
Abstract
Background:
Endothelial dysfunction is the key process in the development of atherosclerosis. The aim of our study was to evaluate endothelial dysfunction measured by the noninvasive technique of Celermajer that plays a role in the pathogenesis of thrombangitis obliterans.
Methods:
A total of 36 patients with thrombangitiis obliterans ([TAO]; mean age 44.9 ± 1.3 years) were compared with 30 healthy individuals (mean age 36.1 ± 1.8 years). High frequency ultrasound was used to measure changes in response to reactive hyperemia (leading to flow-mediated endothelium-dependent dilatation) and in response to 0.4 mg sublingual nitroglycerin ([NTG]; leading to NTG-induced, endothelium-independent dilatation).
Results:
Patients with TAO showed a lower but statistically not significant flow-mediated dilatation and a statistically significant reduced NTG-induced vasodilatation than the control group.
Conclusion:
Our results suggest that both mechanisms play a role in patients with TAO, the endothelium-independent impaired vasodilatation even in a more significant way than the impaired endothelium-dependent vasodilatation.
Keywords
Introduction
Endothelial dysfunction is regarded as the key process in the development of atherosclerosis. It is an early event in experimental studies of atherogenesis preceding the formation of plaques.1,2 Since the development of a noninvasive measurement of endothelial dysfunction by Celermajer et al, the influence of all known vascular risk factors on endothelial function has been evaluated.2,3–9 Some studies also exist highlighting the influence of endothelial dysfunction in the process of nonatherosclerotic vascular disorders such as Raynaud phenomenon, immunologically based vasculitis, and thrombangitiis obliterans (TAO).10,11 The TAO is an arterial occlusive disease which is on one hand a different disease entity than atherosclerosis and on the other hand differs from any immunologically based vasculitis.12–15 It occurs mainly in the small- and medium-sized vessels of young adults with a high history of smoking. The pathogenesis of the disorder is still a matter of discussion and only the positive relationship with smoking is for sure. 15 Patients who stop smoking have a good chance of no further progression of the disease. As smoking has a negative influence on regular endothelial function, it can therefore most probably be concluded that endothelial function is deteriorated in patients with TAO. Some studies until now have addressed this matter and mostly shown markers for impaired endothelial function in TAO. The only drawback of these studies is their less number of patients.16–20
The aim of our study was to evaluate in a larger cohort of patients with TAO if endothelial dysfunction measured by the noninvasive technique of Celermajer 1 in fact plays a role in TAO. Dealing with this question, to our knowledge, this study is the largest cohort of patients with TAO.
Materials and Methods
Individuals
A total of 36 patients with TAO (mean age 44.9 ± 1.3years) were compared with 30 healthy individuals (mean age 36.1 ± 1.8 years). Patients were diagnosed for TAO when they met the following diagnostic criteria: history of smoking, onset of vascular disease before the age of 50, infrapopliteal arterial occlusive disease, either upper-limb involvement or phlebitis migrans, and absence of atherosclerotic risk factors other than smoking. 12 None of the patients or control individuals had any of the typical vascular risk factors, diabetes, or arterial hypertension. Patients with TAO and controls had started smoking around the age of 20. All our patients with TAO were in remission and showed no activity of their underlying disease as can be seen by baseline inflammatory parameters (Table 1 ). Smoking was not allowed on the day of the test. The individuals evaluated had a fasting period for at least 12 hours and no caffeine or tea intake for the same period of time.
Clinical Criteria for the Diagnosis of TAO
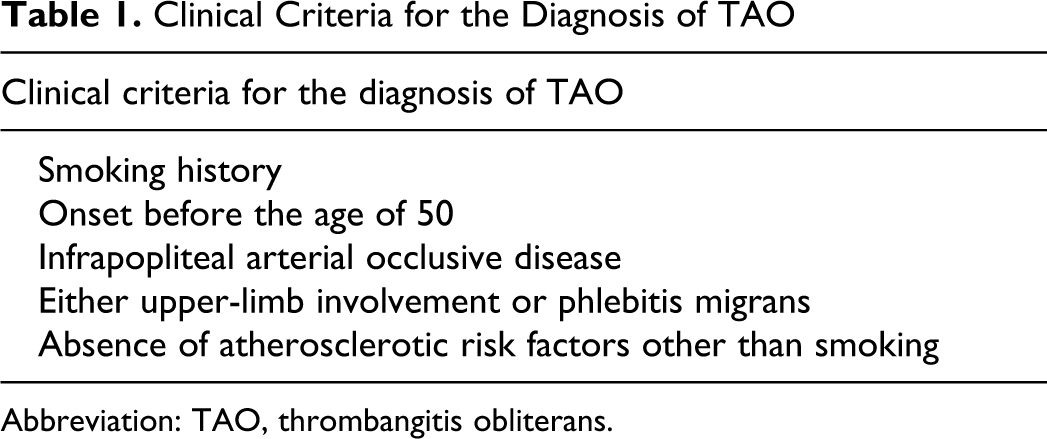
Abbreviation: TAO, thrombangitis obliterans.
