
Abstract
We have utilized high-dose factor VIII (FVIII) concentrates in 4 hemophilia A patients with inhibitors prior to surgery for the insertion of a central venous access device. In total, 3 patients out of 4 had high responding inhibitors. Dosing algorithms for this type of therapy have not been previously validated and established. We devised an effective formula to calculate the initial dose required to neutralize the inhibitors, although some of the patients demonstrated a lower recovery of FVIII than expected. An anamnestic inhibitor response was evident in 3 cases, but overall our strategy provided a reliable hemostatic effect for at least 4 days after surgery. In addition, our protocol appeared to be more cost-effective than FVIII bypass therapy. The financial saving in 1 case for the initial 3 days was estimated to be approximately US$49 122. Our results demonstrated that high-dose FVIII therapy provided clinically effective and economically viable results even in high responders.
Introduction
Hemophilia A is the most common X-linked hereditary hemorrhagic disorder and is caused by a deficiency or functional abnormality of blood clotting factor VIII (FVIII). Bleeding episodes are commonly treated by infusions of plasma-derived FVIII (pdFVIII) concentrates or recombinant FVIII (rFVIII) concentrates. Factor VIII inhibitors arise as alloantibodies against infused, extrinsic FVIII in 15% to 30% of patients with hemophilia A. 1 In these instances, the hemostatic efficiency of infused FVIII is seriously impaired, and the development of alloantibodies, therefore, represents a serious therapeutic complication in such patients. Patients with FVIII inhibitors can be classified into 2 subgroups, high and low responders. High responders have inhibitor levels of >5 BU/mL and exhibit a brisk antibody response following FVIII exposure. The inhibitor titer in these cases usually increases sharply 5 to 7 days after an infusion of FVIII, and this phenomenon is believed to be an anamnestic response. Low responders have inhibitor levels of <5 BU/mL and do not develop an anamnestic response following exposure to FVIII.2,3 Factor VIII-bypassing agents such as activated prothrombin complex concentrates (aPCC) and recombinant activated factor VIIa (rFVIIa) are commonly used for the treatment of hemarthroses in high responders. Inhibitor titers do not remain constant in patients with hemophilia A, however, and after long-term absence of a FVIII antigenic stimulus, inhibitor titers often decrease to the levels where high-dose FVIII concentrate therapy may be used even in high responders. In this study, we utilized high-dose FVIII concentrates in 4 hemophilia A patients with inhibitors prior to surgery for the insertion of a central venous access device (CVAD). All patients were considered suitable for immune tolerance induction (ITI) therapy through the implanted device. There appears to be few reports in which practical strategies for the use of high-dose FVIII concentrates in high responders have been described. We demonstrated that the neutralization of high-responding inhibitors can be hemostatically effective. We described retrospective case reports of surgery performed in these patients between 2006 and 2010.
Materials and Methods
Patient Profiles
All patients had severe hemophilia A with inhibitors (FVIII coagulant activity [FVIII:C], <1%) and were considered suitable for ITI. In each case, however, the current venous access was believed to be too challenging for the necessary frequent infusions, and CVAD placement was planned to facilitate the program. The clinical and laboratory profiles of these patients are summarized in Table 1.
Profiles of 4 Hemophilia A Patients With Inhibitor and Infused Doses of FVIII Concentrate a
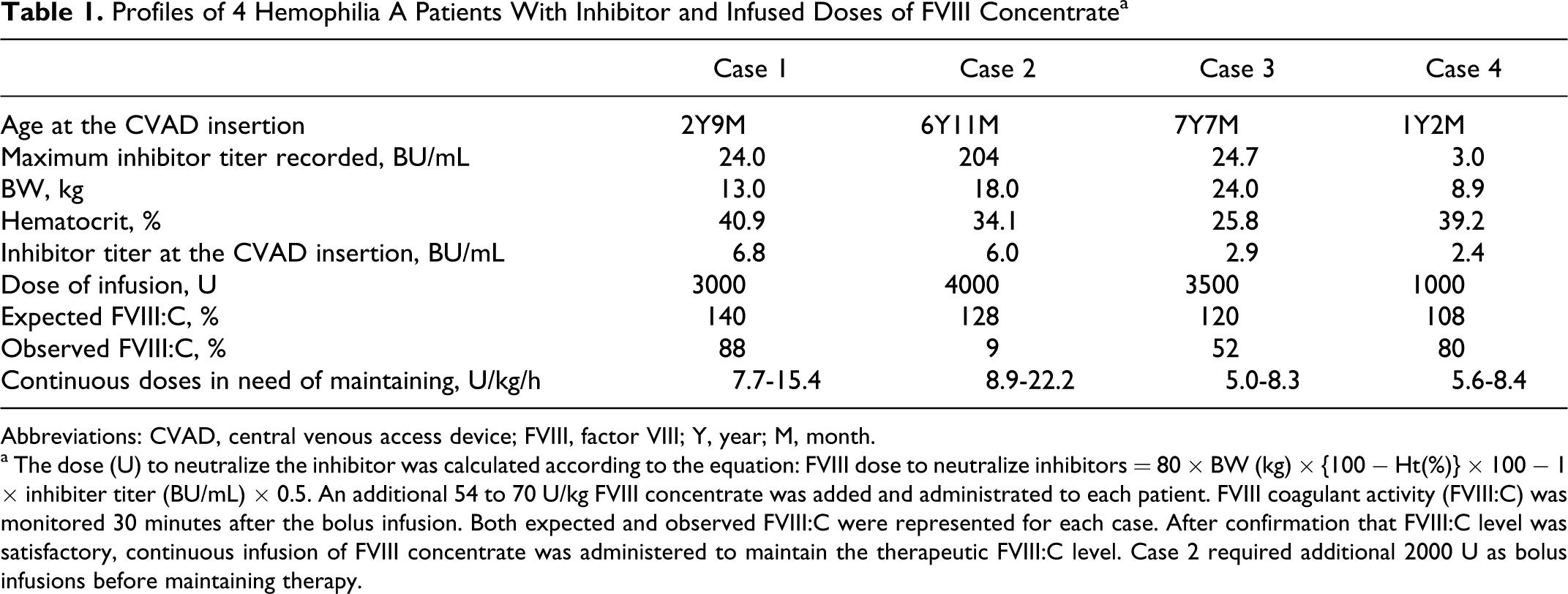
Abbreviations: CVAD, central venous access device; FVIII, factor VIII; Y, year; M, month.
