
Abstract
We describe a case of a 41-year-old woman who was stable for over a year on 22.5 mg/week of warfarin. At a follow-up visit, her international normalized ratio (INR) was found to be supratherapeutic at 3.9. Her only significant change was acyclovir initiation for shingles, and clindamycin and dapsone for infection on her right foot. An interaction report was run using Micromedex with no interactions reported. Sixteen percent of the weekly dose was held and maintenance dose was continued. Two weeks later, the INR remained supratherapeutic at 4.3, with discontinuation of clindamycin and dapsone, 5 days earlier, as the only change. This time an interaction report was run using Lexi-Comp, which identified an interaction between warfarin and dapsone. The INR has been therapeutic and stable since discontinuation of transient factors. It is hypothesized that warfarin and dapsone compete for binding on the CYP2C9 and CYP3A4 isoenzymes and therefore serum concentration of warfarin was elevated.
Keywords
Introduction
Warfarin is used as the oral anticoagulant of choice to prevent thrombotic events in patients with recent orthopedic surgery, a history of venous thromboembolism, atrial fibrillation, and prosthetic heart valves. 1 It works by inhibiting vitamin K used for the activation of clotting factors II, VII, IX, and X. 1 While the efficacy of warfarin on anticoagulation is well established, it is also challenging to use due to its narrow therapeutic window, variability in dose response among patients, and the multitude of food and drug interactions that exists. 1 Because of these characteristics, the safety and efficacy of warfarin must be monitored by the international normalized ratio (INR) continuously.
Warfarin’s chemical makeup and its metabolism are key elements in its extensive interaction profile. Warfarin is a racemic mixture of R- and S-enantiomers, and the S-enantiomer is 2 to 5 times more potent than its R-counterpart. 2 The S-form of warfarin is metabolized by CYP2C9, while the R-form is metabolized by CYP1A2 and CYP3A4.2,3 Since the S-enantiomer is much more potent, concomitant drugs that utilize the CYP2C9 isoenzyme for metabolism will have a much greater effect on INR. Drug interactions with warfarin are most commonly attributed to inhibition or induction of CYP450 isoenzymes.
We describe a scenario where a patient possibly had an interaction between dapsone and warfarin, which resulted in a supratherapeutic INR.
Case Report
A 41-year-old African American woman is receiving warfarin for recurrent deep vein thrombosis (DVT) and pulmonary embolus (PE). On a routine follow-up visit on September 28, 2010, the patient experienced an increase in her INR without any adjustments in warfarin dosage or changes in her maintenance medications. She also reported resumption of her normal dietary vitamin K intake as intended and discussed at her previous visit. In addition, she denied drinking alcohol, smoking, or taking recreational drugs. Her past medical history is significant for systemic lupus erythematosus, arthritis, fatty liver disease, sinus tachycardia, recurrent nephrolithiasis, overactive bladder, and osteopenia. Her daily drug therapy consists of hydroxychloroquine 200 mg, prednisone 10 mg, gabapentin 300 mg, nifedipine XL 60 mg, trospium XR 60 mg, solifenacin 5 mg, omeprazole 40 mg twice daily, calcium–vitamin D 4 times daily, oxycodone/acetaminophen 10/325 mg twice daily, and tramadol/acetaminophen 37.5/325 mg every 4 to 6 hours as needed for pain. She is also taking daily docusate sodium 100 mg, folic acid 1 mg, ferrous sulfate, and a multivitamin. The patient had been on these drugs for more than 5 months with no changes in dose or frequency of use, therefore any potential drug interactions between these maintenance medications were already accounted for. The patient’s warfarin dosage had been stable on her current dose of 22.5 mg/week since July 2009. Monthly INR results since April 2010 has been 2.1, 1.9, 2.3, 2.1, 2.4, and 1.8, with a target range of 2.0 to 3.0 (Table 1).
