
Abstract
The Janus kinase 2V617F (JAK2 V617F) mutation is an acquired genetic defect that is considered to enhance thrombosis in Philadelphia chromosome-negative myeloproliferative neoplasms (MPNs). Thrombosis is also a well-defined component of Behcet syndrome (BS). The aim of this study was to determine the frequency of JAK2 V617F mutation in BS-associated thrombosis. A total of 152 patients with BS (62 with thrombosis and 90 without thrombosis) were enrolled. An additional 186 patients with MPNs and 107 healthy blood donors were included to serve as diseased and healthy controls, respectively. None of the patients with BS and healthy controls carried the JAK2 V617F mutation, whereas 67% of patients with MPNs were positive for JAK2 V617F . The frequency of thrombosis in patients with MPNs was not statistically different between carriers and non-carriers of JAK2 V617F mutation. Our data suggest that JAK2 V617F is not directly related to thrombosis in MPNs and in other thrombotic entities, such as BS.
Introduction
The Janus kinase 2V617F (JAK2V617F ) point mutation is a recently identified acquired genetic defect characteristically present in a majority of Philadelphia chromosome-negative myeloproliferative neoplasms (MPNs), including polycythemia vera (PV), essential thrombocythemia (ET), and primary myelofibrosis (PMF). 1–3 Since MPNs are frequently complicated by arterial and/or venous thrombosis, there has been considerable interest whether JAK2 V617F per se was associated with increased risk of thrombosis.
Hypothetically, JAK2 V617F mutation was proposed to enhance thrombosis mainly by creating a hypercoagulable state through rheological changes, activation of platelets, and leukocytes and by inducing hemostatic mechanisms in patients with PV and ET. 4,5 However, the exact mechanism by which this mutation causes thrombosis is not clear. Additional mechanisms, such as increased expression of adhesion molecules on red blood cells, platelet hyperresponsiveness, elevated soluble P-selectin levels, increased levels of circulating platelet–leukocyte aggregates, and disordered hemostasis, that attributed to the malfunctioning JAK2 gene have been reported. 6–8 [Please approve edits made to the sentence “Additional mechanisms that….”]
Whether the presence of the JAK2 V617F mutation, per se, modifies the thrombotic risk is currently debated. There is some clinical evidence to suggest that the mutation may variably be associated with thrombosis in MPNs, especially in patients with ET. 9 An increased rate of JAK2 V617F mutation has also been found in patients with unprovoked splanchnic vein thrombosis (SVT). 10–12 This finding encouraged other investigators to search for the thrombogenic potential of the JAK2 V617F mutation in other diseases. However, no association between JAK2 V617F and thrombosis has been demonstrated outside MPN, so far. 13,14 We, therefore, thought that it would be interesting to know the relation of JAK2 V617F mutation to thrombosis in a clinical condition that frequently presents with thrombotic events such as Behcet syndrome (BS).
Thrombosis is a well-defined feature of BS, and thrombotic complications are observed in more than one third of the patients. 15 The majority of vascular events involve veins; arterial thrombosis is less prominent. 16 Thrombotic events most commonly occur within the 5 years of disease onset. 17 However, in up to 30% of patients, vascular involvement has been reported to precede the diagnosis of BS. 18
Pathogenesis of thrombosis in BS has not been fully elucidated. Microvascular dysfunction, vascular cell injury as reflected by high levels of von Willebrand factor and thrombomodulin, platelet and leukocyte activation, and increased expression of adhesion molecules on endothelial cells are some of the mechanisms contributing to thrombosis in BS. 19–23 Data at hand show that there is no underlying abnormality in the hemostatic systems of the body. 24–26 The role of thrombophilic factors in BS-associated thrombosis has also been investigated by several groups. However, the results were conflicting and mostly inconclusive. 27–34
The aim of this study was to detect a potential relationship between JAK2 V617F mutation and BS-associated thrombosis and to compare this with the thrombotic events in MPNs.
Materials and Methods
Patients
In this cross-sectional survey between January 2009 and September 2009, we consecutively enrolled 62 patients with BS with acute or chronic arterial and/or venous thrombosis, 90 patients with BS and without thrombosis, and 107 healthy blood donors. A cohort of 186 patients with Ph(−) MPNs, diagnosed according to the World Health Organization criteria 35,36 and followed at the Hematology Department of Cerrahpasa Medical Faculty, Istanbul University, were also included. Since thrombosis in BS rarely occurs in women, 18 only male patients of older than equal to 18 years of age with BS, who fulfilled the International Study Group criteria 37 for BS, were included in the study. All patients with BS with acute and/or chronic arterial/venous thrombosis were designated as having “BS with thrombosis.” Knowing that the majority of BS-related thrombotic events generally occur either before or within the first 5 years of the diagnosis, 17 we defined patients with “BS without thrombosis” as those with a BS diagnosis of more than 5 years and having no history of vascular involvement.
