
Abstract
We retrospectively studied 89 patients with chronic hepatitis C virus (HCV) infection, including 50 chronic hepatitis (CH) cases, 18 liver cirrhosis (LC) cases, and 21 LC with hepatocellular carcinoma (LC + HCC) cases, with regard to various factors related with thrombocytopenia. The platelet count decreased with the stage advancement of liver diseases. Multiple regression analysis revealed that splenomegaly and von Willebrand factor (vWF) were explanatory variables that correlated with thrombocytopenia. Splenomegaly appears to be the most responsible factor, although there are a considerable number of thrombocytopenic cases without splenomegaly, suggesting other factors may also be responsible. The vWF level is inversely correlated with the platelet count. Soluble thrombomodulin, a marker of endothelial dysfunction, increases with the advancement of liver fibrosis. It is positively correlated with vWF and inversely with the platelet count. Our present results imply that vascular endothelial dysfunction is also involved in thrombocytopenia during chronic HCV infection.
Introduction
The platelet count is known to decrease in proportion to the advancement of the stage of liver disease in chronic hepatitis C virus (HCV) infection. Liver biopsy is the golden standard for evaluating the stage of fibrosis in HCV patients. It is, however, a considerably invasive procedure and more simple, non-invasive laboratory methods capable of predicting the stage of fibrosis would be of great help in clinical settings. A strong correlation between liver fibrosis and thrombocytopenia has been noted in a number of papers, and the platelet count is presently used as an index for fibrosis staging.1,2
Thrombocytopenia in liver fibrosis can be attributed to (1) platelet destruction/sequestration by the spleen, (2) the decreased production of platelets, and (3) platelet consumption. Based on several papers that have reported a strong correlation between spleen size and thrombocytopenia,3–5 platelet destruction/sequestration as a result of splenomegaly caused by portal hypertension has been considered to be the most important determinant. On the other hand, a splenectomy or portal vein shunting does not necessarily normalize the platelet count,6,7 suggesting that factors other than splenomegaly are also operative in reducing the platelet count during liver fibrosis.
Since thrombopoietin (TPO), which facilitates the proliferation and differentiation of the megakaryocytic lineage (resulting in the production of platelets), is released from the liver, some reports have suggested that inadequate TPO production is at least partly responsible for thrombocytopenia in liver fibrosis.4,8–11 The expression level of c-mpl, the TPO receptor, is also reportedly low in patients with liver cirrhosis. 12 On the other hand, some reports have argued against a correlation between thrombocytopenia and hepatic TPO production, 13 and whether decreased thrombopoiesis contributes to thrombocytopenia during liver fibrosis awaits further elucidation.
As for platelet consumption, several hypotheses related to von Willebrand factor (vWF) have been proposed. Inflammatory changes that accompany chronic HCV hepatitis and liver cirrhosis may lead to an increase in the vWF level, resulting in platelet consumption.14–16 The impaired hepatic production of ADAMTS13 (a disintegrin and metalloprotease with a thrombospondin type 1 motif, member 13) and its activity, which cleaves vWF, may also lead to an increase in ultra-large multimers of vWF, resulting in platelet microthrombi formation 17 and consumptive thrombocytopenia, similar to the conditions observed with thrombotic thrombocytopenic purpura (TTP).
In the present study, we evaluated various factors, including spleen size, TPO, vWF, and ADAMTS13, as well as general hematological, biochemical, and coagulation parameters in patients with chronic HCV infection, with fibrosis stages ranging from a relative early phase to an advanced stage of liver cirrhosis and attempted to determine the contributing power of each factor to thrombocytopenia using a multiple regression analysis and other analytical methods.
Materials and Methods
Patients
Our study was made up of 89 patients with chronic HCV infection who had been referred to the outpatient clinic of the University of Yamanashi Hospital. Based on the chronic HCV staging, 50 patients had chronic hepatitis (CH), 18 patients had liver cirrhosis (LC), and 21 patients had liver cirrhosis plus hepatocellular carcinoma (LC + HCC). The diagnosis of chronic hepatitis and LC was made by an expert in hepatology (M.S.), fundamentally using the score of Fib-4. 18 Fib-4 was calculated according to the formula of (age × AST/(platelets × ALT0.5)), and the cases exceeding the score of 3.25 were diagnosed as LC. The study was endorsed by the Institutional Review Board of the University of Yamanashi (No. 224), and all the patients gave their written informed consent prior to participation in the study. Blood was withdrawn from the ante-cubital vein; after laboratory measurements for diagnostic purposes, the residual samples were used to assess various factors that may be involved in thrombocytopenia.
Methods
A complete blood count (CBC) analysis was performed using an SE-3000 (Sysmex Co, Kobe, Japan). Serum and plasma anticoagulated with citrate were obtained by centrifugation of the whole blood within 2 hours of blood collection and were stored at −80°C until measurement.
Repeated freezing was avoided as much as possible; when necessary, the thawing of the frozen serum and plasma was performed at 37°C. Biochemical parameters, including albumin, alanine aminotransferase (ALT), and total bilirubin, were measured using a BM-2000 (JEOL Ltd, Tokyo, Japan). The vWF antigen level was determined using STA-LIA kits (Roche Diagnostics K.K., Tokyo Japan), and the ADAMTS13 antigen level was determined using ADAMTS13 ELISA kits (Mitsubishi Chemical Medience Co, Tokyo, Japan).
19
ADAMTS13 activity was measured using the ADAMTS13 Activity Kit (Kainos Laboratories, Tokyo, Japan),
20
thrombomodulin (TM) was measured using TM (MKI) EIA kits (Mitsubishi Kagaku Iatron Co Ltd), and TPO was measured using Human TPO Immunoassay kits (R&D Systems, Minneapolis). For coagulation and fibrinolysis testing, an LPIA A-700 (Mitsubishi Chemical Medience Co) was used to measure the prothrombin time, with results expressed as international normalized ratio (PT-INR),
Statistical Analysis
The analysis of the biochemical parameters, coagulation/fibrinolysis factors, SI index, and so on, and the multiple regression analysis were preformed using the data analysis software STAT FLEX, Ver. 4.1 (Artec, Ltd, Osaka, Japan).
Results
Patient Background
The numbers and sex (male/female) of patients at each stage was 50 patients (37/13) with CH, 18 patients (7/11) with LC, and 21 patients (9/12) with LC + HCC. The patient age tended to increase with the progression of the fibrosis stages: 57.4 ± 10.6 years among patients with CH, 65.3 ± 9.5 years among patients with LC, and 70.0 ± 9.1 years among patients with LC + HCC. The CBC profile, biochemical parameters, coagulation/fibrinolysis factors, and inflammation markers are summarized according to each stage in Table 1 .
