
Abstract
Prognosis of pulmonary embolism (PE) based on levels of
Levels of
Methods
This was a retrospective study of stable patients hospitalized with acute PE who had measurements of
The diagnosis of PE was made by computed tomographic (CT) pulmonary angiography in 280 patients (96%) and a high probability interpretation of the ventilation/perfusion lung scan in 12 patients (4%). Patients were excluded if they were hypotensive (systolic blood pressure <90 mm Hg) or on ventilatory support.
The mini Vitek Immuno Diagnostic Assay System (VIDAS) Quantitative
Cardiac troponin I (cTnI) was measured by Chemiluminescent assay, Access immunoassay system, Beckman Coulter, Fullerton, California, at St. Joseph Mercy Oakland Hospital, and ADVIA Centaur TnI-Ultra, Deerfield, Illinois, at the William Beaumont Hospital. Prior to October 2006 at William Beaumont Hospital, cTnI was defined as normal if ≤0.3 ng/mL. Afterward, at William Beaumont Hospital and at St. Joseph Mercy Oakland Hospital, cTnI was defined as normal if <0.05 ng/mL.
Creatine kinase isoenzyme MB (CK-MB) at William Beaumont Hospital was assayed in with 2-site sandwich immunoassay (ADVIA Centaur CK-MB, Deerfield, Illinois). Levels >5.0 ng/mL were defined as elevated (high). CK-MB at St. Joseph Mercy Oakland Hospital was assayed in 10 patients with a modified 2-site immunoenzymatic (sandwich) assay (Access immunoassay system, Beckman Coulter, Fullerton, California). Levels >6.3 ng/mL were defined as elevated (high).
Right ventricular (RV) dilatation by echocardiography was determined by a qualitative impression on the reports in 186 (85%) of 219 in whom echocardiograms were obtained. Right ventricular/left ventricular (RV/LV) ratios were measured in 33 (15%) of 219. An RV/LV ratio >1 was defined as RV dilatation. 7
Statistical analysis
We arbitrarily selected a D-dimer cut-off of 5000 ng/mL for comparisons of mortality with values above and below this level. Data were analyzed using SPSS Version 11.5 for Windows (SPSS Inc., Chicago, Illinois). Significant tests of equality of 2 proportions were carried out using the 2-tail Fisher exact test (http://www.graphpad.com/quickcalcs/contingency2.cfm); 95% confidence intervals (CI) were calculated using online software (http://www.hutchon.net/ConfidOR.htm). Student t-test was used for comparing means of continuous variables.
Results
Baseline characteristics of patients are shown in Table 1. None of the baseline characteristics differed significantly comparing those with D-dimer <5000 ng/mL with those with D-dimer ≥5000 ng/mL.
Baseline Characteristics According to D-dimer Level a
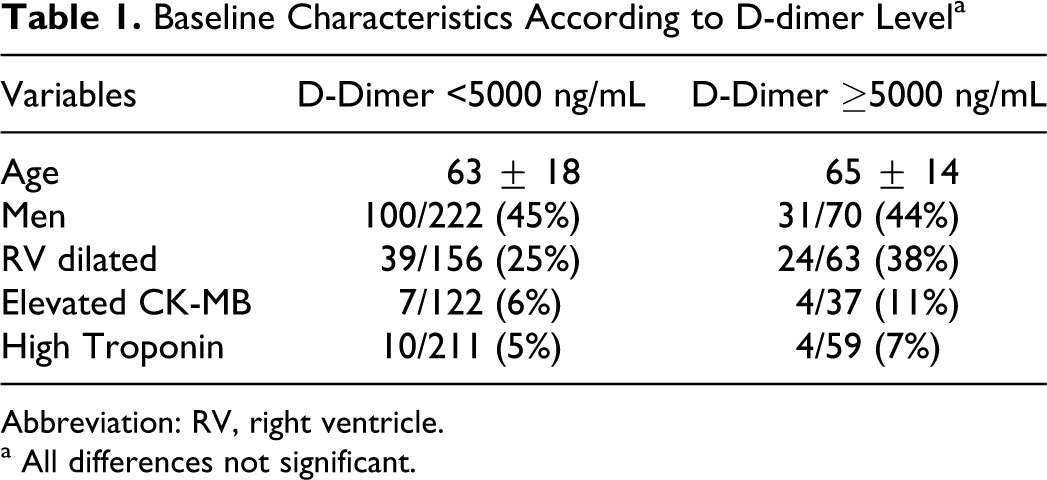
Abbreviation: RV, right ventricle.
a All differences not significant.