Healthy controls consisted of male blood donors at the Blood Bank of Cerrahpasa Medical Faculty, Istanbul University for blood donation. They were included only if they did not have a history of arterial or venous thrombotic event and did not have clinical signs of thrombosis on examination.
Patients with a diagnosis of Ph(−) MPNs, mainly PV, served as diseased controls. The thrombotic events that these patients had experienced were recovered from patient charts retrospectively.
All patients and controls were inhabitants of Istanbul. Considering its ethnic composition, Istanbul’s population adequately represents Turkish population. The study was approved by the local ethics committee and conducted according to the principles of the Declaration of Helsinki. All included patients and healthy volunteers gave written consent before entering the study.
Methods
The JAK2 V617F mutation was detected by allele-specific polymerase chain reaction (PCR) in all recruited patients. Venous blood (2 mL) was drawn into EDTA-containing sample tubes (Greiner Bio-One GmBH, Kremsmünster, Austria) from patients and healthy controls by peripheral venipuncture. Using standard techniques as described elsewhere, 38 DNA was extracted from blood samples and stored at −70°C. Polymerase chain reaction amplification for the detection of JAK2 V617F and visualization of the PCR products were carried out using a commercial assay (Seeplex JAK2 Genotyping Kit; Seegene, Seoul, Korea).
Statistical Analysis
Statistical analysis was done with Statistical Package for the Social Sciences software, release 15.0 (SPSS Inc, Chicago, Illinois). Mann-Whitney U test was used for comparison. Odds ratios (ORs) were calculated to determine the role of JAK2 V617F mutation in thrombotic events in patients with MPN.
Results
Demographic and clinical features of the 152 patients with BS, 186 patients with MPNs, and 107 healthy controls are given in Table 1 . Among patients with BS, 62 had a history of documented thrombosis. Almost all of the thrombotic events were of venous origin; the deep vein thrombosis being the most frequently observed type of presentation.