Clinical Characteristics of Patients With Chronic HCV Infection
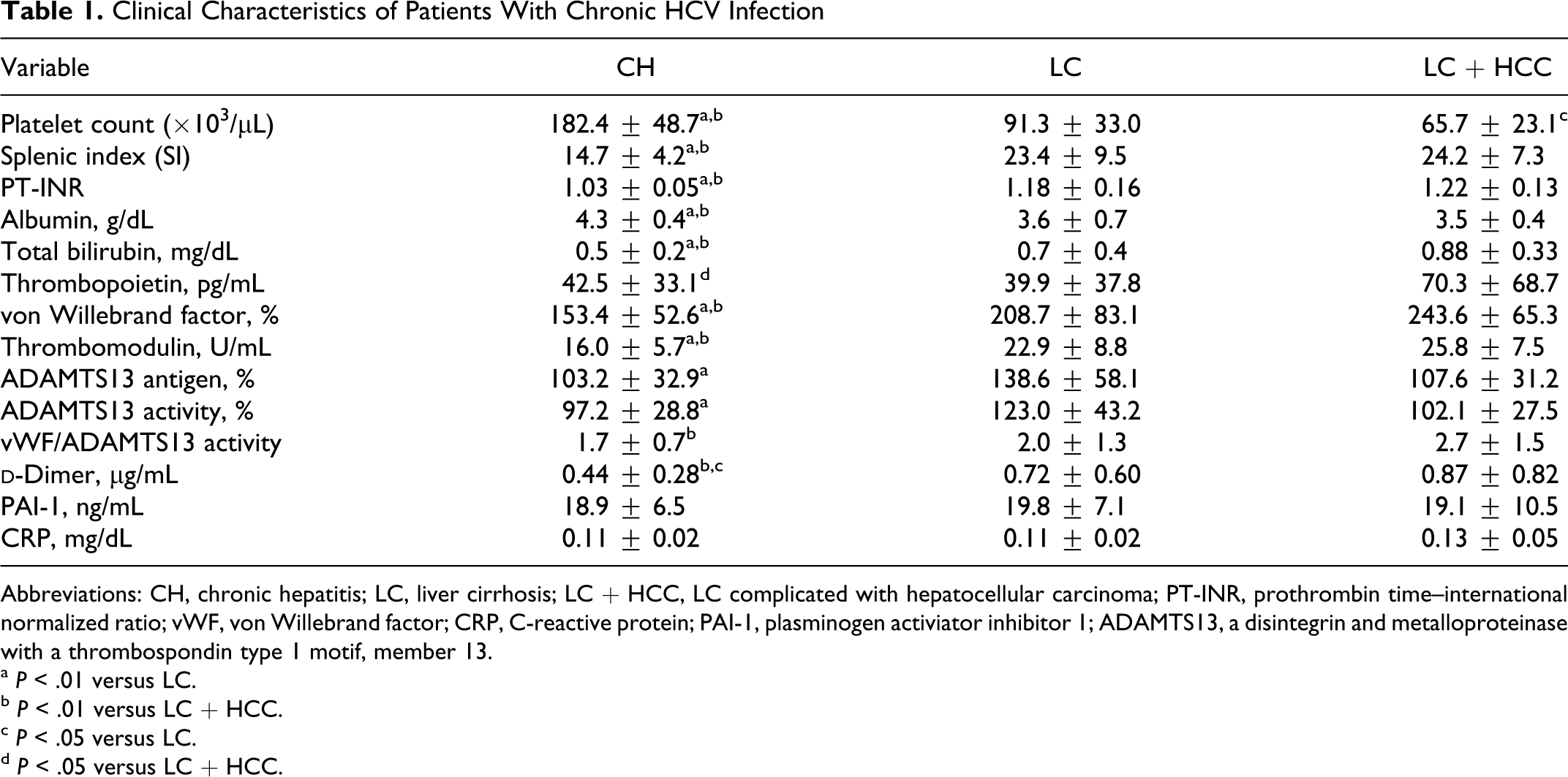
Abbreviations: CH, chronic hepatitis; LC, liver cirrhosis; LC + HCC, LC complicated with hepatocellular carcinoma; PT-INR, prothrombin time–international normalized ratio; vWF, von Willebrand factor; CRP, C-reactive protein; PAI-1, plasminogen activiator inhibitor 1; ADAMTS13, a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13.
a P < .01 versus LC.
b P < .01 versus LC + HCC.
c P < .05 versus LC.
d P < .05 versus LC + HCC.
Platelet Count
The platelet count decreased with the progression of fibrosis staging, and significant differences in the platelet count were observed between the stages: 182.8 ± 47.5 × 103/μL among patients with CH, 85.9 ± 33.6 × 103/μL among patients with LC, and 66.7 ± 25.2 × 103/μL among patients with LC + HCC (Table 1 and Figure 1 ).
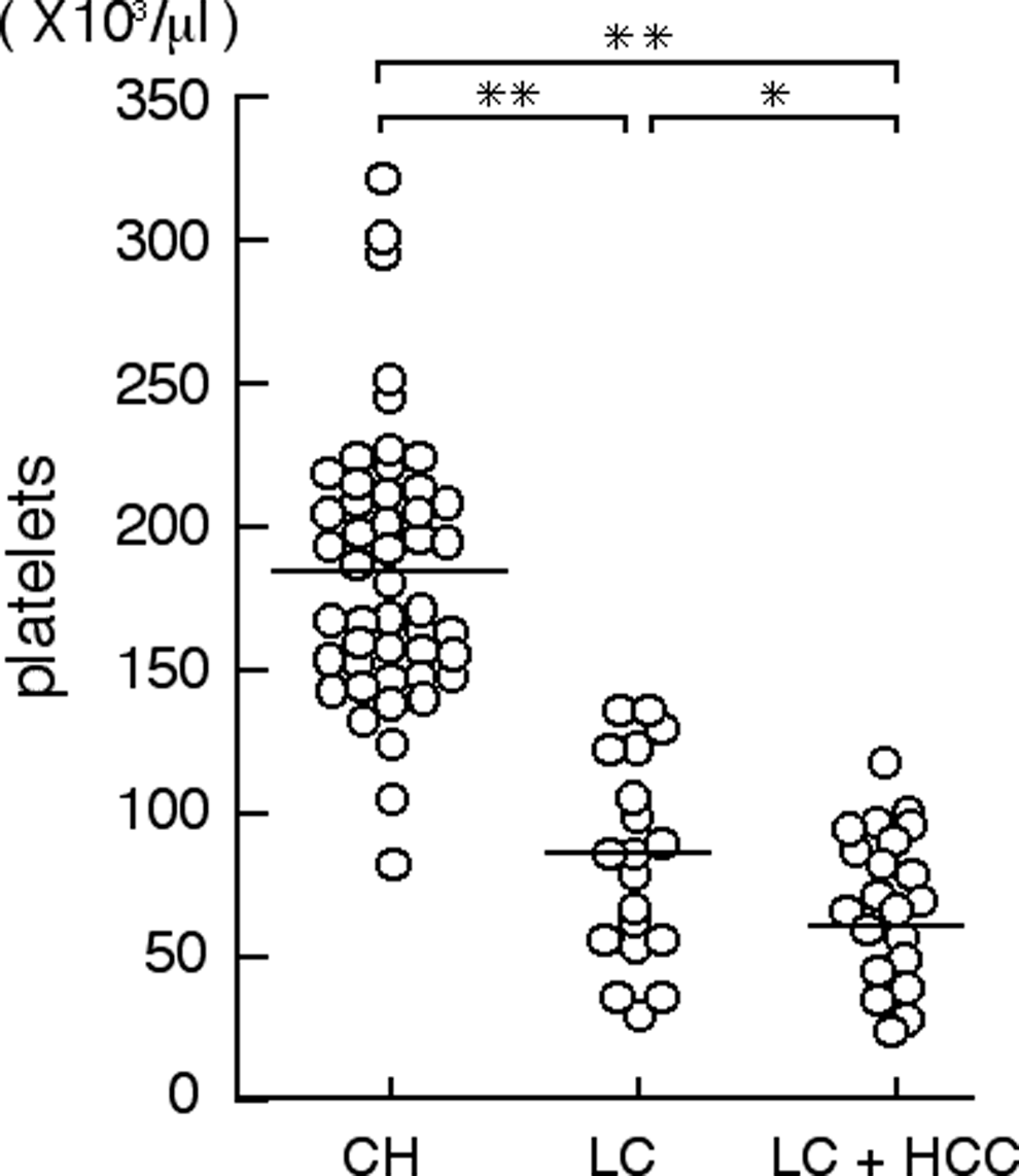
Platelet counts in chronic hepatitis C virus (HCV) infection patients with chronic hepatitis (CH), liver cirrhosis (LC), and liver cirrhosis complicated by hepatocellular carcinoma (LC + HCC). The open circles represent each individual patient, and the mean of each patient group is indicated by the horizontal line. Statistical differences are indicated with *P < .05 and **P < .01.