Brachial Artery Vascular Reactivity
High frequency ultrasound (8 MHz transducer, Sequoia system; Acuson, California) was used to measure changes in response to reactive hyperemia (leading to endothelium-dependent flow-mediated dilation [FMD]) and in response to 0.4 mg sublingual nitroglycerin ([NTG]; leading to NTG-induced, endothelium-independent dilatation [NMD]) as described previously. 1 The right brachial artery was scanned in longitudinal sections 2 to 15 cm above the elbow, after at least 10 minutes of rest in the supine position. Hyperemia was induced by inflating a pneumatic cuff placed around the forearm to 230 mm Hg for 5 minutes, then deflating the cuff to 0 mm Hg. The artery was scanned before cuff inflation and 1 minute after deflation. After another 20-minute rest, a further control scan was recorded. A single dose of 0.4 mg of NTG was administered sublingually and the brachial artery diameter was recorded 4 minutes afterward. Four cardiac cycles were analyzed for each scan and the measurements averaged. All scans were recorded for later analysis. Diameter measurements were taken end diastole, coincident with R-wave on a continuously recorded electrocardiographic trace.
For the calculation of flow-mediated dilatation, the vessel diameter change of 1 minute after cuff deflation was divided by the average control diameter and expressed as percentage of the first control scan. Endothelium-independent dilatation was calculated as the vessel diameter change at 4 minutes after NTG had been given divided by the average control diameter and expressed as the percentage of the first control scan.
Statistical Analysis
All values are expressed as the mean ± standard error of the mean. Comparison of normally distributed variables was performed by Student test in order to test for differences among the 2 groups. For not normally distributed variables, the Mann-Whitney test was used for comparisons between 2 groups. P values less than .05 were considered statistically significant. All calculations were done with SPSS 10.0 for Windows.
Results
The characteristics of study individuals are summarized in Table 2 . There was no significant difference besides smoking between the 2 groups. Concerning smoking patients with TAO showed a significant higher percentage in smoking history than the control group (100% vs 20%).
Patient Characteristics
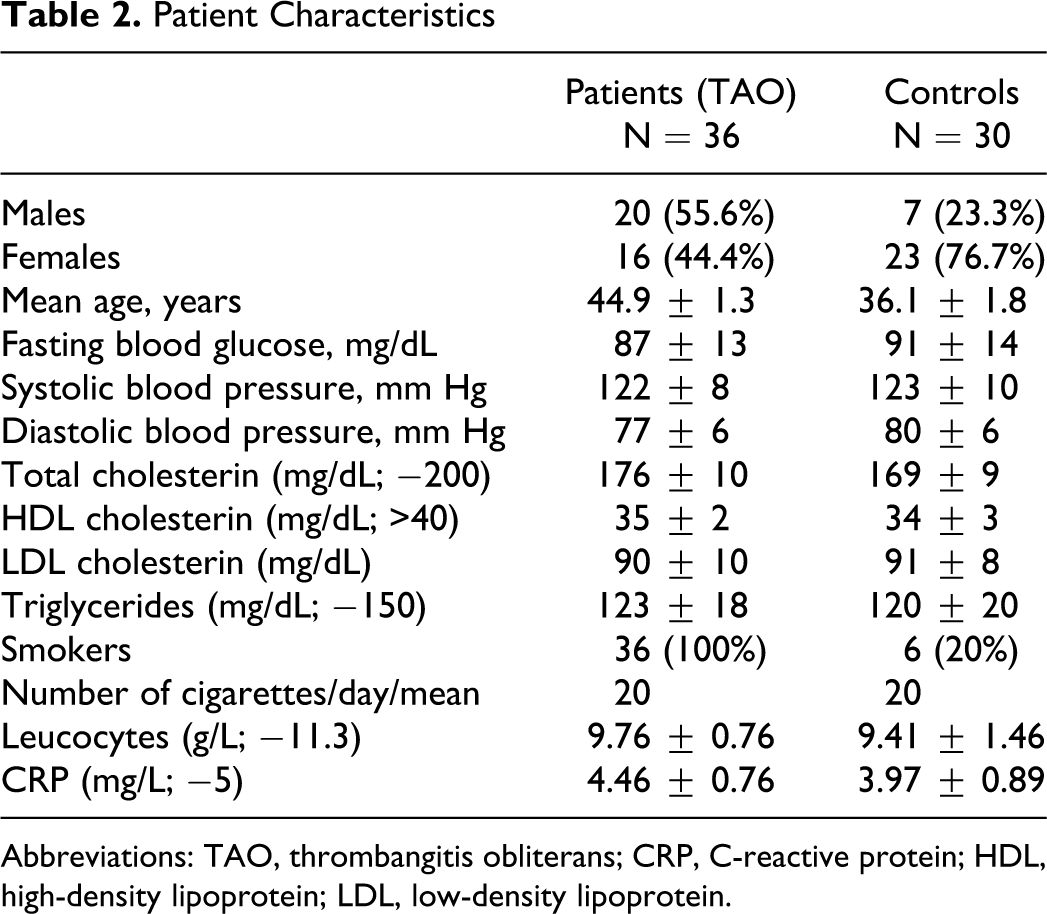
Abbreviations: TAO, thrombangitis obliterans; CRP, C-reactive protein; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Patients with TAO showed a lower FMD than the control group. But the difference did not reach statistical significance (Table 3 ). Nitroglycerin-induced dilatation did show significant difference between the 2 groups. Compared to the control group, NTG-induced (endothelium independent) vasodilatation was statistically significantly reduced in patients with TAO (Table 3).
