
Abstract
Aim: We aimed to evaluate the frequency of catheter-related internal jugular vein (IJV) thrombosis, associated factors, and the anatomical variations of IJV in hemodialysis patients. Material and methods: Hemodialysis patients were evaluated with B-mode ultrasonography (USG). Participants in the prospective group were evaluated using USG prior to catheter insertion, 10 days after catheter insertion, at the time of catheter removal, and 15 days after removal. Results: The rate of thrombosis was increased correlated with the number of catheter insertions. These rates were 14%, 15%, and 47% in those undergoing catheter insertion once, twice, and three times, respectively (P < .05). The anatomical variations of IJV were 21% in the retrospective cases. No significant relationship was found between anatomical variations and thrombosis and between some biochemical parameters and thrombosis. Conclusion: Catheter-related IJV thrombosis is frequent in hemodialysis patients. Long catheter remaining time and repeated catheterization increase the thrombosis rate.
Introduction
Central venous catheters are frequently used in patients with end-stage renal failure, mainly for urgent hemodialysis treatment. Because the rates of stenosis and thrombosis are higher in the subclavian veins, catheterization of the internal jugular vein (IJV) is preferred. 1 Temporary hemodialysis catheters inserted into the IJV may lead to various early or late complications besides their advantages such as easy bedside insertion with USG.2 –4 One of these complications is venous thrombosis. This may lead to failure in arteriovenous fistulae, which are the most appropriate venous route for hemodialysis treatment, besides rendering subsequent catheterizations impossible. 5
In this study, we evaluated the frequency of catheter-related thrombosis, the associated factors, and anatomical variations of IJV in hemodialysis patients who had undergone insertion of the catheter.
Material and Methods
In this study, patients were conducted in the Hemodialysis Unit of the Medical Faculty of Yuzuncu Yıl University. Participants who had just undergone insertion of catheters into the IJV (n: 45, prospective group) and those who had undergone catheter insertion previously (n: 100, retrospective group) were evaluated in terms of thrombosis and anatomical variations using B-mode ultrasonography (USG; Fukudu Denshi UF–4100, Tokyo, Japan). The participants in the prospective group were evaluated using the USG prior to the catheter insertion, 10 days after the catheter insertion, at the time of catheter removal, and 15 days following removal.
Additionally, patients underwent Doppler USG (Philips HD 11, France) when there was presence of any of the followings: When a thrombus was visualized in the lumen of the vein. When the vein was not completely compressed. In the absence of spontaneous flow in the vein. When the flow did not demonstrate phases with respiration. In the presence of increased collaterals.
The age, gender, history of thrombosis, history, and number of previous catheter insertions, presence of diabetes mellitus (DM) of all cases were recorded. Furthermore, laboratory parameters such as calcium, phosphorus, parathormone, C-reactive protein (CRP), albumin, low-density lipoprotein (LDL), high-density lipoprotein (HDL), and triglyceride were studied (Table 1
). Parathormone was studied with the Immulite 2000 device using the chemiluminescence method. C-reactive protein was measured with the Dade Behring device using the nephelometric method. Other laboratory parameters were measured using the colorimetric method in the modular device.
Some Parameters That May be Related to Thrombosis in Prospective Group
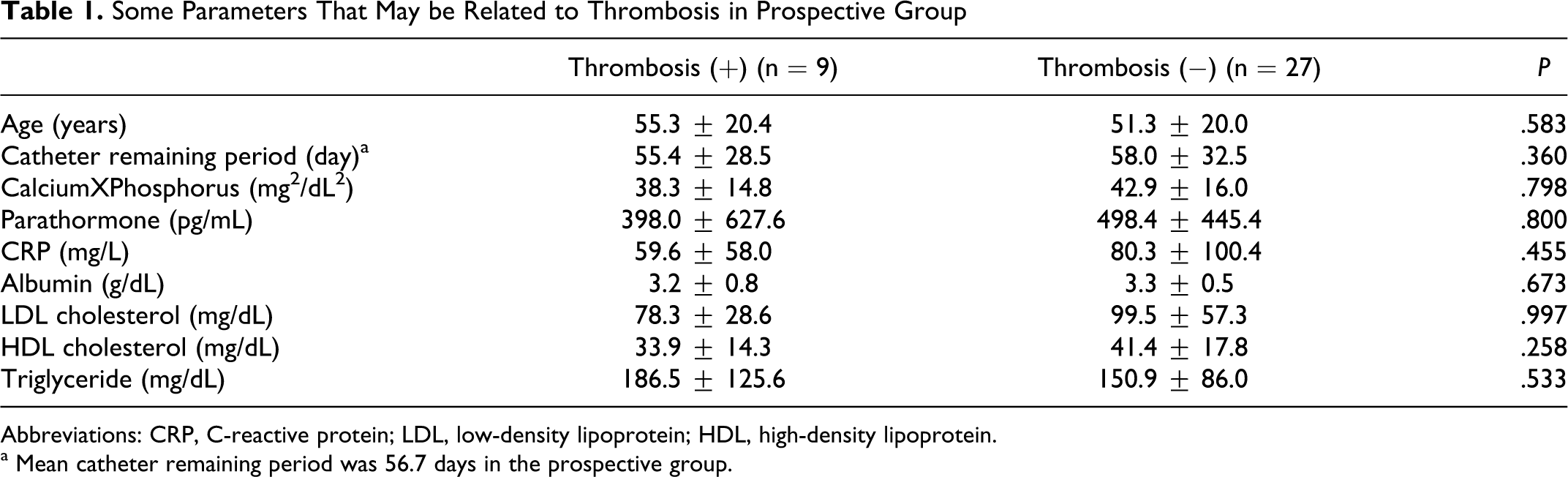
Abbreviations: CRP, C-reactive protein; LDL, low-density lipoprotein; HDL, high-density lipoprotein.