Liver Function
Prothrombin time–international normalized ratio (PT-INR), which represents the overall coagulation capacity of the extrinsic pathway, is a good marker for hepatic protein synthesis. Prothrombin time–international normalized ratio was positively correlated with the progression of the fibrosis stages; 1.03 ± 0.05 among patients with CH, 1.18 ± 0.16 among patients with LC, and 1.22 ± 1.13 among patients with LC + HCC; significant differences were observed among the stages (P < .01; Table 1). A negative correlation was seen between PT-INR and the platelet count (r = −.71, P < .0001), suggesting that the platelet count decreases with impaired liver function in patients with chronic HCV infection (Figure 2). A positive correlation (r = .59, P < .0001) was observed between the platelet count and the albumin level, which represents hepatic protein synthesis, and an inverse correlation was observed between the platelet count and the total bilirubin level, the elevation of which represents a fibrosis-related impairment in bile secretion (r = −.49, P < .0001). Of these markers of liver function, the coefficient value of PT-INR exceeded those of the others. A negative correlation was also observed between PT-INR and the albumin level (r = −.73, P < 0.0001), and a positive correlation was observed between PT-INR and the total bilirubin level (r = .76, P < .0001).
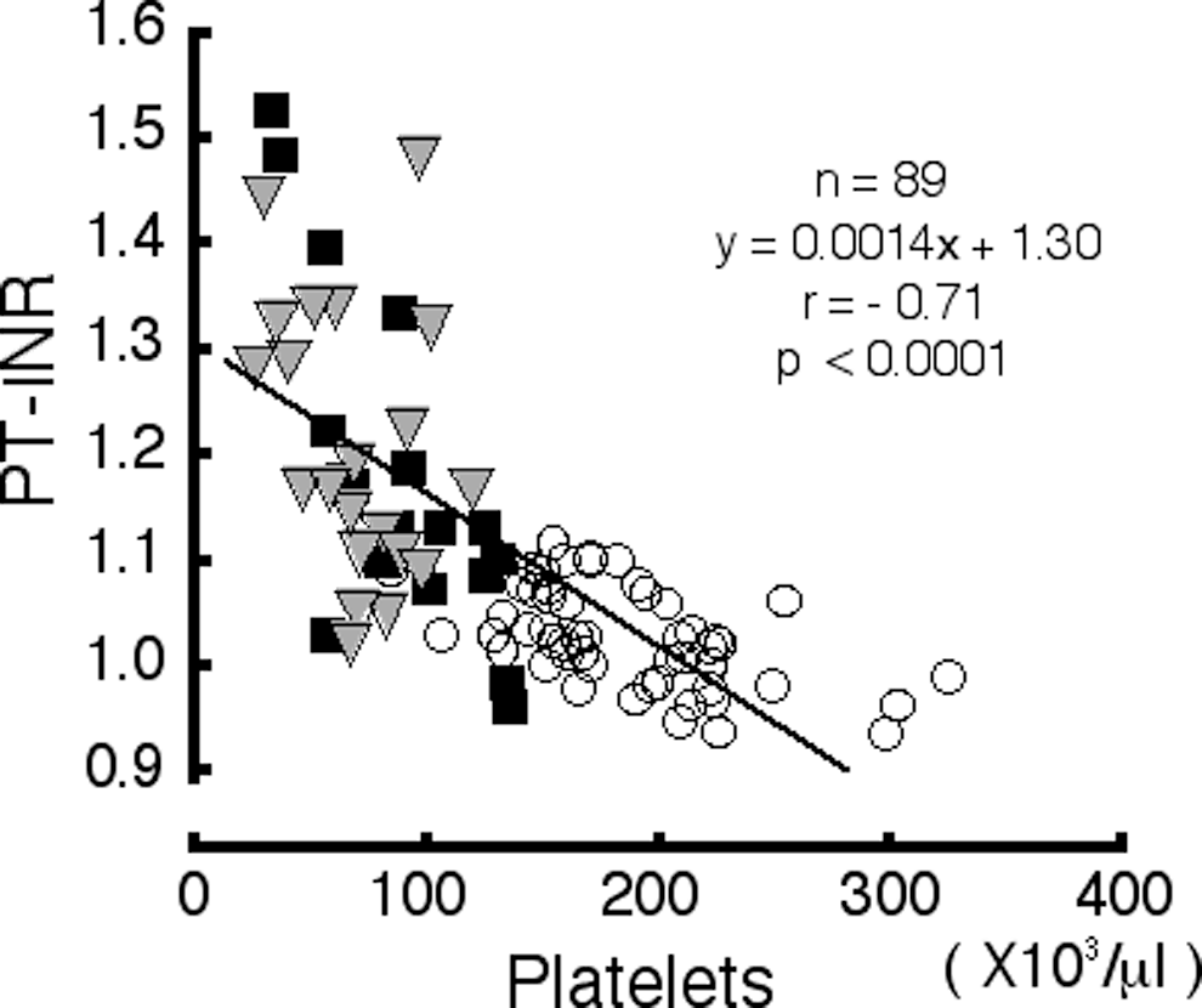
Scattergram showing the correlation between prothrombin time–international normalized ratio (PT-INR) and the platelet count (r = −.71, P < .0001). The line represents the linear regression of PT-INR versus platelet count. The symbols represent the patients as follows: open circle, chronic hepatitis (CH); square, liver cirrhosis (LC); and triangle, liver cirrhosis complicated by hepatocellular carcinoma (LC + HCC).
Splenomegaly
Splenomegaly is considered to be one of the major causes of thrombocytopenia during chronic HCV infection. The SI was 14.7 ± 4.2 among the patients with CH, 23.7 ± 9.2 among the patient with LC, and 25.3 ± 8.2 among the patients with LC + HCC. These values were significantly different (P < .01; Table 1), suggesting that splenomegaly increases in size with the progression of the fibrosis stage. A negative correlation was observed between the platelet count and the splenomegaly (r = −.65, P < .0001; Figure 3), confirming the previous notion that the thrombocytopenia was attributable to splenomegaly in proportion to the stage of progression. On the other hand, of the 33 patients with a platelet count of less than 100 × 103/μL, 8 patients had no significant splenomegaly, while 25 patients had splenomegaly with SI values higher than 20. These findings imply that there are some cases of thrombocytopenia that are unexplainable by splenomegaly.