In-hospital mortality from PE was 0% (0 of 222) with D-dimer <5000 ng/mL compared with 2.9% (2 of 70) with D-dimer ≥5000 ng/mL (P = .06; Table 1). In-hospital all-cause mortality was 2.3% (5 of 222) with D-dimer <5000 ng/mL compared with 2.9% (2 of 70) with D-dimer ≥5000 ng/mL (NS; Table 2).
Mortality and D-Dimer Level
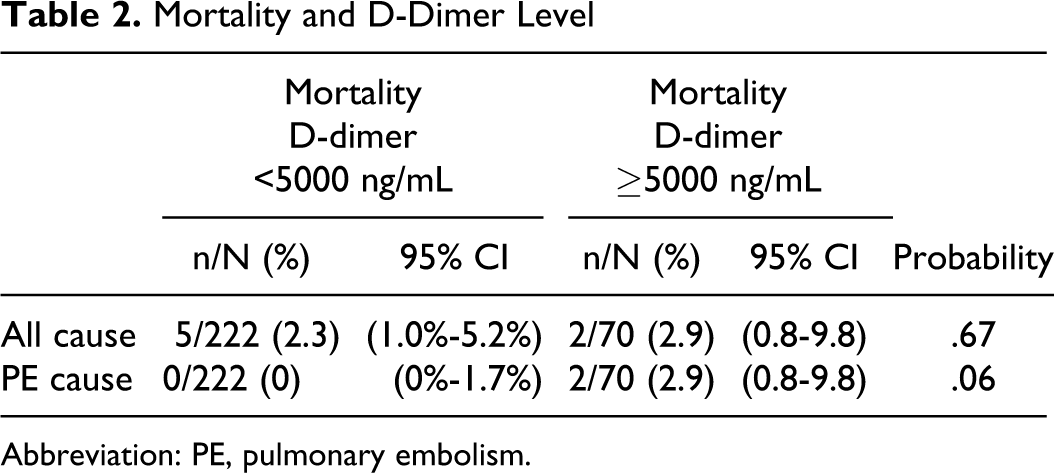
Abbreviation: PE, pulmonary embolism.
Among patients with D-dimer ≥5000 ng/mL who had RV dilatation, mortality from PE was 4.2% (1 of 24) compared with 0% (0 of 39) among patients with D-dimer <5000 ng/mL who had RV dilatation (NS). Combinations of D-dimer level and RV dilatation are shown in Table 3.
Death From Pulmonary Embolism According to D-Dimer and Right Ventricular Size
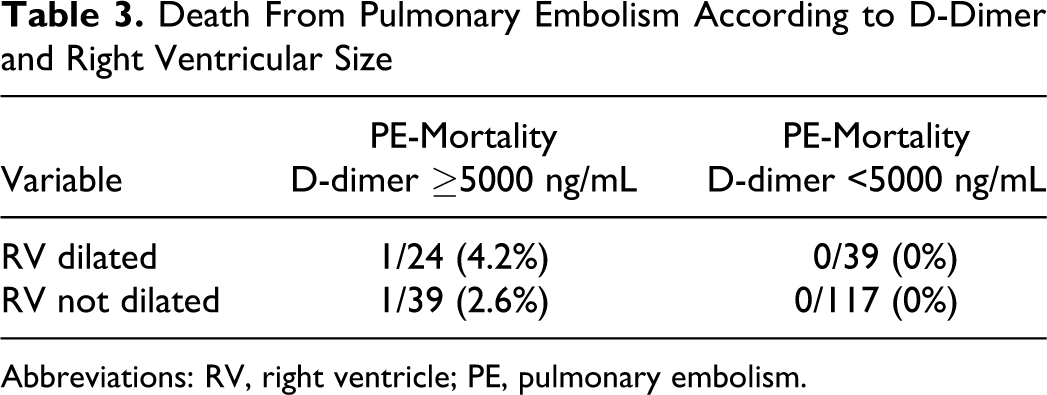
Abbreviations: RV, right ventricle; PE, pulmonary embolism.
Discussion
The prevalence of in-hospital all-cause mortality did not differ significantly among patients with D-dimer ≥ 5000 ng/mL (2.9% mortality) and those with lower levels (2.3% mortality). In-hospital mortality from PE showed differences that almost reached statistical significance (0% vs 2.9%).