a The dose (U) to neutralize the inhibitor was calculated according to the equation: FVIII dose to neutralize inhibitors = 80 × BW (kg) × {100 − Ht(%)} × 100 − 1 × inhibiter titer (BU/mL) × 0.5. An additional 54 to 70 U/kg FVIII concentrate was added and administrated to each patient. FVIII coagulant activity (FVIII:C) was monitored 30 minutes after the bolus infusion. Both expected and observed FVIII:C were represented for each case. After confirmation that FVIII:C level was satisfactory, continuous infusion of FVIII concentrate was administered to maintain the therapeutic FVIII:C level. Case 2 required additional 2000 U as bolus infusions before maintaining therapy.
Case 1: Patient was 2 years old and was diagnosed at the age of 3 months. Subsequently, he was treated with pdFVIII on demand for recurrent hemorrhagic episodes. At the age of 15 months, a FVIII inhibitor was detected (1.0 BU/mL). Since then he has had repeated muscle and joint bleeding, and although he has been treated with FVIII-bypassing agents, he developed progressive hemophilic arthropathy. The maximum inhibitor titer recorded (highest inhibitor level since diagnosis) was 24 BU/mL which decreased to 6.8 BU/mL at the time of surgery.
Case 2: Patient was 6 years old. He was diagnosed at the age of 5 months. At the age of 10 months, he was admitted with an intractable hemorrhage in the scrotal sack, and a FVIII inhibitor (80 BU/mL) was detected. Since then he has had repeated muscle and joint bleeding, and although he has been treated with bypassing agents, both knee joints have been destroyed. He has difficulty in walking unaided and is usually confined to a wheelchair. The maximum inhibitor titer recorded was 204 BU/mL which decreased to 6.0 BU/mL at the time of surgery.
Case 3: Patient was 7 years old. He was the younger brother of case 2 and was diagnosed at the age of 1 month. At the age of 1 year, a FVIII inhibitor was detected. As with his older brother, he has been treated with bypassing agents but has had repeated muscle and joint bleeding and developed progressive hemophilic arthropathy. The maximum inhibitor titer was 24.7 BU/mL, which decreased to 2.9 BU/mL at the time of surgery.
Case 4: Patient was 1 year old and was diagnosed at the age of 2 months. At the age of 9 months, a FVIII inhibitor (1.0 BU/mL) was detected. His family requested ITI instead of using bypassing agents to prevent serious joint deterioration. Difficulties with venous access prompted us to consider the insertion of a CVAD. The maximum inhibitor titer was 3.0 BU/mL which decreased to 2.4 BU/mL at the time of surgery.