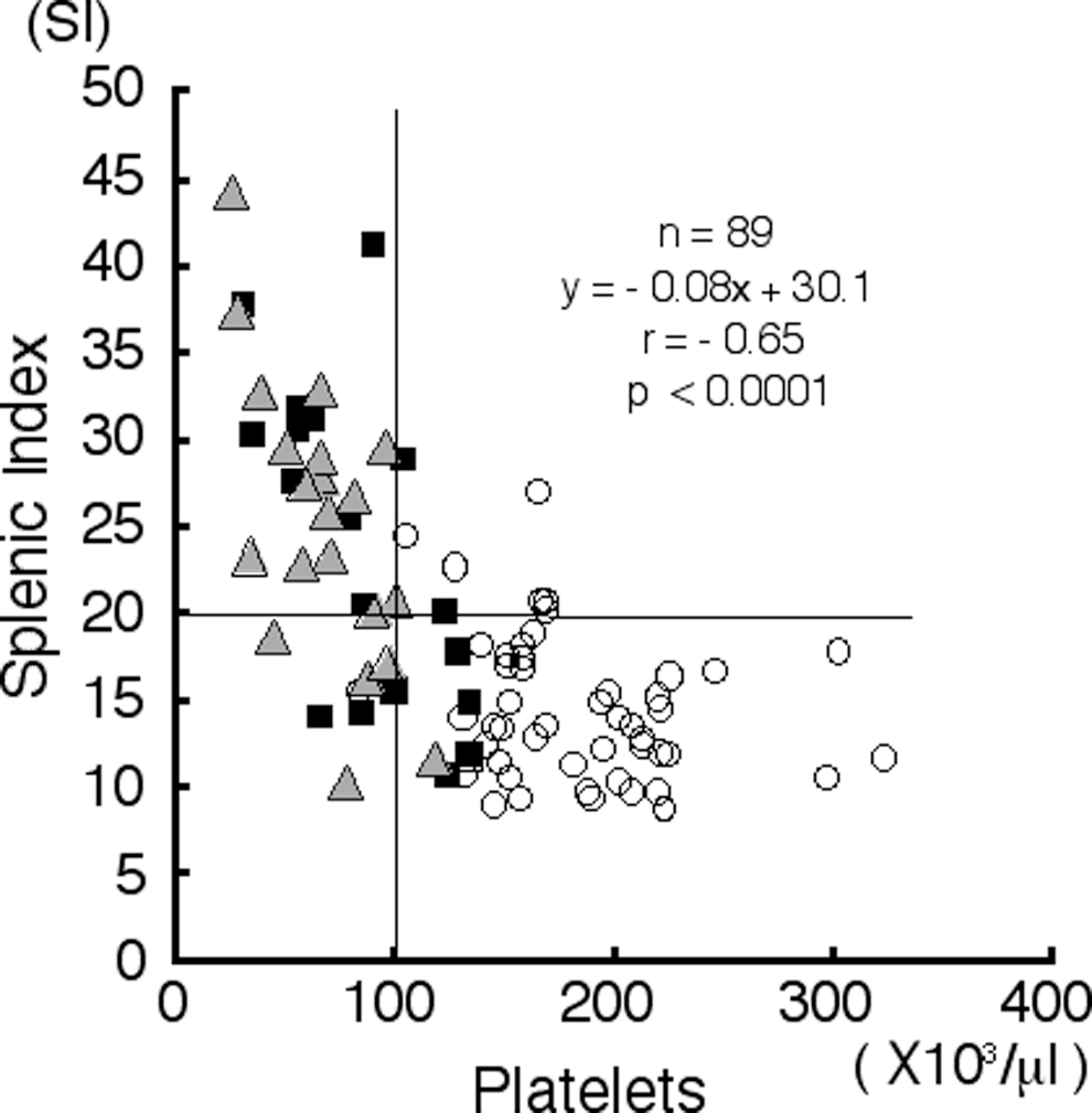
Scattergram showing the correlation between the platelet count and the splenic index (SI; r = −.65, P < .0001). The horizontal and vertical lines denote the cutoff values used to define splenomegaly, with SI values higher than 20 and thrombocytopenia with a platelet count less than 100 × 103 cells/µL, respectively. The symbols represent the patients as follows: open circle, chronic hepatitis (CH); square, liver cirrhosis (LC); and triangle, liver cirrhosis complicated by hepatocellular carcinoma (LC + HCC).
Thrombopoietin
The TPO concentrations were 42.5 ± 33.1 pg/mL among patients with CH, 39.9 ± 37.8 pg/mL among patients with LC, and 70.3 ± 68.7 pg/mL among patients with LC + HCC, respectively; no significant differences were observed among the stages (Table 1). No correlation between the platelet count and the TPO concentration was seen (r = −.23, P < .0475).
von Willebrand factor Antigen
The vWF antigen values were 153.4% ± 52.6% among patients with CH, 208.7% ± 83.1% among patients with LC, and 243.6% ± 65.3% among patients with LC + HCC. These values were significantly different (P < .01; Table 1), suggesting that vWF antigen increases with the progression of the stage of chronic HCV infection. A negative correlation was observed between the platelet count and the vWF antigen value (r = −.54, P < .0001; Figure 4).