a Mean catheter remaining period was 56.7 days in the prospective group.
A total of 9 participants in the prospective group were excluded due to death (n = 4) and not turning up for follow-ups (n = 5). Of the remaining patients, 20 were females, 16 were males, and mean age was 52 ± 19.9 years. Of the patients in the retrospective group, 52 were females and 48 were males, with a mean age of 47 ± 17.2 years.
The data of the study were transferred to the SPSS 15.0 program and statistical analyses were performed. The results were recorded as mean and standard deviation. The 1-way analysis of variance (ANOVA) test was used in order to determine whether there was a significant difference between the groups in terms of the studied properties. Categorical variables were given as numbers and percentages. The chi-square (χ 2 ) test was used to determine the relationship between the 2 groups. In order to determine the frequency of thrombosis according to the number of catheter insertions, proportion comparisons were made using the Z test. A P value of <.05 was accepted as the level of statistical significance.
Results
While the rate of thrombosis in the retrospective group was 20%, it was 58.3% in the prospective group (P < .01, Z = 4.19). In the retrospective group, the duration of catheter remaining time was 125.2 ± 33.0 and 63.3 ± 4.4 days in the patients with or without thrombosis, respectively (P < .05). In prospective group, some parameters that may be related to thrombosis were evaluated such as age, catheter remaining period, calciumXPhosfors, parathormone, albumin, LDL cholesterol, HDL cholesterol, triglyceride, and CRP (Table 1).
While there was no thrombus in the prospective group before catheter insertion, the rate of thrombosis was 25% 10 days after catheter insertion and 58.3% at the time of catheter removal and 15 days after catheter removal (Table 2 ). In the retrospective group, of the cases in which thrombosis was detected, 15 (28.8%) were females and 5 (10.4%) were males (χ 2 = 5.29, P < .05). No relationship was found between thrombosis and gender in the prospective group.
Thrombosis Ratio and Catheter Duration Time in the Prospective Group
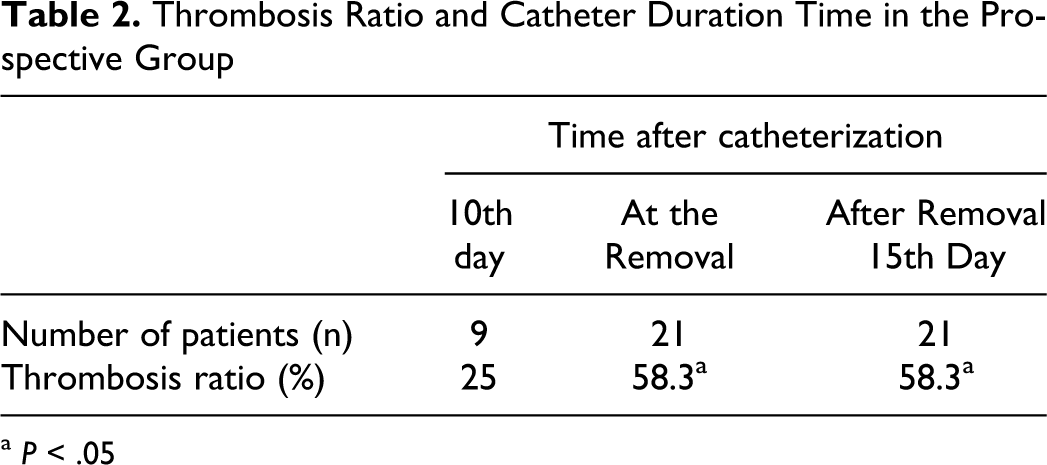
a P < .05
The rate of thrombosis increased as the number of catheter insertion increased in the retrospective group. These rates were 14%, 15%, and 47% in those who had undergone catheter insertion once, twice, three times, and more, respectively (P < .05; Table 3 ).