Protocol
All therapy was conducted after obtaining fully informed consent. Before the start of surgery, in each case sufficient high-dose FVIII concentrate was administrated to overcome the circulating inhibitor. Previous dosing algorithms for this type of procedure have little scientific basis, however, and have not been validated 2 ; and in the absence of a rational and validated approach, we devised the following formula to estimate the amount of FVIII required to neutralize the inhibitors. FVIII dose = 80 × body weight BW (kg) × {100 − Ht(%)} × 100–1 × inhibiter titer (BU/mL) × 0.5, where the calculations incorporating the body weight (BW) in kilogram and the hematocrit (Ht%) provided an estimate of the circulating plasma volume (mL). An additional 50 U/kg FVIII concentrate was added to obtain the therapeutic dose, and the resulting circulating FVIII:C was expected to be 100% (1.0 U/mL). After confirmation that the FVIII:C level was satisfactory, continuous infusion of FVIII concentrate was administered to maintain therapeutic levels. FVIII:C was monitored during continuous infusion, with target levels of FVIII:C above 50% (0.5 U/mL) for 2 days after the surgery, and above 20% (0.2 U/mL) for a further 3 to 5 days. Immune tolerance induction therapy was commenced 7 to 10 days later using 50 U/kg FVIII concentrate 3 times a week administered through the implanted devices. Standard, 5F port catheters (Anthron P-U Catheter, TORAY Medical Co Ltd, Tokyo, Japan) were utilized as CVADs in all cases. The devices consisted of a subcutaneous reservoir with a self-sealing silicone septum coupled to a radiopaque silicone catheter. They were implanted as generally accepted in the upper anterior chest wall with the catheter fed via the jugular venous system into the superior vena cava (SVC) such that the catheter tip was located at or just above the entry of the SVC into the right atrium. Port access was gained using a specialized noncoring percutaneous needle (Huber needle, B. Braun Medical Inc, Bethlehem, Pennsylvania). 4
Factor VIII Assays
FVIII:C was measured using 1-stage procoagulant assays as described previously. 5 Factor VIII inhibitor assays were performed using the Bethesda method. 6
Results
The doses of FVIII concentrate administrated and FVIII:C recovery are summarized in Table 1. The clinical course in each case is shown in Figures 1 to 4, respectively.
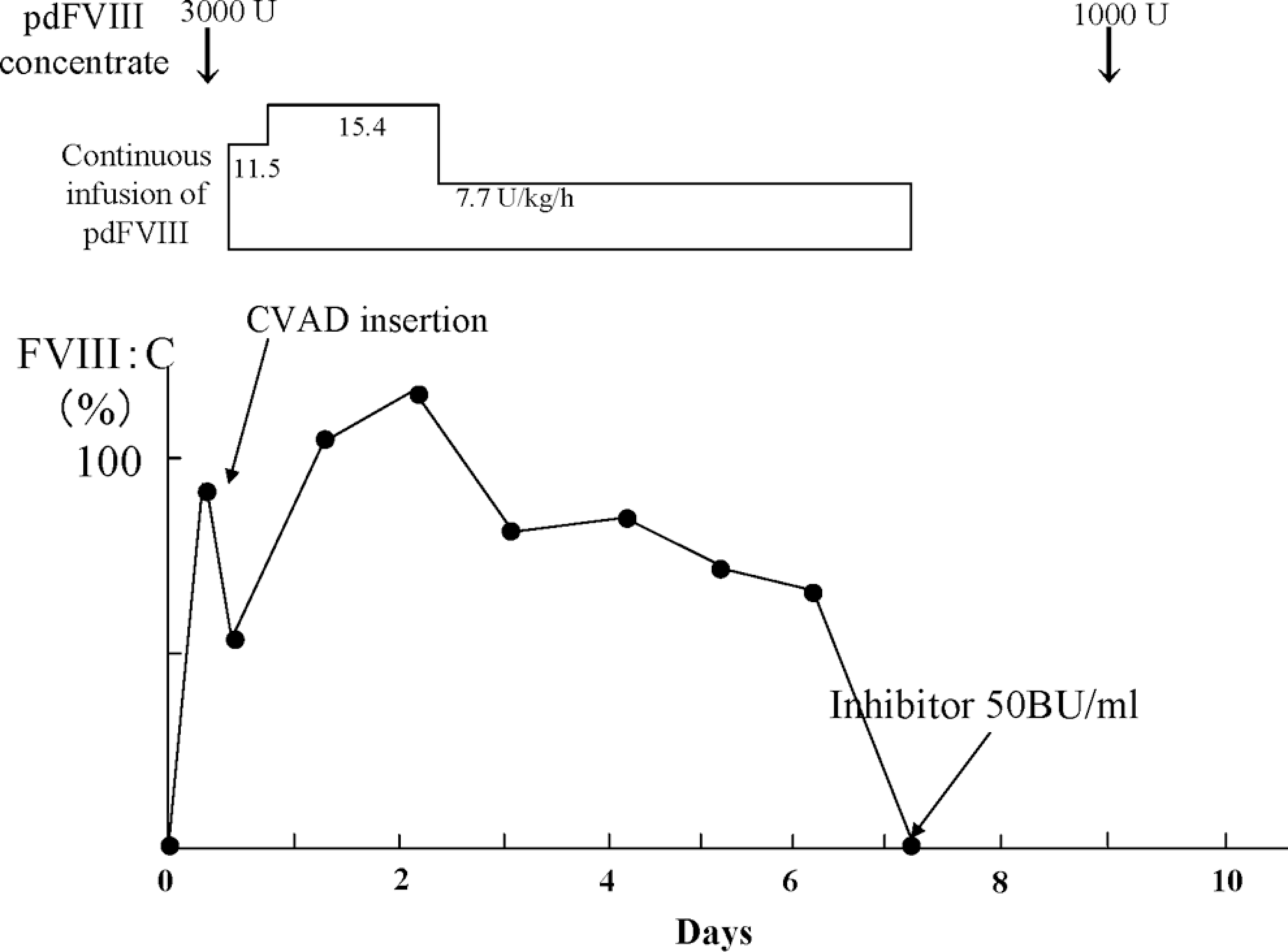
Clinical course of case 1. The FVIII:C after the infusion of 3000 U pdFVIII was 88% (expected 140%). Subsequently, continuous infusion of FVIII concentrate was administered. The patient required the dose of 7.7 to 15.4 U/kg per h to maintain the target levels of circulating FVIII:C. Seven days later, the inhibitor level was elevated to 50 BU/mL. pdFVIII indicates plasma-derived factor VIII; FVIII:C, FVIII coagulant activity.