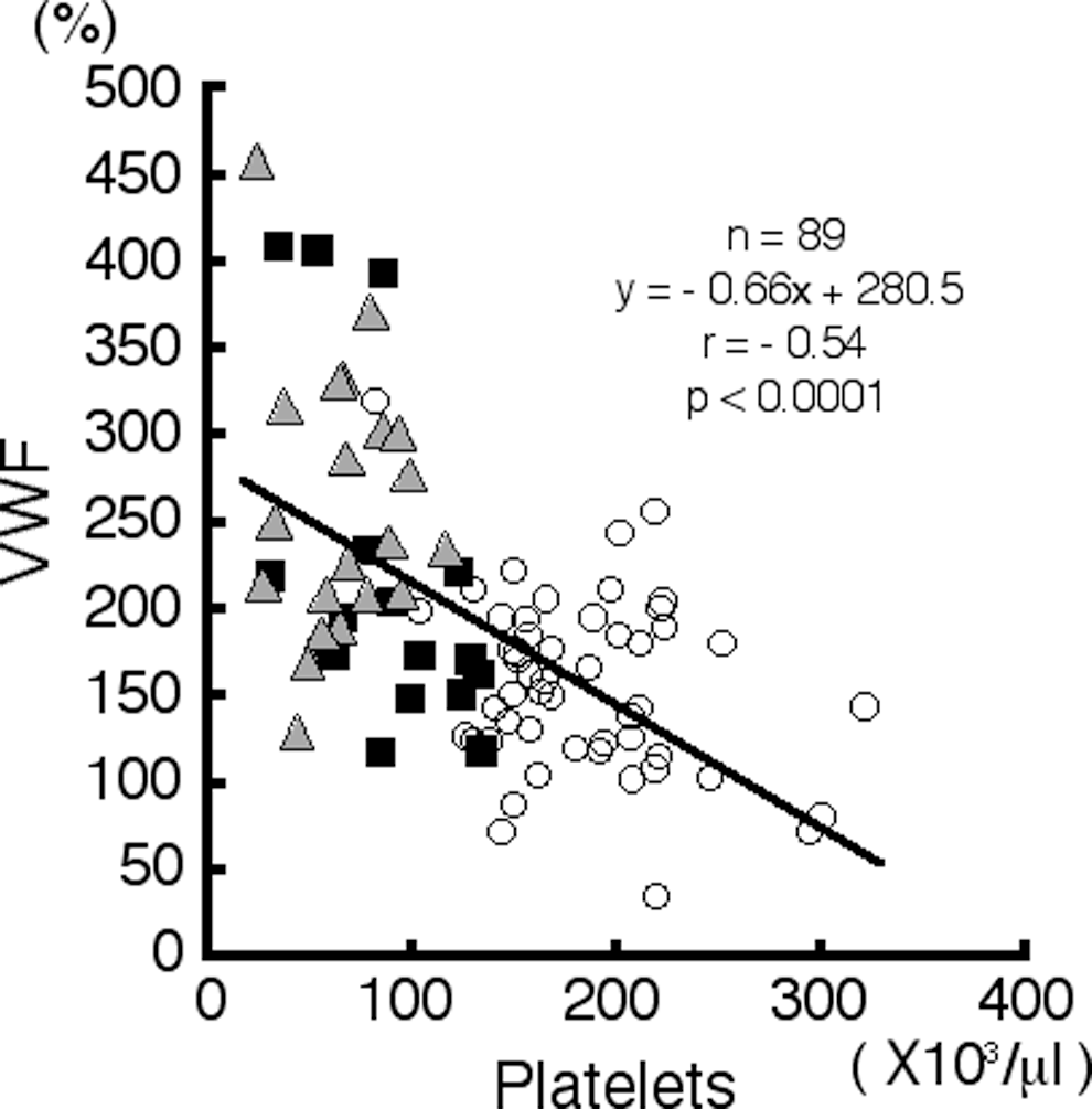
Scattergram showing the correlation between the von Willebrand factor (vWF) antigen value and the platelet count (r = −.54, P < .0001). The line represents the linear regression of vWF antigen versus the platelet count. The symbols represent the patients as follows: open circle, chronic hepatitis (CH); square, liver cirrhosis (LC); and triangle, liver cirrhosis complicated by hepatocellular carcinoma (LC + HCC).
Thrombomodulin
Thrombomodulin is often used as a marker of endothelial cell damage. As expected, the TM values were 16.0 ± 5.7 U/mL among patients with CH, 22.9 ± 8.8 U/mL among patients with LC, and 25.8 ± 7.5 U/mL among patients with LC + HCC. These values were significantly different (P < .01; Table 1). A negative correlation was observed between the platelet count and the TM value (r = −.51, P < .0001; Figure 5A), and a positive correlation was observed between the vWF antigen value and the TM value (r = .48, P < .0001; Figure 5B).
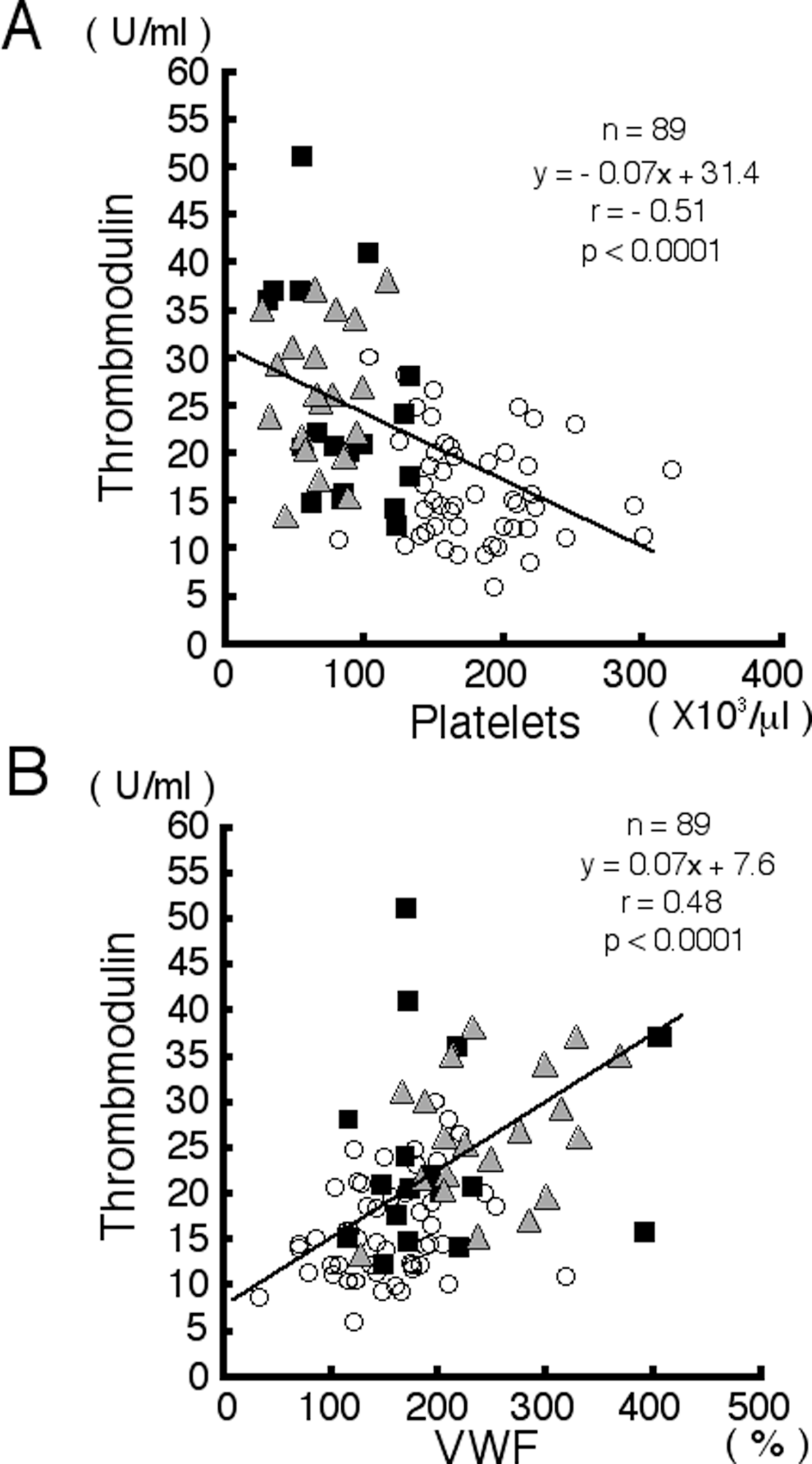
Scattergram showing the correlation between thrombomodulin (TM) and the platelet count (r = −.51, P < .0001) (A) and between TM and the von Willebrand factor (vWF) antigen value (r = .48, P < .0001) (B). The line represents the linear regression. The symbols represent the patients as follows: open circle, chronic hepatitis (CH); square, liver cirrhosis (LC); and triangle, liver cirrhosis complicated by hepatocellular carcinoma (LC + HCC).