Anticoagulation Management
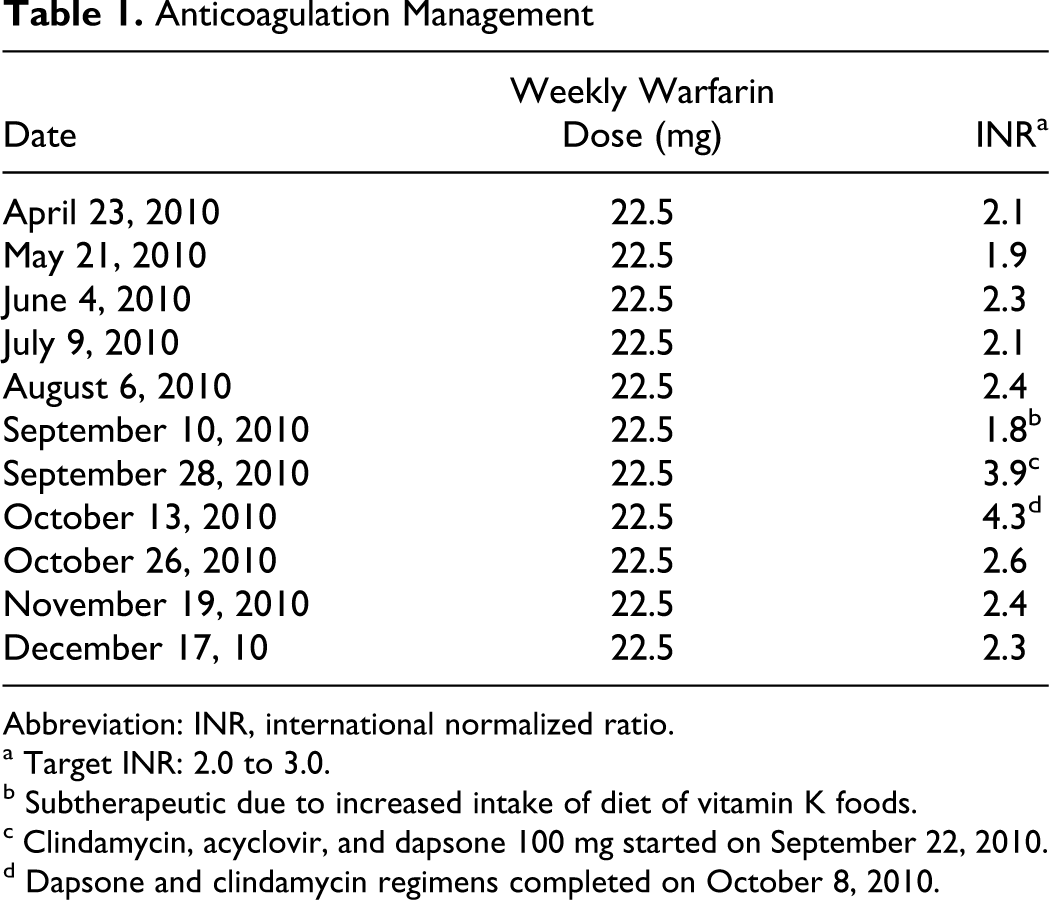
Abbreviation: INR, international normalized ratio.
a Target INR: 2.0 to 3.0.
b Subtherapeutic due to increased intake of diet of vitamin K foods.
c Clindamycin, acyclovir, and dapsone 100 mg started on September 22, 2010.
d Dapsone and clindamycin regimens completed on October 8, 2010.
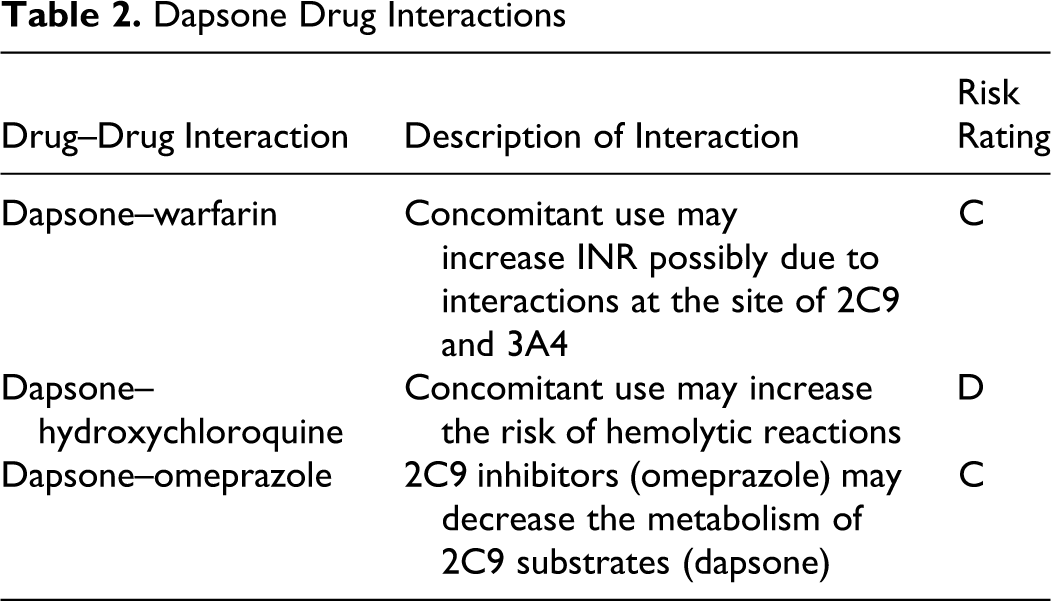
Five days prior to this follow-up visit on September 28th, the patient was started on a 10-day regimen of acyclovir for shingles and 14-day regimen of clindamycin and dapsone 100 mg for a large area of infection on the anterior of her foot secondary to a shingles blister. We performed an interaction report using Micromedex and inputting all 18 medications. There were no interactions found between the maintenance medications and the newly initiated, acyclovir, clindamycin, or dapsone. Given that she was previously therapeutic and stable on her dose, we held, approximately 16% of her weekly dose, and continued with her normal warfarin regimen of 22.5 mg/week. On the patient’s next office visit on October 13th, 2 weeks later, her INR was still supratherapeutic at 4.3. Once again, all other potential influencing factors were unchanged. She had completed her 14-day therapy of clindamycin and dapsone 5 days earlier. An interaction report for all drugs was run again using Lexi-Comp this time, and a drug interaction with dapsone was noted for warfarin, hydroxychloroquine, and omeprazole (Table 2). No drug interactions were found with clindamycin. Since the half-life of dapsone is 30 hours, it was likely the patient’s INR was trending downward. However, it was appropriate to hold 2 doses of her warfarin, approximately 27% of her weekly dose, and resume with 22.5 mg/week. Two weeks later on October 26th the patient returned for a follow-up visit and her INR had returned to therapeutic range at 2.6 and has remained therapeutic since then (Table 1).