Previous investigators used cut-off levels of 6-fold higher than normal, 5 3000 ng/mL, 3 4200 ng/mL, 6 and 5500 ng/mL. We arbitrarily selected 5000 ng/mL.
The only previous investigation of in-hospital mortality with stable patients showed, as we showed, no difference in all-cause mortality or PE-related mortality 5 (Table 4). All-cause mortality, however, with longer follow-up of 15 days to 3 months, was shown to be higher in patients with elevated D-dimer levels.3–6 Mortality from PE at 15 days to 3 months was found to be higher in one investigation 6 but not in another. Irrespective of whether patients with markedly elevated levels of D-dimer showed statistically significantly higher mortalities from PE, the mortality rates were insufficient to warrant thrombolytic or invasive therapy.
Mortality Related to D-Dimer
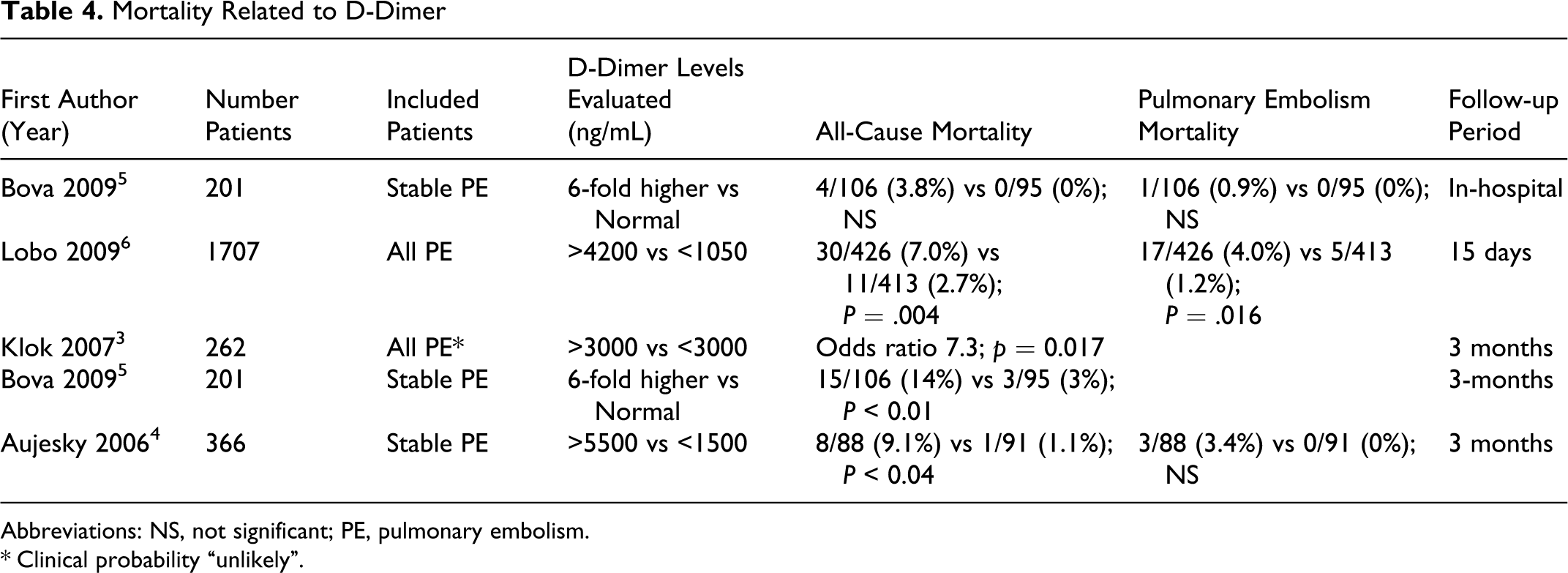
Abbreviations: NS, not significant; PE, pulmonary embolism.
*Clinical probability “unlikely”.
Strengths of this investigation are that both all-cause mortality and PE-related mortality were assessed in stable patients, which, to our knowledge, had been done in only one previous investigation. A weakness is that relatively few patients were evaluated, although we evaluated a larger number than previously evaluated in stable patients.
In conclusion, markedly elevated levels of D-dimer did not indicate a high mortality from PE or all-cause mortality during hospitalization.
Footnotes
All authors had access to the data and played a role in writing this manuscript.
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.