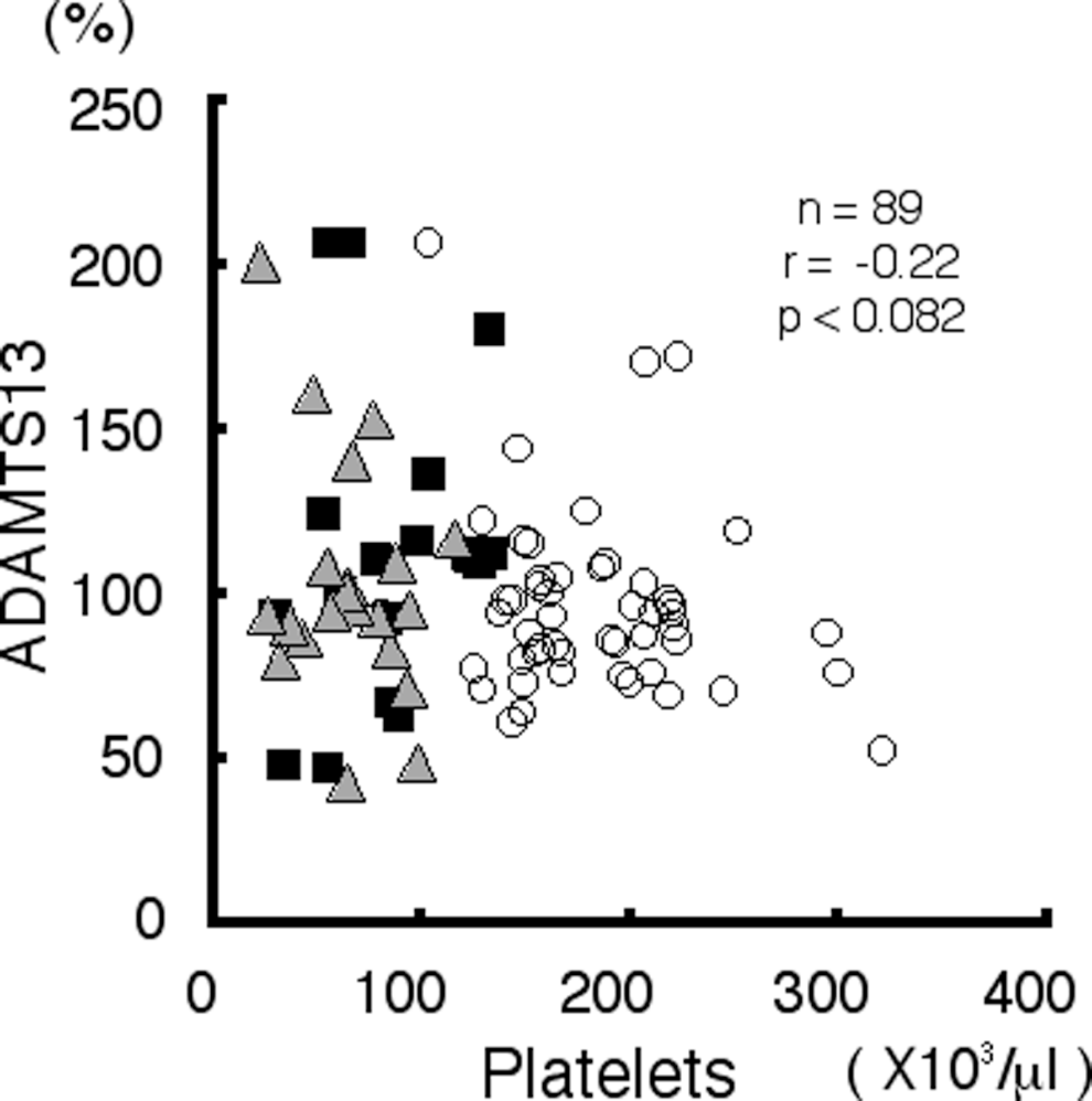
Scattergram showing the correlation between ADAMTS13 activity and the platelet count (r = −.22, P < .0825). The symbols represent the patients as follows: open circle, chronic hepatitis (CH); square, liver cirrhosis (LC); and triangle, liver cirrhosis complicated by hepatocellular carcinoma (LC + HCC).
ADAMTS13
A decrease in ADAMTS13 activity is known to result in an increase in ultra-large vWF multimers, which is associated with a low platelet count. The ADAMTS13 activities were 97.2% ± 28.8% among patients with CH, 123.0% ± 43.2% among patients with LC, and 102.1% ± 27.5% among patients with LC + HCC. No significant differences were observed among the stages (Table 1). Neither a correlation between ADAMTS13 activity and the platelet count (r = −.22, P < .0825; Figure 6) nor a correlation between ADAMTS13 activity and the VWF antigen value was observed (r = −.02, P < .8746).
Multiple Regression Analysis
With the parameters measured in this study, we performed a multiple regression analysis using thrombocytopenia as the target index. As a result, splenomegaly, PT-INR, and the vWF antigen value were extracted as factors that were significantly responsible for thrombocytopenia (Table 2 , panel A). Since splenomegaly is related to the impairment of liver function, with which the PT level is assumed to be associated, we also performed an analysis without PT-INR, revealing splenomegaly and the vWF antigen value as significant factors (Table 2, panel B). We further performed a stratified analysis, in which the patients were subdivided into 4 groups, based on 2 parameters: splenomegaly (+, SI > 20) or (−) and thrombocytopenia (+, platelet count < 100 × 103 cells/μL) or (−). In the splenomegaly (+) group, significant differences in spleen size (SI), liver function, and the vWF antigen value were observed between the thrombocytopenia (+) group and (−) group (Table 3 ). Taking into consideration the fact that impaired liver function is related to splenomegaly and that these 2 factors may be evaluated as one in this group, splenomegaly appears to be the major determinant of thrombocytopenia. However, among the 55 cases without splenomegaly, a significant increase in the vWF antigen value and PT-INR was observed in the thrombocytopenia (+) group compared with the (−) group, while no difference in spleen size or platelet count was observed. Thus, in the group of patients without splenomegaly, some factors related to the vWF antigen increase or liver function impairment may play a role in inducing thrombocytopenia.