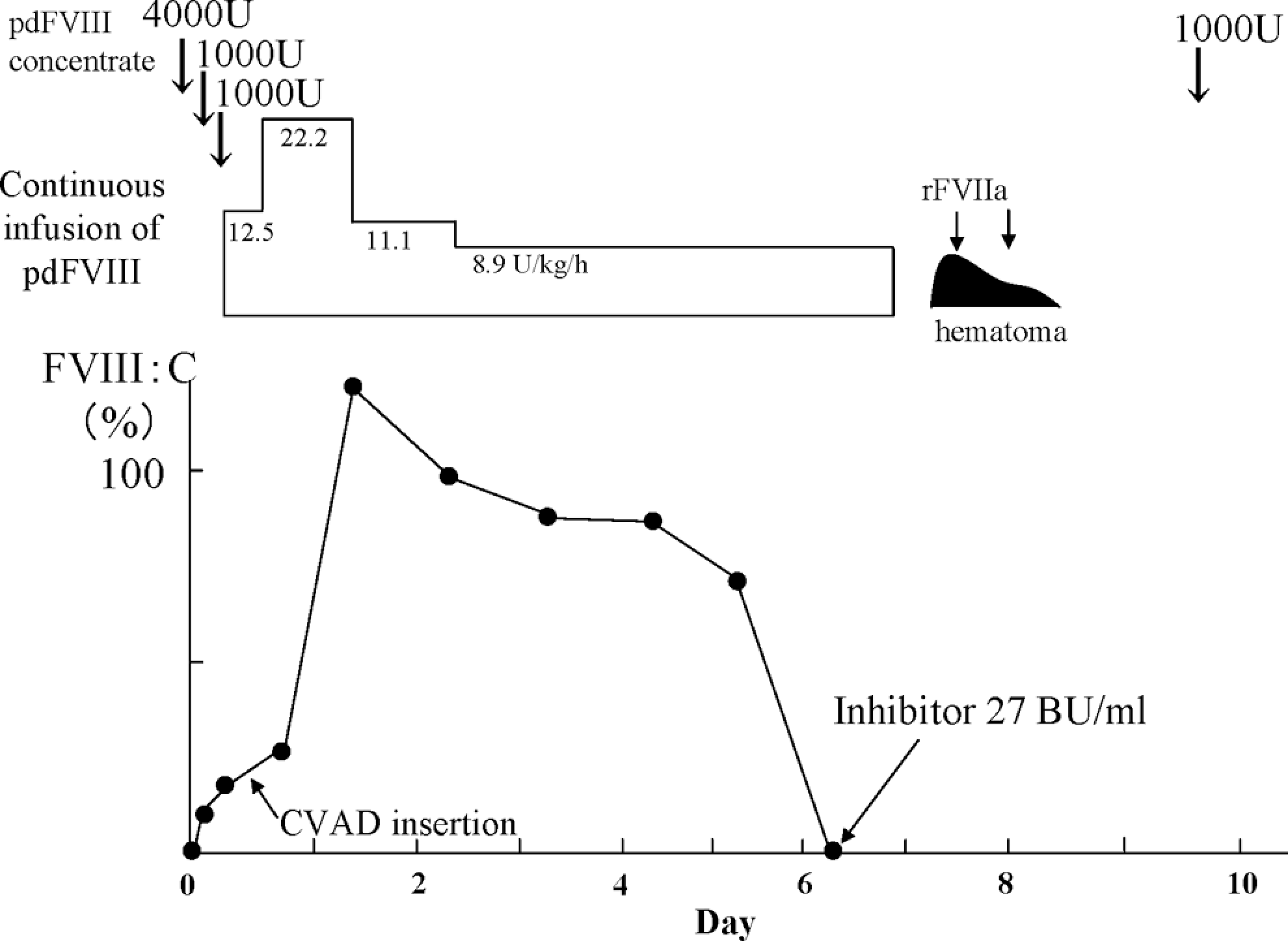
Clinical course of case 2. The FVIII:C in case 2 after the infusion of 3000 U pdFVIII was only 9.4% (expected 128%). An additional 1000 U pdFVIII raised the FVIII:C to 16%. A further 1000 U pdFVIII was given and surgery performed immediately. The operation was completed without untoward bleeding. Subsequently, continuous infusion of pdFVIII was administered. The patient required the higher doses of FVIII (8.9-22.2 U/kg per h) than anticipated to maintain the therapeutic level of FVIII:C. Six days after surgery, a circulating inhibitor was detected at a titer of 27 BU/mL in the absence of FVIII:C. pdFVIII indicates plasma-derived factor VIII; FVIII:C, FVIII coagulant activity.