Dapsone Drug Interactions
Discussion
According to the Naranjo Adverse Drug Reaction Probability Scale and the Drug Interaction Probability Scale (DIPS), our patient’s supratherapeutic INR is considered probably related to a warfarin and dapsone interaction.4,5 The patient’s INR was stable for several months prior to dapsone initiation, and she is historically very methodical at keeping potential influencing factors consistent. There were no other explanations for the increased INR, and her INR returned to therapeutic range on her normal maintenance dose after discontinuation of dapsone and has remained therapeutic since then.
Dapsone is a miscellaneous antibiotic used in the treatment of leprosy, dermititis herpetiformis, and the prevention and treatment of pneumonia caused by Pneumocystis jiroveci. 6 Several studies demonstrate that dapsone is converted into its active metabolite through multiple cytochrome p450 enzymes, including CYP3A4, CYP2C9, and CYP2E1. 7 Since both dapsone and warfarin are major substrates of CYP2C9 and CYP3A4, we hypothesize that an interaction may exist due to these 2 drugs competing for the same binding site. Of highest concern is the competition for the CYP2C9 isoenzyme since it is responsible for the metabolism of S-warfarin, the more potent form of warfarin. In this particular case, dapsone may have potentiated the effects of warfarin and increased INR.
The Medline database was searched to confirm our hypothesis and identify previous reports of interactions between warfarin and dapsone. Despite an exhaustive search, we were unable to find any such reports. Two noteworthy interactions with dapsone were found that may further support the interaction between dapsone and warfarin. Reportedly, concurrent use 8 of rifampin decreases the serum concentration of dapsone by 22% to 83%, while dapsone concentration is increased by approximately 40% when used with trimethoprim. 9 Warfarin concentration, when used concomitantly with rifampin and trimethoprim, is known to react similarly. Unfortunately, with no current evidence to confirm an existing interaction between warfarin and dapsone, it is difficult to be certain that dapsone was the cause for the supratherapeutic readings in this patient case. However, these hypotheses are presented as possible explanations for a potential interaction between these 2 drugs.
Although it is believed that the increase in INR was due to a drug interaction between warfarin and dapsone, alternative possibilities should also be discussed as well as the other 2 drug interactions found with dapsone (Table 2). The potential interaction between dapsone and hydroxychloroquine may increase the risk of bleeding, but would not likely affect INR because it does not affect the pharmacokinetics of warfarin nor does it affect vitamin K concentrations. The potential dapsone and omeprazole interaction would result in an increased concentration of dapsone and as hypothesized, would consequently increase competition with warfarin for the binding site of the CYP2C9 and CYP3A4 isoenzymes. As for alternative possibilities for increase in INR, it is possible that clindamycin decreased vitamin K-producing flora in the intestine which would increase INR. 10 However, this typically results only if clindamycin has caused diarrhea. Another possible cause of elevated INR is the potential for shingles and/or cellulitis of the foot to cause fever which would increase the catabolism of vitamin K and thereby increase INR. 1 Although these are possibilities, the patient denied illness and side effects while taking these new medications.
An additional item to note is the inconsistency in evidence found among several reputable drug databases. Three databases were used to identify drug interactions. Micromedex revealed no interactions with warfarin and did not mention the metabolism of dapsone through the CYP450 system. Epocrates provided information that dapsone is metabolized by CYP2C9 and CYP3A but showed no interaction with warfarin using its interaction finder. Finally, Lexi-Comp indicated that there was a moderate interaction between the 2 drugs, and stated it was possibly related to the effects of CYP2C9 and CYP3A isoenzymes. Further evidence is needed to confirm or refute this interaction so that information provided by these reliable sources may be congruent and pertinent interactions are not missed.
Conclusion
Warfarin is the most widely used anticoagulant in the prevention and treatment of thromboembolism. To our knowledge, this is the first case report of an interaction between warfarin and dapsone. According to the Naranjo and the DIPS adverse drug reaction probability scale, this interaction was probably related. This case report reiterates the importance of monitoring warfarin patients closely when new antibiotics are started, and using 2 reliable drug resources to check for interactions. This case report supports the need for further studies exploring the relationship between warfarin and dapsone interactions and CYP450 enzymes responsible for the metabolism of dapsone. Patients currently on warfarin, and starting treatment with dapsone, should be followed closely to ensure they remain within therapeutic range and prevent complications.
Footnotes
The work presented in this article has not been presented at any professional meeting.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.