Patient Characteristics
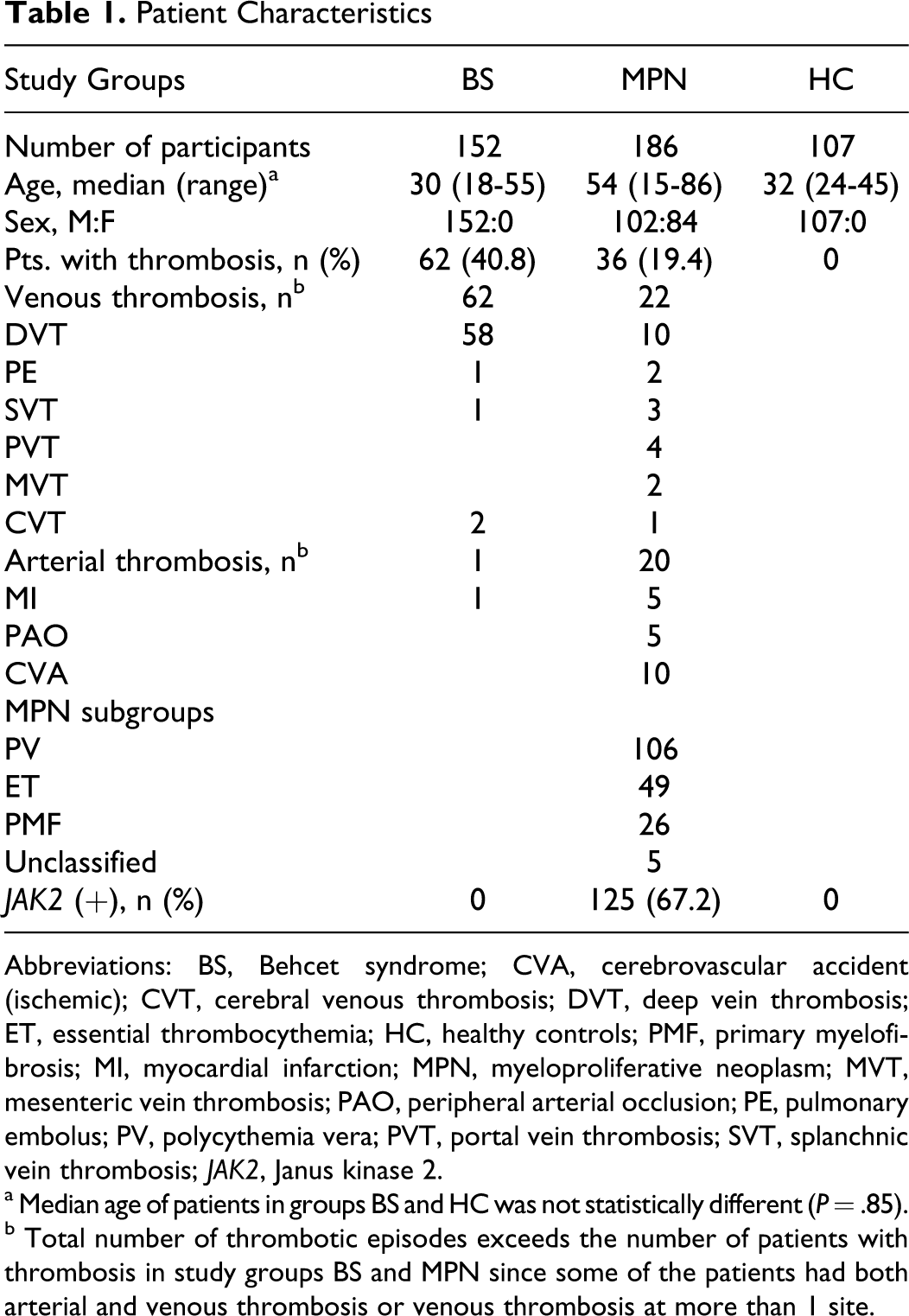
Abbreviations: BS, Behcet syndrome; CVA, cerebrovascular accident (ischemic); CVT, cerebral venous thrombosis; DVT, deep vein thrombosis; ET, essential thrombocythemia; HC, healthy controls; PMF, primary myelofibrosis; MI, myocardial infarction; MPN, myeloproliferative neoplasm; MVT, mesenteric vein thrombosis; PAO, peripheral arterial occlusion; PE, pulmonary embolus; PV, polycythemia vera; PVT, portal vein thrombosis; SVT, splanchnic vein thrombosis; JAK2, Janus kinase 2.
a Median age of patients in groups BS and HC was not statistically different (P = .85).
b
Among the 186 patients with MPNs, who constituted the diseased control group, PV was the most frequent MPN, followed by ET and PMF. In 5 patients, the subgroup of MPNs could not be identified. A total of 42 venous and arterial thrombotic events with almost equal frequencies had been observed in 36 (19.2%) of the 186 patients. Half of the venous thrombosis were located intra-abdominally.
None of the patients with BS, with or without thrombosis, had a JAK2 V617F mutation. The healthy controls were also negative for the JAK2 V617F mutation, whereas 67% of patients with MPNs were found to harbor the mutation.
There was no statistically significant difference between patients with JAK2 V617F (+) and (−) MPN in terms of the frequency of arterial and venous thrombotic events (P = .098; Table 2 ). We noted, however, that 8 of 9 patients with SVT and 7 of 10 patients with ischemic cerebrovascular events (CVEs) were carriers of JAK2 V617F mutation. Three patients had both arterial and venous thromboses.
Thrombotic Events in Patients with MPN
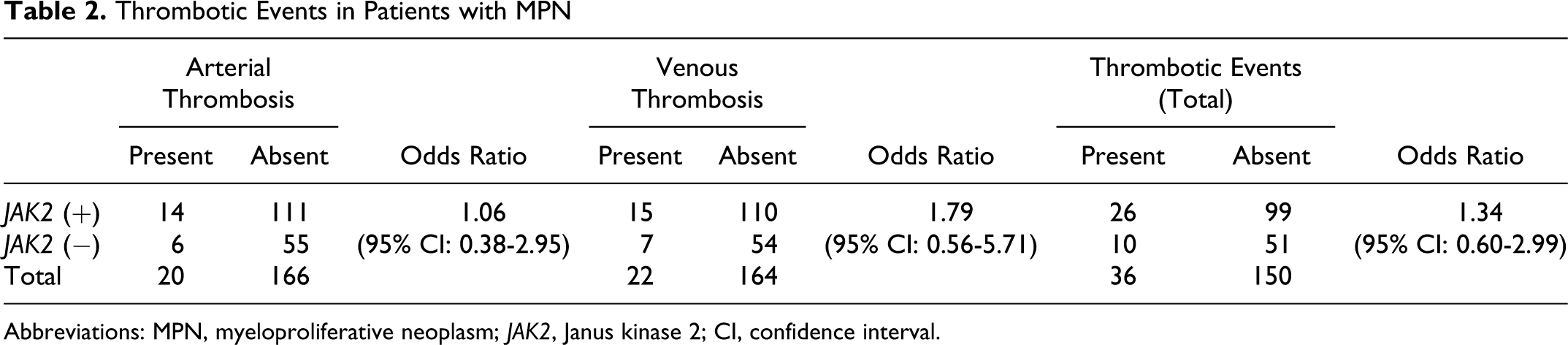
Abbreviations: MPN, myeloproliferative neoplasm; JAK2, Janus kinase 2; CI, confidence interval.
