intermediate group, and 1.84 in the high 4Ts score group. Although there was no correlation between the overall average %inhibition and 4Ts scores (P > .05 by Spearman correlation; Figure 5B), negative HNA results (%inhibition <70%) are associated with low 4Ts score group (P < .05 by χ2 test). The ROC analysis was performed to evaluate the ability of the 4Ts score to diagnose HIT (Figure 5C). The AUC was 0.83 (P < .0001, ROC analysis). The point in the ROC curve with the maximum sum of sensitivity and specificity corresponds to 3.5, where the sensitivity of the 4Ts score to diagnose HIT is 88% (14/16) with a PPV of 52% (14/27). To study whether the HNA improves the ability of 4Ts scores to predict HIT, ROC analysis was performed on 4Ts scores limited to specimens with %inhibition ≥70% (Figure 5D). The AUC was 0.86 (P < .0001, ROC analysis). In conjunction with the HNA, the PPV of the 4Ts score for HIT is increased to 61% (14/23) without compromising sensitivity.
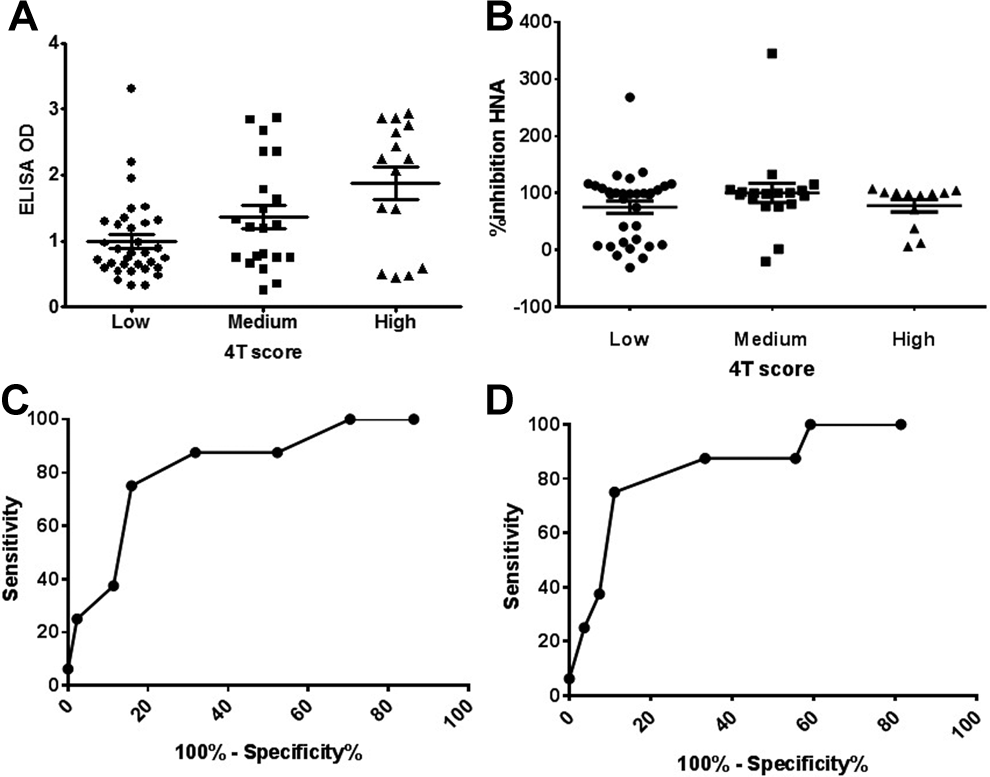
4Ts scores correlates with enzyme-linked immunosorbent assay (ELISA) OD value but not heparin neutralization assay (HNA) and predict HIT. A, Dot plot of ELISA OD in low, medium, and high 4Ts score groups. The ELISA OD correlates with 4Ts scores (P = .017 by Spearman correlation). Mean ± standard error of the mean (SEM) was shown as horizontal lines. B, Dot plot of %inhibition in HNA in low, medium, and high 4Ts score groups. Mean ± SEM was shown as horizontal lines. There is no correlation between HNA %inhibition and 4Ts scores (P > .05). C, Receiver–operator characteristic (ROC) curve analysis for 4Ts scores was performed, designating patients with positive serotonin release assay (SRA) as “disease positive.” Area under the curve (AUC) was 0.83, P < .001. D, The ROC curve analysis for 4Ts scores was performed for patients with HNA %inhibition ≥70%. Patients with positive SRA were designated as “disease positive.” Area under the curve (AUC) was 0.86, P < .001.
Discussion
Heparin-induced thrombocytopenia remains diagnostically challenging. 18,19 It can be missed due to the high frequency of thrombocytopenia in hospitalized patients and the numerous causes of thrombocytopenia, 20,21 and it is also frequently overdiagnosed due to the poor specificity of immunoassays. 22,23 In our cohort, the PPV of a positive heparin/PF4 ELISA (OD value ≥0.4) is only 25%. Overdiagnosis and underdiagnosis of HIT have important medical and economic consequences. 24 –27 Unfortunately, “gold standard” functional assays such as the SRA are not available in a timely manner in many medical centers. Therefore, an alternative assay that is rapidly and easily performed would be of significant utility. In this study, we showed that implementation of an HNA improved the diagnostic accuracy of the heparin/PF4 ELISA. Although HNA itself has poor diagnostic accuracy overall, it has high NPV: All cases with the HNA %inhibition <70% are negative for SRA. Using an ELISA OD cutoff of 1.4 and an HNA %inhibition cutoff of 70%, the ELISA/HNA combination has a sensitivity of 88% and a PPV of 82% with the SRA as the gold standard. The high NPV of the HNA could be used potentially to decrease the need for the SRA: For example, specimens with %inhibition <70% in the HNA should be considered HIT negative and don’t need SRA confirmation.