Multiple Regression Analysis of Variables Associated With Thrombocytopenia
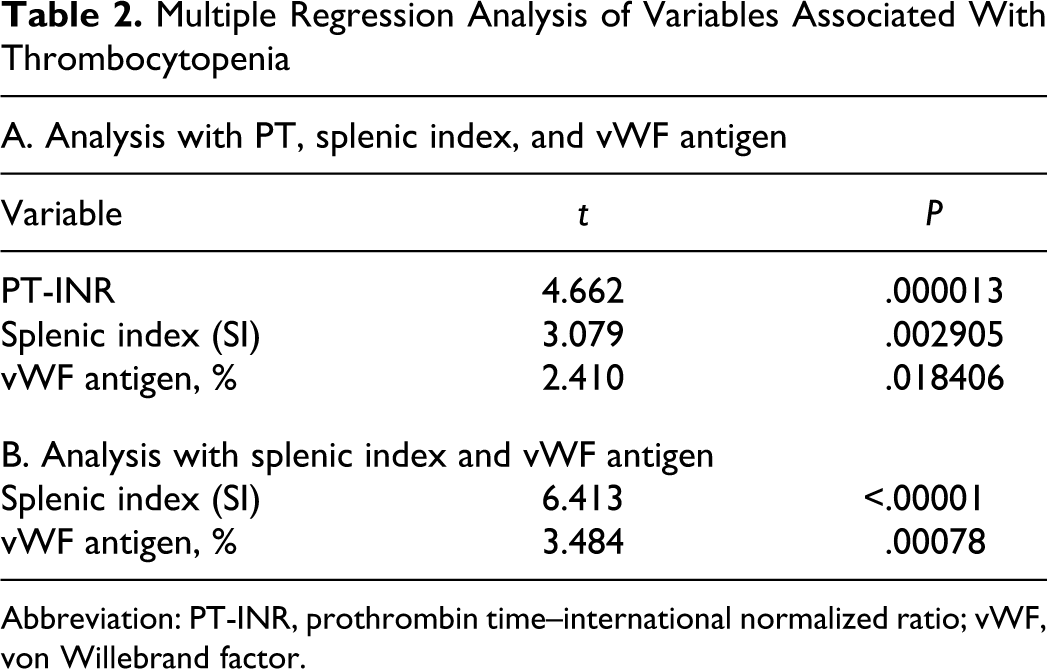
Abbreviation: PT-INR, prothrombin time–international normalized ratio; vWF, von Willebrand factor.
Stratified Analysis of Patients with Thrombocytopenia With or Without Splenomegaly
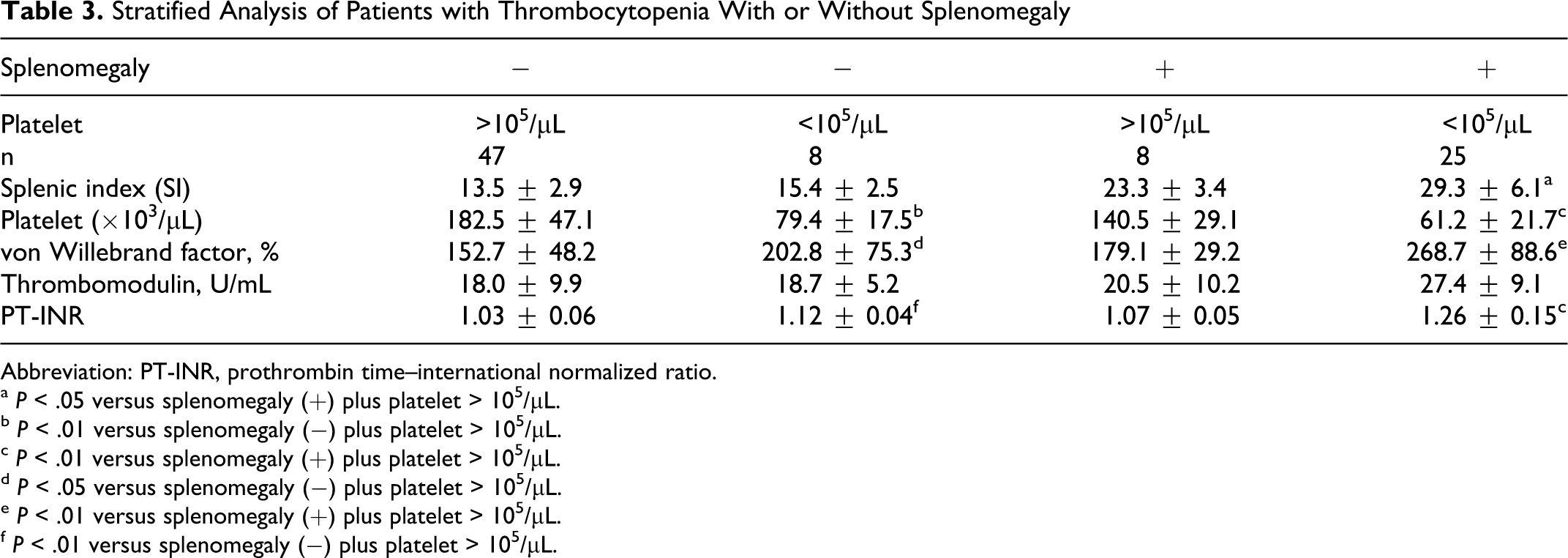
Abbreviation: PT-INR, prothrombin time–international normalized ratio.
a P < .05 versus splenomegaly (+) plus platelet > 105/μL.
b P < .01 versus splenomegaly (−) plus platelet > 105/μL.
c P < .01 versus splenomegaly (+) plus platelet > 105/μL.
d P < .05 versus splenomegaly (−) plus platelet > 105/μL.
e P < .01 versus splenomegaly (+) plus platelet > 105/μL.
f P < .01 versus splenomegaly (−) plus platelet > 105/μL.
Other Markers
Fibrinolysis markers such as
Discussion
Thrombocytopenia in chronic HCV infection may be caused by platelet destruction/sequestration, the decreased production of platelets, or platelet consumption. In this study, we sought to evaluate the roles of various factors that may contribute to thrombocytopenia.
Platelet destruction/sequestration by splenomegaly induced by liver fibrosis is a major cause of thrombocytopenia. In this study, examining 89 patients infected with HCV, splenomegaly, impaired liver function as represented by PT, and the vWF antigen value were correlated well with thrombocytopenia, and a multiple regression analysis also extracted these 3 parameters as explanatory variables for thrombocytopenia, confirming the results of previous reports.4,14–16 Since splenomegaly and PT are partially dependent, we removed PT from the analysis to extract other underlying factors; only splenomegaly and the vWF antigen value were identified as major determinants of thrombocytopenia, with splenomegaly exhibiting the stronger dependence. On the other hand, a splenectomy or the shunting of the portal veins does not necessarily correct the low platelet count,6,21 suggesting that some mechanism other than splenomegaly is responsible for thrombocytopenia in liver fibrosis induced by HCV infection. In our stratified analysis of 55 cases without splenomegaly (SI < 20), significant differences in the vWF antigen value and PT were observed between the thrombocytopenia (+) group and the thrombocytopenia (−) group, although no significant difference in spleen size was noted. These findings suggest that even among cases without splenomegaly, thrombocytopenia is induced by some other factors that may be related to an elevation in the vWF antigen level or the impairment of liver function.