Irrespective of the JAK2 V617F mutational status, patients with arterial thrombosis including cerebral events were significantly older than those without thrombosis (P < .001). The frequency of venous thrombotic events, on the contrary, did not seem to be significantly influenced by age (P = .311) although the median age was slightly higher in patients with venous thrombosis harboring the JAK2 V617F mutation (Table 3 ).
Median Age (Years) at the Time of First Thrombotic Event in Patients with MPN

Abbreviation: JAK2, Janus kinase 2.
Eighteen patients with PV and one patient with ET carried JAK2 V617F mutation in homozygous state (17% and 2%, respectively). Homozygosity of JAK2 V617F mutation was not found to be associated with increased frequency of thrombosis (P = .884) in patients with PV.
Discussion
The current study clearly demonstrates that the JAK2 V617F mutation is prevalent in neither BS nor BS-associated thrombosis. Thrombosis is usually observed in about one third of the patients with BS. 15 Endothelial cell damage and activation of leucocytes, platelets, as well as the coagulation system have been accused to lead to thrombosis in BS. 20–26 Thrombotic complications in BS usually involve venous system and present as deep vein thrombosis of the lower extremities and/or superficial thrombophlebitis in most of the cases. 16 Although much more rare than in MPNs, SVT is also observed in patients with BS. 39
Although thrombosis in BS is mainly attributed to vascular inflammation and endothelial damage, the role of thrombophilia in creating a tendency for thrombosis is also frequently considered. Several studies have been published on the frequency of various thrombophilic factors among patients with BS with thrombosis, with conflicting results. 27–34 Some studies showed an increased risk of thrombosis associated with factors such as increased thrombin activatable fibrinolysis inhibitor levels 25 or activated protein C levels, 32 while others failed to show such associations. 30–31 A recent meta-analysis showed that hyperhomocysteinemia may be associated with thrombosis in patients with BS, 29 whereas another study proposed an association between factor V Leiden (FVL) and prothrombin mutations and thrombosis in BS. 34
Similar to BS, thrombotic manifestations are observed in about 10% to 30% of patients with myeloproliferative disorders. 4 Thrombosis, in fact, is the most important cause of morbidity and mortality in MPNs, particularly in PV and ET. 4,40 It usually prefers veins more than arteries. Localization of venous thrombosis is unusual with a high frequency of splanchnic vein involvement. 41
In our cohort of patients with MPNs, 9 of the 22 venous thrombotic events (41% of venous thrombosis and 21% of all thrombotic events) were observed in the splanchnic veins. Of these 9 (7 PV and 2 ET) patients, 8 (88%) were carriers of JAK2 V617F mutation. Increased frequency of intra-abdominal vein thrombosis in MPNs can partially be explained by impaired blood flow and pooling of blood in splanchnic area due to splenomegaly. Impaired rheological and hemostatic functions seem to set up the scene for increased thrombotic risk. 5,7,8 Whether the presence of JAK2 V617F mutation directly triggers the events leading to thrombosis or induces indirectly a thrombotic background via MPNs is still unclear. Dentali et al 42 has recently reported that about 50% of patients without MPNs presenting with SVT were JAK2 V617F -positive. More than half of these patients developed signs of MPN, subsequently. This suggests that JAK2 V617F positive mutation might have a direct role in the development of SVT through some yet unexplained mechanism. Although in our study, JAK2 V617F positivity among patients with SVT was higher than in patients with venous thrombosis at other sites (8 of 9 vs 7 of 13), we could not demonstrate a significant difference (P = .17).