Data FMD and NMD (%)a
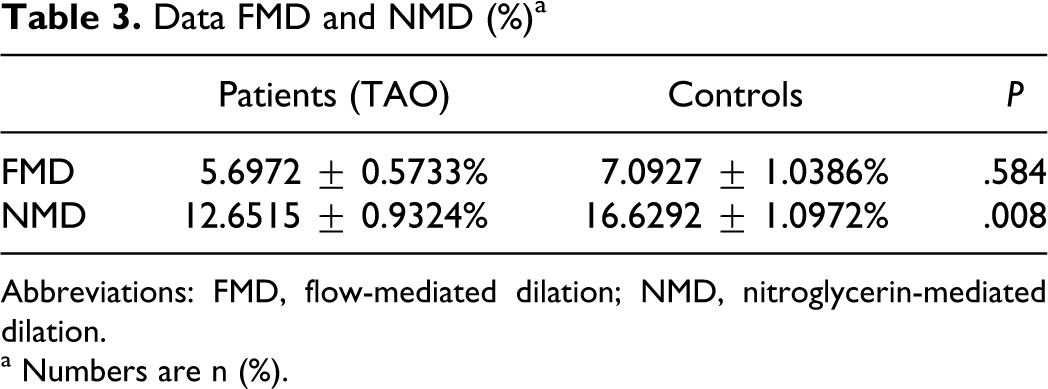
Abbreviations: FMD, flow-mediated dilation; NMD, nitroglycerin-mediated dilation.
a Numbers are n (%).
Discussion
In a disease like thromboangiitis obliterans, which is an arterial occlusive disease but differs in its entity from atherosclerosis and all other immunological vasculitides, the role of the endothelium in the pathogenesis of the disease is the more interesting, especially when regarding the positive and strong relationship of the disease to smoking.12–15
The results of our study show a positive relationship to impaired endothelium-dependent vasodilatation (FMD) in patients with TAO, although this difference was not statistically significant. The possible explanation for this phenomenon may be the high rate of non-dilatating individuals among the healthy control group. Our results resemble the results of 2 other studies,16,17 with the difference that in the above-mentioned studies, the authors found controversial results concerning NMD. In our collective data, NMD was statistically significantly lower in patients with TAO than in the control group. In arteries lined by healthy endothelium increased blood flow causes dilatation of the vessel, via release of endothelium-derived relaxation factor. This mechanism fails in endothelial dysfunction. In contrast, NTG causes vasodilatation by direct action of the smooth muscle, its effect is therefore independent of the endothelium. 1 In one article by Joras et al, an insignificant decrease of endothelium-independent vasodilatation was found. The authors therefore concluded a well-preserved muscle cell function in patients with TAO. 17
Our results suggest that both mechanisms seem to play a role in patients with TAO, the endothelium-independent impaired vasodilatation even in a more significant way than the impaired endothelium-dependent vasodilatation. This indicates also the probability of smooth muscle cell dysfunction of the arterial wall, owing to structural changes in vascular tissues and consequently more rigid vessels. The coincidence of endothelial dysfunction and impaired endothelial-independent vasorelaxation would also be a reasonable explanation why the disease is occurring at such a young age in a people’s collective with only one typical vascular risk factor, that is, smoking.
Besides our results represent data from a cohort of patients with TAO not in an active state of their disease, as much as such a state can be proved by baseline inflammatory parameters. Therefore, the data gained from both, endothelium-dependent vasodilatation and endothelium-independent vasodilatation, can be assumed to be data from a homogenous cohort. This is in contrast to the data published before.
When regarding the influence of typical vascular risk factors like hyperhomozysteinemia who are influencing endothelial function, for the development of TAO, these factors seem to play a role but not a high key role. Hyperhomozysteinemia is said to be related to TAO, but it seems only to be the environmentally acquired hyperhomozysteinemia not the genetically based defect of Methylentetrahydrofolat-Reduktase (MTHFR). 17 The genetic defect of nitric oxide synthetase also cannot be found in patients with TAO.
As all the factors influencing endothelial function are the same in people with atherosclerosis and TAO and not a specific one has been identified until now for TAO; and on the contrary, the distribution of these risk factors is even smaller in TAO, and it must be another fact which is crucial in the development of such a severe disorder in a young patients' group. The search should go for a factor which is influencing both endothelial function and endothelium-independent (smooth muscle cell dependent) vasorelaxation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.