The Rate of Thrombosis and Number of Catheter Insertion in the Retrospective Group
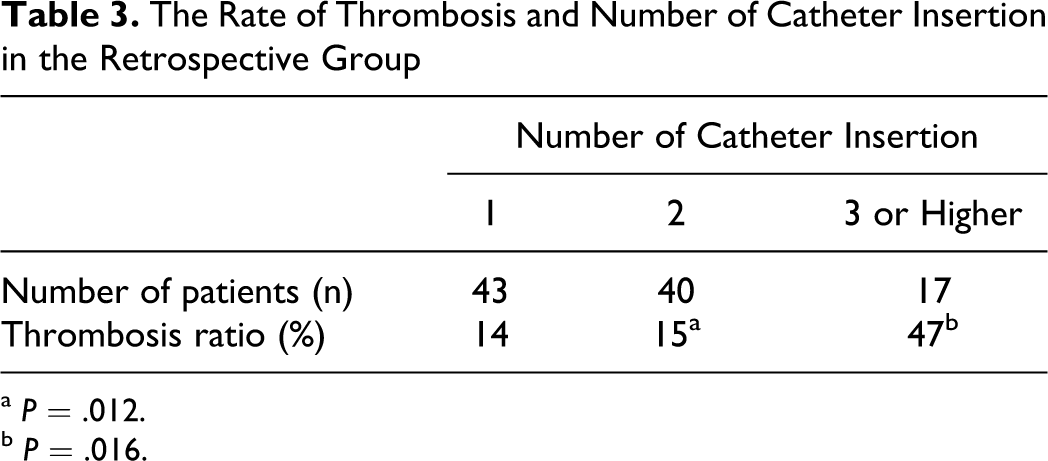
a P = .012.
b P = .016.
Diabetes mellitus was present in 14% of the retrospective cases. There was no difference between diabetic and not diabetic cases in terms of thrombosis rates (Table 4 ).
The Rate of Thrombosis and Diabetes Mellitus History in the Retrospective Groupa
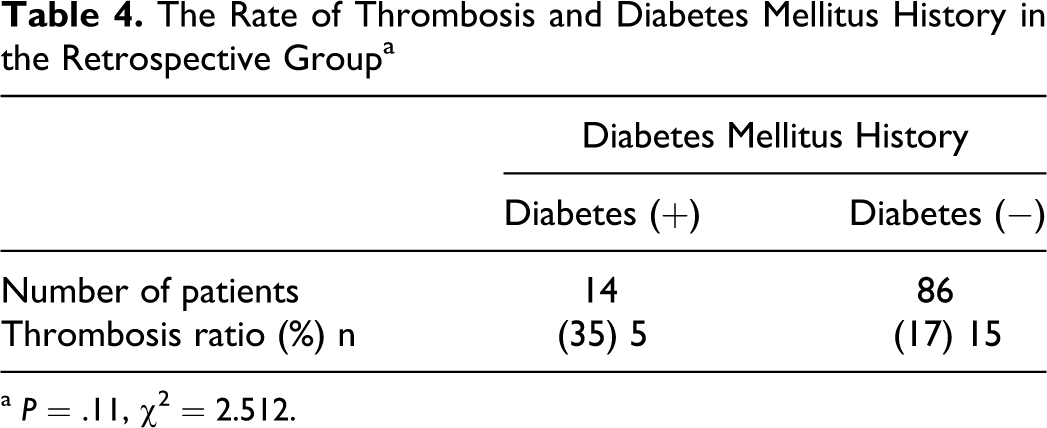
a P = .11, χ2 = 2.512.
Anatomical variations in IJV were detected at a rate of 21% in the retrospective cases. No significant relationship was found between anatomical variation and presence of thrombosis in the retrospective group (Table 5 ).