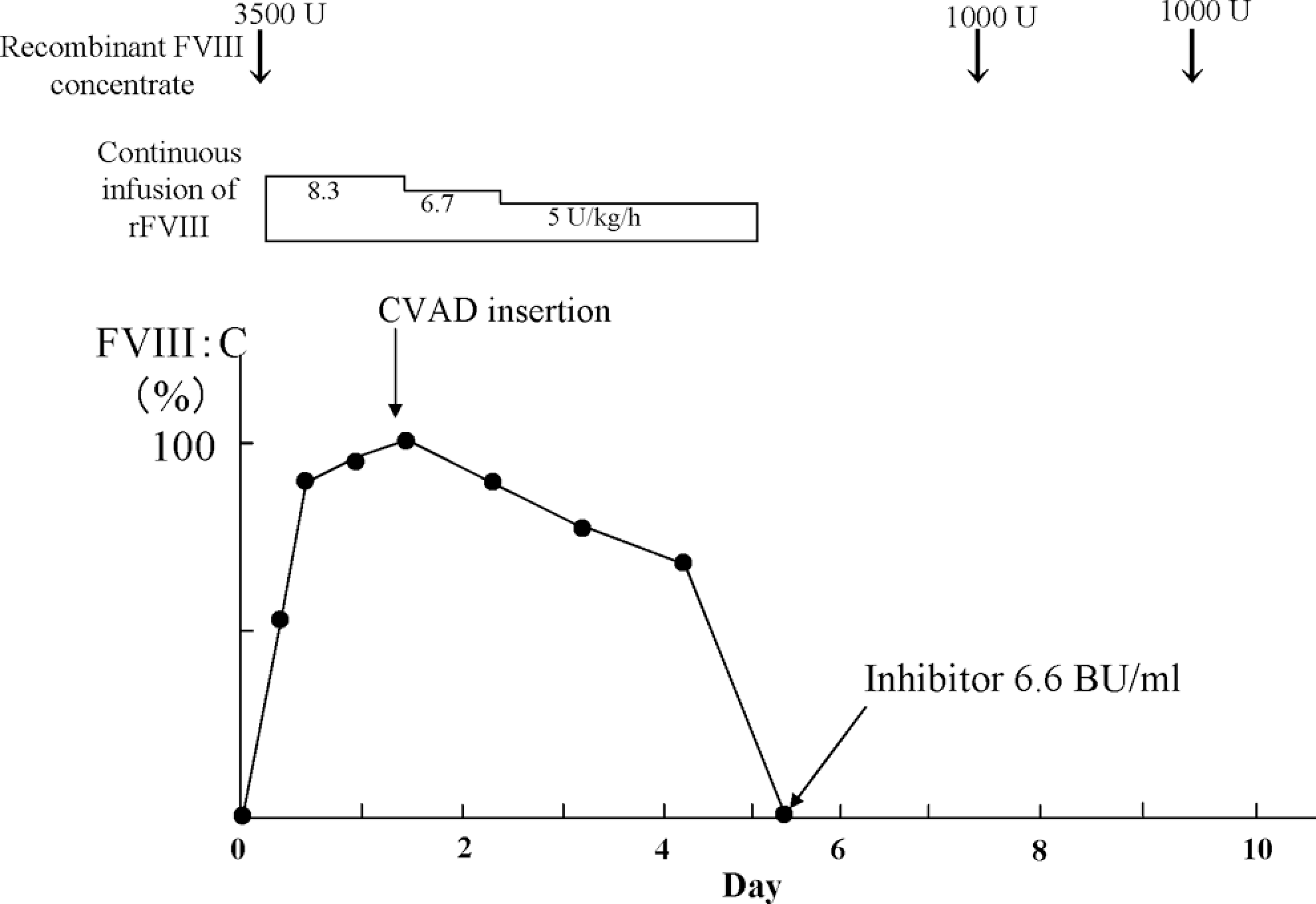
Clinical course of case 3.