The heparin/PF4 ELISA is the most widely used test in the United States for HIT. It has been suggested that the specificity of the heparin/PF4 ELISA can be enhanced by increasing the OD threshold for a positive result. 28 In our cohort, we found that all SRA+ had an ELISA OD of ≥0.9, which is in agreement with another study suggesting that an ELISA OD value in the range of 0.45 to 0.8 rules out the diagnosis of clinical HIT. 29 However, the OD cutoff should be taken with caution, because antibody titers can be dynamic and change rapidly over a small time window after heparin treatment; thus, using an OD of 0.9 as a cutoff to rule out HIT needs validation in a larger study. Our results also support the correlation between SRA positivity and increased ELISA OD value; PPV increases with increasing ELISA OD. The PPV of OD ≥0.9 is 48% (16/33), while PPV of OD ≥2.6 is 88% (7/8; Figure 1B).
Heparin-dependent binding is a specific feature of HIT antibodies. Others have evaluated the clinical utility of the HNA, 12 –15 but their conclusions are conflicting. These studies on HNA either lack SRA data for comparison 13,14 or 4Ts scores for clinical correlation. 12 The current study is the first, to our knowledge, to include both clinical information (4Ts scores) and SRA results. Althaus et al 12 showed that heparin neutralization step increased the specificity for weak positive sera (OD ≤1.0) but decreased the sensitivity for strong positive sera (OD >1.0). In contrast, our study showed that sensitivity was not compromised by HNA even with strong positive sera. This discrepancy could potentially be explained using different immunoassays. Althaus et al used an in-house enzyme immunoassay (EIA) for anti-PF4/heparin IgG, while we used a commercial ELISA from Immucor-GTI. Different PF4/heparin ELISAs differ in several aspects: different sources of PF4, different polyanions, different classes of antibodies recognized, and varying thresholds. 30,31 It has been recognized that the diagnostic value may differ relevantly between the individual tests, 30,31 and as a result, the application of assays varies among laboratories. Given the variability in different ELISA assays, the %inhibition cutoff identified in our study may not be applicable to other assays, and assay condition such as the concentration of heparin in the HNA may need to be optimized for other ELISA assays. One previous study on the HNA that included both 4Ts scores and heparin-induced platelet aggregation (HIPA) assay data for correlation found that 2 HIPA-positive sera were not inhibited in the HNA, 15 which is in contrast to our study where all SRA-positive cases show HNA %inhibition of >70%. This discrepancy could be explained by the fact that platelet aggregation in HIPA has potential to be false positive. 32
The manufacturer of the commercial immunoassay in our study recommends that the %inhibition ≥50% in the presence of high-concentration heparin (100 U/mL) is considered confirmatory, while our study showed that 70% is a better cutoff with high NPV. Although neither ELISA nor HNA alone in isolation is a perfect predictor for HIT, these tests complement each other, as demonstrated by our study. The HNA is a much easier test to perform than the SRA and can be performed rapidly, suggesting that the HNA has the potential to facilitate a more timely and accurate HIT diagnosis. Based on our data, we propose to use the HNA, as a reflex test for a positive PF4/heparin ELISA test, to increase the specificity and PPV of the PF4/heparin ELISA test.
Clinical assessment tools such as the 4Ts score can identify patients with a low pretest probability and exclude HIT in many patients if conducted by experienced investigators. 33 However, the PPV of the 4Ts scores for HIT is low, 33 and 4Ts score assignment is subject to interobserver variability. 34 Lack of experience among observers has been shown to be a potential source of variation. 33,34 Moreover, some clinical information may not be available for adequate evaluation, 35 and the 4Ts score alone may be insufficient to exclude HIT in more complex patients. Our study shows that the 4Ts score correlate with ELISA OD and predicts HIT, and the predictive accuracy can be improved by HNA. Moreover, %inhibition of <70% in the HNA is associated with a low 4Ts score. It is noticed that a patient (no. 1 patient in Table 2) with a 4Ts score of 1, ELISA OD of 1.52, and HNA %inhibition of 98.6% had negative SRA, emphasizing that the clinical correlation is important in HIT diagnosis.
In conclusion, we show that the HNA, due to its high NPV, improves the diagnostic accuracy of PF4/heparin ELISA without compromising sensitivity. Our study has limitations. We had a limited sample size. Although there were more than 1100 samples submitted for HIT testing included in the study, only a limited number of samples with a positive ELISA had SRA and HNA data. The study is also limited to 1 immunoassay, which may reduce the generalizability of our results. Given the limitations, larger laboratory and clinical studies are warranted to further define the clinical utility of the HNA in guiding HIT management.
Footnotes
Authors’ Note
Paul Lin, a Clarksville high school student, contributed to the data analysis in HIT testing statistics.
Author Contributions
GZ, MBS, JJ, and TSK were involved in study design. JJ and DJ oversaw ELISA and HNA testing. GZ, TSK, JB, and EG assigned 4Ts scores. GZ analyzed the data. TSK and MBS provided advice on all aspects of the study. GZ wrote the manuscript, and all authors edited and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.