The Rate of Thrombosis and Anatomical Variations of IJV in the Retrospective Groupa
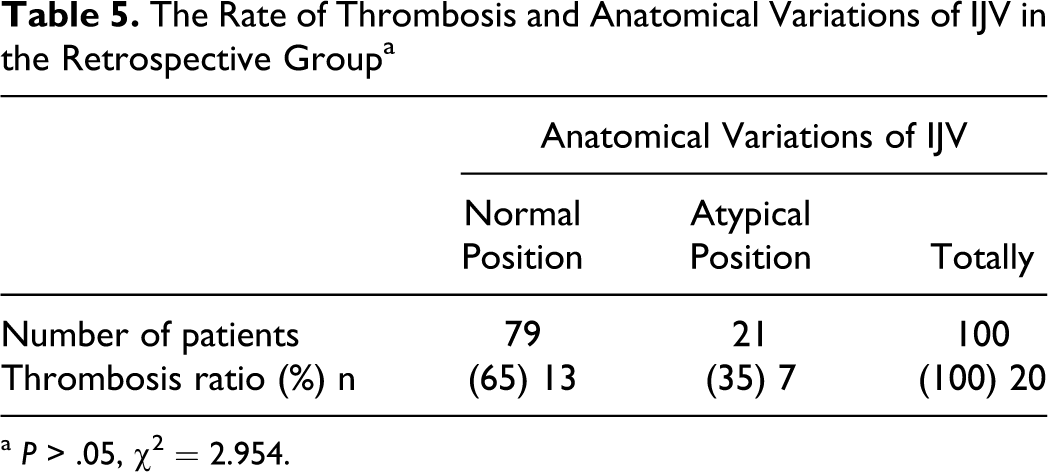
a P > .05, χ2 = 2.954.
Discussion
In this study it was revealed that IJV thrombosis was found in 25% of cases 10 days after catheterization for vascular access, and this ratio increased progressively after the time of catheterization. When retrospective cases were evaluated the thrombosis rate was 20%.
The frequency of thrombosis in IJV varies in different studies. It was detected as 2% in an early study, 6 but following studies revealed very higher numbers, such as 36.7% 7 and 63%. 8 A recent study revealed similar results. 9 In our study, the frequency of thrombosis in IJV was found as 20% (total thrombus in 25%) in the retrospective group and 58.3% (total thrombus in 20%) in the prospective group. In our study, the 25% thrombosis rate in prospective group at day 10 is impressive, and we could not find any data in literature regarding the thrombosis at such an early time after catheterization for the comparison. Effect of heparinization or any anticoagulant, antithrombotic therapy in the treatment or prophylaxis of IJV thrombosis should be evaluated; the lower rate of thrombosis in the retrospective group may be explained by the spontaneous recanalization of thrombosed vessel by the time. This ratio is still high and limits the availability of vascular access for the patient.
The risk of thrombosis increases as the duration of catheter remaining in situ prolongs. 10 We obtained similar results in our study. The frequency of thrombosis development increases as the number of catheter insertions increases.11 –13 Moreover, in our study, the rate of thrombosis was significantly higher in participants undergoing catheter insertion 3 times and more, compared to those who had undergone catheter insertion once or twice. Chou et al reported that there was a possibility that inflammation was related to the development of stenosis and thrombosis. 14 However, we did not detect a relationship between CRP and thrombosis.
The anatomical position of the IJV is generally lateral and anterior to the carotid artery. 15 Anatomical variations in IJV have been determined as 16% in some studies 16 and 36% in another. 17 This rate was 21% in the retrospective group in our study. In the light of these data, it is possible to state that the failure rate of catheter insertion into the IJV using the Landmark method (blinded) would be high. Likewise, USG-guided insertion has also been recommended in the Kidney Disease Outcomes Quality Initiative (K/DOQI) guideline. 18
When evaluated together with the risks, in particular the risk of thrombosis, the use of arteriovenous grafts of fistulae takes a priority rather than the catheter. K/DOQI, too, has recommended that catheter usage should be less than 10%. 19
The small number of study population is a limitation of the study especially for the prospective group. We did not use venography for the detection of thrombosis. Venography is the gold standard for the demonstration of thrombus. However, it is not frequently used as it is invasive and expensive.20,21
In conclusion, catheter-related IJV thrombosis is frequent in hemodialysis patients, when progressively followed this ratio was 25% at day 10 after catheterization and 58.3% at the time of catheter removal and remained unchanged after 15 days. The thrombosis ratio was 20% in retrospective cases; long catheter remaining time and repeated catheterizations increase this rate. Whether the thrombosis follow-up is necessary after catheterizations and treatment opportunities in terms of prevention of vascular access limitations should be evaluated in further clinical trials.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.