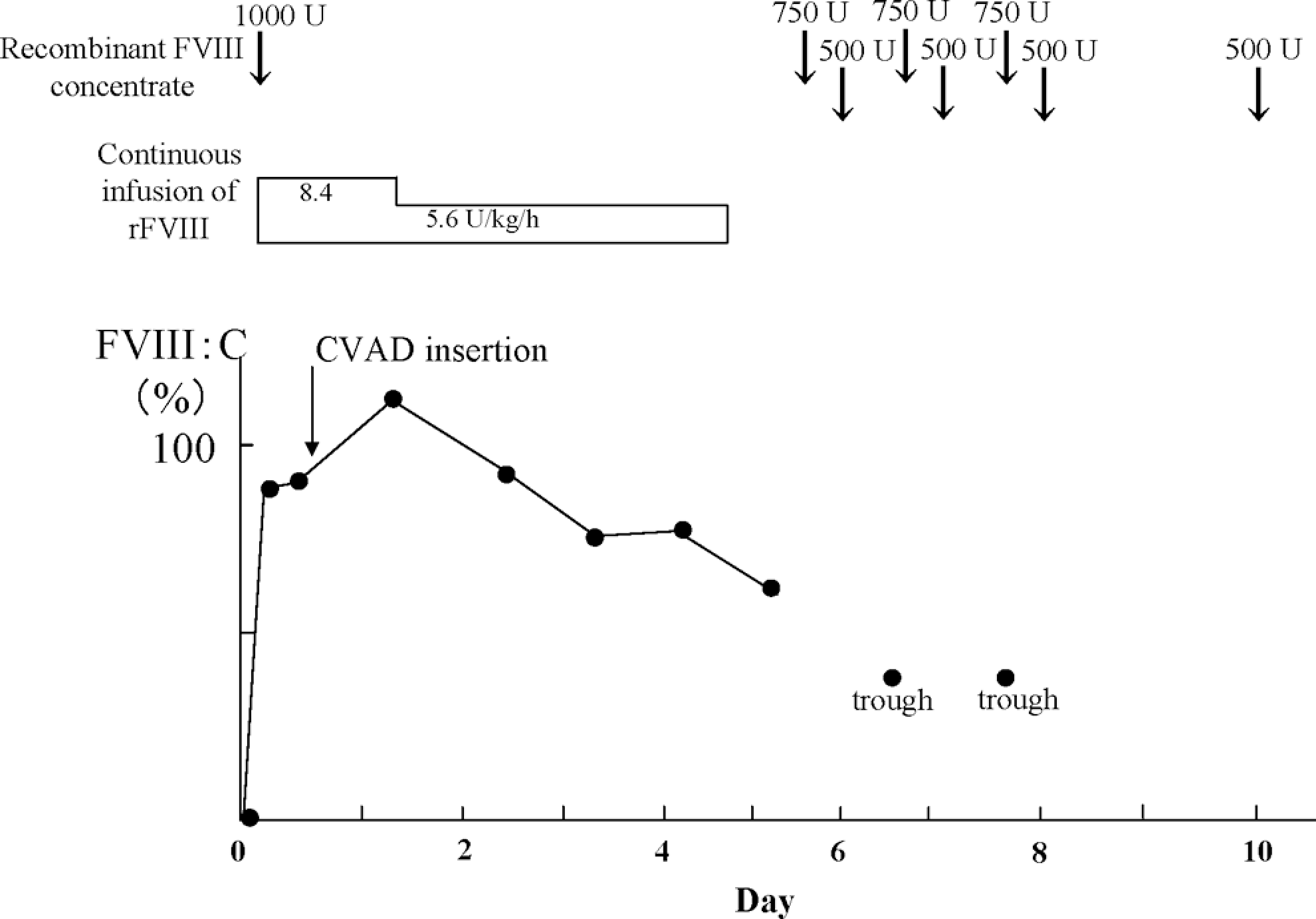
Clinical course of case 4.
The plasma level of FVIII:C in case 1 after the infusion of 3000 U pdFVIII (Cross-Eight M, The Japanese Red Cross, Chitose, Japan) was 88% (expected 140%). Subsequently, continuous infusion of FVIII concentrate was administered at a dose of 7.7 to 15.4 U/kg per h to maintain the target levels of circulating FVIII:C. Surgery was completed without significant blood loss, and no bleeding was observed after the operation. Seven days later, an anamnestic response stimulated the inhibitor level to 50 BU/mL, and no FVIII:C was present in plasma. The inhibitor level declined after ITI therapy and a normal FVIII half-life and complete disappearance of inhibitor was confirmed 2½ years later. Clinical hemorrhagic events decreased dramatically and the patient has overcome serious joint problems. The CVAD was removed 3 years after the surgery. No complications were observed during the period of the implantation.
In contrast, the plasma level of FVIII:C in case 2 after the infusion of 3000 U pdFVIII (Cross-Eight M) was only 9.4% (expected 128%). An additional 1000 U pdFVIII raised the FVIII:C to 16%. A further 1000 U pdFVIII was given and the surgery was performed immediately. The operation was completed without untoward bleeding. Subsequently, continuous infusion of pdFVIII at a dose of 8.9 to 22.2 U/kg per h was administered to maintain the target levels of FVIII:C. The presence of the latent inhibitor required the use of higher doses of FVIII than anticipated to maintain the therapeutic level of FVIII:C. Six days after surgery, a circulating inhibitor was detected at a titer of 27 BU/mL in the absence of FVIII:C. A hematoma developed around the implanted reservoir 7 days after the surgery but resolved in a few days after treatment with rFVIIa. Subsequently, ITI therapy was attempted for 2 years, and although the inhibitor titer declined to 1.7 BU/mL 60 weeks after surgery, it was later elevated to 103 BU/mL and ITI therapy was discontinued. The patient continues to have repeated joint and muscle hemorrhages.