The impaired production of platelets, that is, impaired thrombopoiesis, may be partially responsible for thrombocytopenia in patients infected with HCV. Thrombopoietin is a major cytokine that stimulates the proliferation and differentiation of the megakaryocytic lineage, with resultant platelet production.22,23 Since TPO is produced by the liver, impaired liver function in chronic HCV infection may lead to a low level of TPO in the blood, which cannot maintain normal thrombopoiesis in the bone marrow and the peripheral platelet count. 24 In agreement with this hypothesis, a negative correlation between the blood TPO level and the progression of the stage of liver disease has been reported in patients with HCV infection. 25 On the other hand, a previous study hypothesized that the total blood TPO is maintained at a certain level, irrespective of liver function, and that the blood TPO level is inversely related to the platelet count since TPO binding to its receptors on platelets and megakaryocytes tends to lower the blood TPO level. 26 Based on this hypothesis, it follows that the blood TPO is elevated in proportion to the severity of thrombocytopenia in patients with chronic HCV infection. In the present study, we found that no correlation existed between the platelet count and the blood TPO level, although the blood TPO level tended to be elevated in the LC + HCC group. A multiple regression analysis did not recognize TPO as an explanatory factor, and it is likely that TPO contributes minimally to thrombocytopenia in patients with chronic HCV infection. Consistently, recent reports have proposed that TPO produced by stromal cells in the bone marrow acts locally on megakaryocytes27,28 and that the blood TPO level does not reflect thrombopoiesis in the bone marrow. 29
Other hypotheses have also been presented in relation to vWF-induced platelet consumption, which accounts for the thrombocytopenia in patients infected with HCV. von Willebrand factor associates with Glycoprotein IB (GPIB) molecules on the platelet membrane and leads to platelet adhesion/aggregation at sites of vascular damage. If the blood vWF level is increased in patients with liver fibrosis, its interaction with platelets may lead to the increased consumption of platelets, resulting in thrombocytopenia.14–16,30 von Willebrand factor antigen has been reported to increase significantly with the progression of the stage of liver fibrosis, 30 and vWF production has been postulated to be facilitated by the remodeling of the liver tissue or endotoxic damage to the hepatocytes 31 or extrahepatic organs, such as the spleen. 32 Recent reports on vWF regulation in patients with chronic HCV infection have focused on ADAMTS13 activity, which cleaves the vWF multimers. An elevated vWF antigen level in patients with chronic HCV infection may reflect a proportional decrease in ADAMTS13 activity and the existence of ultra-large vWF multimers, which are apt to react with platelets. 33 possibly leading to thrombocytopenia. In accordance with this notion, a recent report has demonstrated a correlation between the platelet count and ADAMTS13 activity in patients with advanced stages of liver fibrosis, including HCV infection. 17
Contrary to our expectation, we were unable to observe a significant correlation between ADAMTS13 antigen/activity (data not shown) and the platelet count in this study, and no significant differences in these ADAMTS13-related parameters were observed among the stages of liver fibrosis. The discrepancy between our study and previous reports, particularly that of Uemura, 17 appears to be attributable to the overall severity of liver fibrosis in patients evaluated in each study. The report of Uemura et al deals with a number of patients with considerably advanced stages of liver fibrosis, such as those complicated with ascites. The patient profile in terms of Child’s classification corresponded to 33 cases of CH, 35 cases of LC Child A, 33 cases of Child B, and 41 cases of Child C, with mean ADAMTS13 activities of 87%, 79%, 63%, and 31%, respectively. A clear difference in the ADAMTS13 activities was observed among the stages of liver fibrosis, with the lowest level observed with Child C. On the other hand, the patients in our study all attended our outpatient clinic on a regular basis, and the overall severity of liver fibrosis was far less than that of the series reported by Uemura, which was comprised of 50 cases of CH, 23 cases of LC Child A, 13 cases of Child B, and 3 cases of Child C; the ADAMTS13 activities were 95.9%, 119.5%, 92%, and 81%, respectively. Of note, the ADAMTS13 activities of even our Child B and C groups were fairly well retained (81%-92%), although these patients exhibited considerably severe thrombocytopenia. Recent reports on the pathogenesis of TTP have demonstrated that severe ADAMTS13 activity of less than 3% is required to increase ultra-large vWF multimers, resulting in thrombocytopenia.34–36 It is also now known that a simple deficiency in ADAMTS13 does not lead to overt TTP. 37 Furthermore, hepatic stellate cells have been reported to possibly be a key factor in the reduction of plasma ADAMTS13 activities in rats with liver injury. 38 Taken together with the findings of these previous reports, our findings that thrombocytopenia occurs in the apparent absence of clear changes in ADAMTS13 activity suggests that ADAMTS13 changes may not be heavily involved in thrombocytopenia during chronic HCV infection.
Stellate cells appear to play an important role in liver fibrosis, and it is well known that the number of hepatic stellate cells is increased in cirrhotic liver in humans as well as rats. Furthermore, the current study revealed a relation between the increased production of ADAMTS13 and the enhanced plasma ADAMTS13 activity in a rat model of steatohepatitis during the process of liver fibrosis, where hepatic stellate cells are known to proliferate, suggesting that hepatic stellate cells in the liver play a significant role in the regulation of plasma ADAMTS13 activity. 39 Thus, it is speculated that stellate cells remain functional until the very last stage of liver fibrosis, 25 and the level of ADAMTS13, which is produced by stellate cells, may be maintained until the most advanced stage of liver cirrhosis, 40 which agrees well with our findings and those of a previous report 30 in which little difference in the ADAMTS13 level was noted among the different stages of liver fibrosis. The regulatory mechanism responsible for ADAMTS13 production by hepatic stellate cells in advanced cirrhosis and the inactivation of ADAMTS13 in humans requires further elucidation.
The vWF antigen value increased significantly with the progression of the stage of liver fibrosis in this study, in agreement with the results of a previous report. 30 Since the vWF value was not correlated with that of ADAMTS13, the increase in the vWF antigen value is likely due to its release from activated endothelial cells. von Willebrand factor antigen is negatively correlated with the platelet count; in the multiple regression analysis, it was extracted as an explanatory variable for thrombocytopenia, although the P value was significance less than that for splenomegaly. Thus, an elevation in the vWF antigen value may be partly responsible for the thrombocytopenia in patients with chronic HCV infection. However, the reference value for vWF antigen is considerably wide among healthy individuals, and further studies are needed to determine whether the difference in the vWF antigen value according to the stage of fibrosis is related to thrombocytopenia and to elucidate the possible mechanism.
Thrombomodulin is expressed on vascular endothelial cells and acts to regulate coagulation pathways by interacting with thrombin, producing activated protein C. Since TM is cleaved and released into the circulation during inflammatory processes, it is used as a marker of endothelial cell damage. Of particular interest is that this marker can be used to predict endothelial damage in the liver, independent of systemic circulation. 41 In this study, we found that the TM level increased with the progression of the stage of liver fibrosis, in the absence of an elevation in the CRP level, representing systemic inflammation. In chronic HCV infection, inflammatory processes in the liver are assumed to play a role in fibrotic changes, and our findings suggest that TM can be a good marker in predicting endothelial damage, that is, the process of inflammation and fibrosis in the liver. Although a negative correlation was observed between TM and the platelet count, this factor was not extracted as an explanatory variable in the multiple regression analysis. We found a good correlation between the vWF antigen value and TM (r = .48, P < .0001; Figure 4B), suggesting that both parameters may represent endothelial dysfunction induced by inflammatory changes in the liver. Thrombomodulin might not have been extracted as an explanatory variable in the multiple regression analysis as a result of its close association with vWF antigen. Our notion is in good agreement with a previous report that in liver damage induced by HBV and HCV infection in children, vWF antigen and TM can predict endothelial cell function. 42 Taken together, our findings, along with those of the previous report, suggest that TM can serve as a marker for inflammatory changes in the liver in patients with chronic HCV infection. Furthermore, thrombocytopenia in this disorder may be related to endothelial dysfunction revealed by its activation, that is, vWF release, and its damage, that is TM cleavage. This hypothesis seems consistent with previous results indicating that TM and vWF change in parallel as endothelial dysfunction markers. 43
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: supported by a grant from Charitable Trust Laboratory Medicine Research Foundation of Japan.