Cerebral venous thrombosis (CVT) is another rare but typical clinical manifestation associated with MPNs and BS. 43,44 The frequency of CVT has been found to be 1% and 7.8% in large series of patients with ET and BS, respectively. 44,45 In our study, CVT was detected in 2 patients with BS and 1 patient with ET. They all were JAK2 V617F negative.
Ischemic CVEs have also been frequently observed in patients with MPNs. 46 Their association with JAK2 V617F mutation is another issue of discussion. In our cohort, 7 of the 10 patients with ischemic CVEs carried the JAK2 V617F mutation. The frequency was not significantly different among patients with arterial thrombosis at other sites (P = .62). The carriers were mainly male patients with PV (6 PV and 1 ET). We could not explain the occurrence of ischemic CVEs with the presence of JAK2 V617F mutation alone since most of these patients were of older age (median 68 years) and had comorbidities predisposing them to ischemic events (hypercholesterolemia, n = 8; arterial hypertension, n = 6; diabetes mellitus, n = 2; and coronary artery disease, n = 2). Interestingly, Zerjavic et al asserted having found a significant association between ischemic stroke and JAK2 V617F mutation in patients without MPNs. 47
Arterial thrombosis including CVEs was diagnosed in 20 (11%) of our patients with MPN. Recently, 3 large meta-analyses showed evidence for increased risk of arterial thrombosis in patients with JAK2 V617F-positive ET (OR, 1.68-2.09). 48–50 In contrast to current literature, we could not demonstrate a significantly elevated risk for arterial thrombotic events in patients with MPNs carrying the JAK2 V617F mutation. This may result from the relatively low number of patients with ET within the study population. Retrospective design of the study should also be considered as a limitation.
Despite existing controversial results mentioned above, there is some clinical evidence to suggest that the JAK2 V617F mutation may be variably associated with thrombosis. JAK2 V617F mutation has been reported by Pardanani et al 51 in 4 of the 210 patients with deep vein thrombosis and/or pulmonary embolism and in 1 of 8 patients with cerebral vein thrombosis. None of the patients harboring JAK2 V617F mutation met the diagnostic criteria for MPNs. This suggests that JAK2 V617F mutation may, albeit rarely, be associated with thrombosis with no other clinical associations or may accompany thrombosis-related clinical entities other than MPNs. However, subsequent studies among patients with idiopathic venous thromboembolism (VTE) could not demonstrate any convincing results to designate JAK2 V617F mutation as an independent risk factor for thrombosis. 52,53 Therefore, screening for JAK2 V617F mutation in idiopathic thrombotic events is currently not recommended in the absence of findings associated with overt or latent MPN. 54 The significance of JAK2 V617F mutation in other thrombosis prone clinical entities is yet to be determined.
A number of studies indicated that JAK2 V617F mutation is absent in healthy control groups as we observed in this study. 55,56 Although speculative, it is interesting to note that acquired mutations like JAK2 V617F, rarely occur in healthy participants. They seem to be almost always associated with certain clinical conditions. Hereditary mutations, on the other hand, are frequently observed in healthy populations without always causing disease; as it is the case with FVL. The prevalence of FVL in normal Turkish population is about 8%. 57 It has been stated that up to 50% of FVL carriers experience VTE during their lifetime, if they were born to symptomatic families. 58 Accordingly, the presence of FVL does not result in thromboembolic events in more than half of the carriers.
In conclusion, our findings suggest that there is no evidence for JAK2 V617F mutation occurrence among healthy participants and patients with BS. In fact, no clinical condition other than MPNs has been identified so far to be strongly associated with JAK2 V617F. The only clinical entity reported to be associated with increased frequency of JAK2 V617F mutation in the absence of MPNs seems to be the “unprovoked” SVT. 41,59 We found that JAK2 V617F mutation was frequent in patients with MPN associated SVT and CVEs. But this occurred probably as a result of the relatively higher number of JAK2 V617F-positive patients in our cohort. In contrast to most of the current literature, 48–50,54 we could not demonstrate a statistically significant difference in the frequency of thrombotic events among patients with MPN with and without JAK2 V617F mutation. We, therefore, speculate that the thrombogenicity observed in MPNs is multifactorial and does not solely depend on JAK2 V617F positivity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was partially funded by the unrestricted grants of Eczacıbaşı-Baxter Hospital Supply Inc. and Berk İlaç A.Ş.