The plasma level of FVIII:C in case 3 after the infusion of 3500 U rFVIII (Advate, Baxter Healthcare Corporation, Neuchatel, Switzerland) was 52% (expected 120%). The bolus infusion was followed by continuous infusion at a dose of 8.3 U/kg per h and 12 hours later the plasma level of FVIII:C was 90%. Central venous access device insertion was accomplished without significant blood loss. Continuous infusion of rFVIII was administered at a dose of 5 to 8.3 U/kg per h to maintain the target levels of FVIII:C. No intra or postoperative bleeding was observed. An anamnestic response stimulated the inhibitor to 50 BU/mL 5 days after the initiation of high-dose FVIII therapy. Immune tolerance induction therapy has been continued for 1½ years; and although the inhibitor titer reached a peak of 385 BU/mL, it has presently declined to 37 BU/mL.
The plasma level of FVIII:C in case 4 after the infusion of 1000 U rFVIII (Advate) was 80% (expected 109%). The bolus infusion was followed by continuous infusion at a dose of 8.4 U/kg per h. Twelve hours later, the plasma level of FVIII:C was 90%, and the surgery commenced. Central venous access device insertion was completed without significant blood loss. Continuous infusion of rFVIII was administered at a dose of 5.6 to 8.4 U/kg per h to maintain the target levels of FVIII:C. No postoperative bleeding was observed. Ten days after the surgery, the inhibitor titer rose to a maximum of 1.8 BU/mL, consistent with the behavior of a low-responding inhibitor. Immune tolerance induction therapy has been continued for 5 months and the inhibitor titer currently remains at 1.2 BU/mL.
Discussion
High-dose FVIII therapy provided reliable hemostatic control and successfully prevented intra and postoperative hemorrhage in each of the present case, although 3 of the 4 patients had high responding inhibitors. Assessment of the effectiveness of FVIII-bypassing therapy for controlling hemostasis in hemophilia A patients with inhibitors is known to be difficult. Thromboelastgraphy (TEG) 7 and thrombin generation assays (TGT) 8 have been utilized for this purpose, but these techniques are not widely adopted and some of the assay parameters can be difficult to interpret. In addition, long-term use of aPCC or rFVIIa might be refractory in some cases. 9 In contrast, high-dose FVIII therapy appears to be hemostatically effective once the circulating inhibitor is neutralized. In the present study, anamnestic responses were evident in cases 1 to 3, but therapeutic levels of FVIII:C were maintained above 20% for 5 days after commencing high-dose FVIII therapy. After starting the therapy, the time when the antibody response was seen varied between patients (days 7, 6, and 5 in cases 1-3, respectively), indicating that careful monitoring of FVIII:C was indispensable for reliable clinical management.
Importantly, our experience demonstrated that mathematical calculations of the required FVIII dose based on the inhibitor titer and blood volume may not be reliable. In case 2 especially, much more exogenous FVIII was required than calculated in order to neutralize the inhibitor and maintain therapeutic FVIII:C levels. Previous studies have suggested that inhibitors may be contained in the so-called third, extravascular space, including interstitial fluid, lymph nodes, and splenic tissue. 10 Although inhibitors may be present in interstitial fluid in equilibrium with plasma, it is difficult to predict the amount of antibodies in the third space in any individual patient. Our equation, FVIII doses to neutralize inhibitors = (80 × BW (kg) × {100–Ht(%)} × 100–1 × inhibiter titer (BU/mL)] × 0.5), excludes noncirculating inhibitor and might underestimate the required dose in some circumstances. Kasper proposed an alternative equation, {40 × BW (kg) + 20 × BW (kg) × inhibiter titer (BU/mL)}, to determine the initial dose, 11 but using this method in our cases indicated that 2288, 2880, 2352, and 783 U should be used for cases 1, 2, 3, and 4, respectively. These amounts were much lower than those that were eventually required. Furthermore, recalculation 12 using van Leuven’s equation {2 × BW (kg) × inhibiter titer (BU/mL) × 0.8 × {100 − Ht(%)} + 50 × BW (kg)}, overestimated the dose (9009, 12 287, 8038, and 2523 U for cases 1, 2, 3, and 4, respectively). It seems likely, therefore, that no formula can be reliably applied to all cases, although our equation provided the closest estimate to that required in 3 of our patients. Our findings in case 2 also indicated that adequate time should be allowed before surgery to ensure FVIII inhibitor neutralization. Infusions of high doses of FVIII concentrate were commenced 12 hours before the surgery in cases 3 and 4; and in these instances, the inhibitors were neutralized and effective levels of FVIII:C were established. This protocol ensured adequate hemostasis without fear of sudden FVIII loss during the course of surgery.
Our findings do not infer that this type of treatment maximized FVIII recovery or that ITI was successful in all cases, but our data suggest that the strategy of using FVIII concentrate successfully provided a reliable hemostatic effect for at least 4 days after surgery. The hematoma that appeared in case 2 was not unusual and is seen often in patients with hemophilia at the site of the self-sealing silicone septum after establishing port access with a percutaneous needle. The hematoma was not regarded as serious and disappeared quickly after treatment with rFVIIa. Generally, the clearance of FVIII is known to be 2 to 4 mL/kg per h, and infusions of pdFVIII or rFVIII at 3 U/kg per h is usually enough to maintain therapeutic levels in patients without inhibitors. 13 In our cases with inhibitors, especially cases 1 and 2, much higher doses of continuous pdFVIII were required, and although the clearance rates are known to differ between individuals, it seems likely that our results in cases 1 and 2 were associated with inhibitor-mediated enhanced clearance of FVIII. Further studies are required to clarify the effects of inhibitors on clearance of infused FVIII. Nevertheless, overall our results clearly illustrated that plasma FVIII:C should be carefully monitored during and after concentrate infusion so that additional material can be administrated if the therapeutic levels are not adequate.
In general, treatment costs for patients with inhibitors are usually considerably higher than those for patients without inhibitors. 14 The financial implications of high-dose FVIII replacement compared with FVIII-bypassing therapy are represented by case 3 and illustrated in Table 2. Hemostatic control for the initial 3 days after surgery is especially important, and on the basis of current recommendations, 15 rFVIIa (NovoSeven, Novo Nordisk, Bagsvaerd, Denmark) would be given at a dose of 80 to 120 μg/kg every 3 hours for this period. For this reason, therefore, we compared these therapeutic options for this period. Hence, the financial saving in this case for this time would be 4.6 million yen (JPY), approximately US$49 122. Similar economic benefits would be seen in the other 3 cases. The financial savings were calculated to be US$20 988, US$44 357, and US$26 547 in cases 1, 2, and 4, respectively. The data indicate, therefore, that high-dose FVIII therapy could be substantially more cost-effective than bypassing therapy in these circumstances.
Economical Comparison a Between High-Dose FVIII Therapy and FVIIa Bypassing Therapy in Case 3
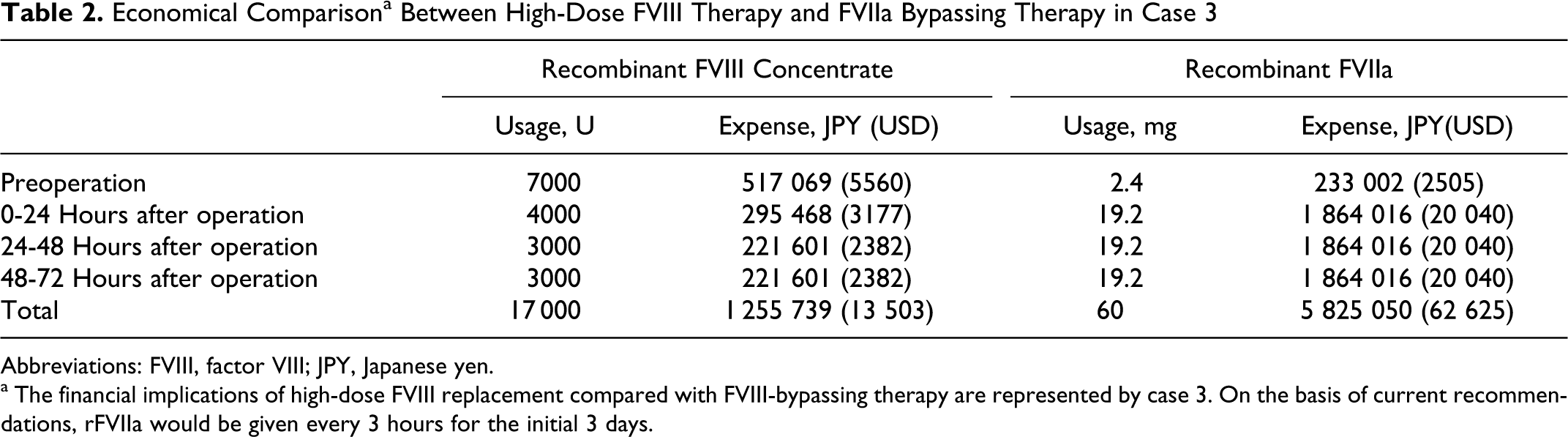
Abbreviations: FVIII, factor VIII; JPY, Japanese yen.
a The financial implications of high-dose FVIII replacement compared with FVIII-bypassing therapy are represented by case 3. On the basis of current recommendations, rFVIIa would be given every 3 hours for the initial 3 days.
With regard to the efficacy of ITI in our patients, case 1 was successful, whereas case 2 failed. Therapy is still ongoing in cases 3 and 4. The importance of the intensity of initial therapy on the outcome of ITI remains to be fully evaluated. Nevertheless, although minor surgery such as CVAD insertion could be performed under bypassing therapy, our results emphasize that high-dose FVIII therapy is clinically effective and economically viable in patients with high-responding inhibitors. In addition, our findings suggest that this hemostatic strategy could be applicable to more invasive operations in patients with hemophilia A.
Footnotes
This submission is an original work and not previously published in any substantial part, not under consideration of publication elsewhere, and submitted to CATH for consideration of publication.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported in part by Health and Labour Sciences Research Grants (for Research on HIV/AIDS) from Ministry of Health, Labour and Welfare.