
Abstract
The purpose of this investigation is to assess the prevalence of elevated cardiac biomarkers, with or without estimates of right ventricular (RV) size, in stable patients with acute pulmonary embolism (PE). Our hypothesis is that the combination of high levels of cardiac troponin I (cTnI), high creatine kinase isoenzyme MB (CK-MB), and normal size RV are sufficiently uncommon in stable patients with PE to make the diagnosis of PE unlikely. Retrospective review showed a high cTnI plus high CK-MB in 20 (3.4%) of 585 stable patients with acute PE. A high cTnI plus high CK-MB with normal RV size was shown in 5 (1.9%) of 264 patients. In stable patients with such findings, therefore, PE is unlikely and other diagnoses, particularly acute coronary syndrome, should be considered before pursuing a diagnosis of PE.
Cardiac biomarkers, especially cardiac troponin I (cTnI), often used in combination with echocardiographic assessment of right ventricular (RV) size or function, have been used for risk stratification of patients with acute pulmonary embolism (PE).1–4 The proportion of stable patients having PE with cTnI elevated to levels consistent with myocardial infarction was uncommon and ranged from 3.4% to 4.2%.3,5,6 Elevated creatine kinase isoenzyme MB (CK-MB) also was uncommon in stable patients with acute PE, the prevalence being 12.3% and 26.6%.7,8 The uncommon occurrence of biomarkers elevated to levels consistent with myocardial infarction in stable patients with acute PE suggests that high levels of biomarkers might be used for an entirely different purpose than risk stratification. We hypothesize that the prevalence of the combination of high cTnI, high CK-MB and normal size RV is sufficiently low to suggest an unlikely diagnosis of PE in stable patients. The purpose of this investigation was to test this hypothesis.
Methods
This was a retrospective study of stable patients hospitalized with acute PE who had measurements of cTnI, CK-MB, and estimates of RV size. Patients were studied from March 2007 through May 2010 at St. Joseph Mercy Oakland Hospital, Pontiac, Michigan (217 patients) and from January 2004 through June 2008 at William Beaumont Hospital, Royal Oak, Michigan (656 patients). The patients reported in this investigation were included in a previous investigation of prognosis based on cTnI and RV size. 3 The investigation was approved by the institutional review boards of both hospitals. Hospitalized patients with PE were identified by computer listings of International Classification of Diseases, Ninth Revision (ICD-9) discharge codes. Medical records, reports of computed tomographic (CT) pulmonary angiograms, ventilation/perfusion (V/Q) lung scans, laboratory data, and reports of echocardiograms were reviewed in all patients.
The diagnosis of PE was made with CT pulmonary angiography in 843 (97%) of 873 patients and a high-probability interpretation of the V/Q lung scan in 30 (3%) of 873 patients.
Patients were excluded if they were unstable (systolic blood pressure <90 mm Hg or on ventilator support). Patients were also excluded if they had a possible cause of cTnI elevation other than PE, such as heart failure9,10 (which we defined as ejection fraction <40%), chronic obstructive pulmonary disease,11,12 pneumonia, 13 hemodialysis, 14 coronary artery bypass graft surgery within 1 week, or myocardial infarction or ischemia within 1 week. Patients were also excluded if they had other known causes of an elevated CK or CK-MB including rhabdomylosis,15,16 severe muscle trauma, 17 and liposuction. 18
Cardiac biomarkers (cTnI and CK-MB) were measured within 48 hours before or after the diagnosis of PE was made. Levels defined as normal, intermediate, and high (highly suggestive of myocardial infarction or “critical”) and methods of measurement are shown in Table 1.
Cutoff Levels for Interpretation and Methods of Measurement of Cardiac Troponin I and Creatine Kinase Isoenzyme MB
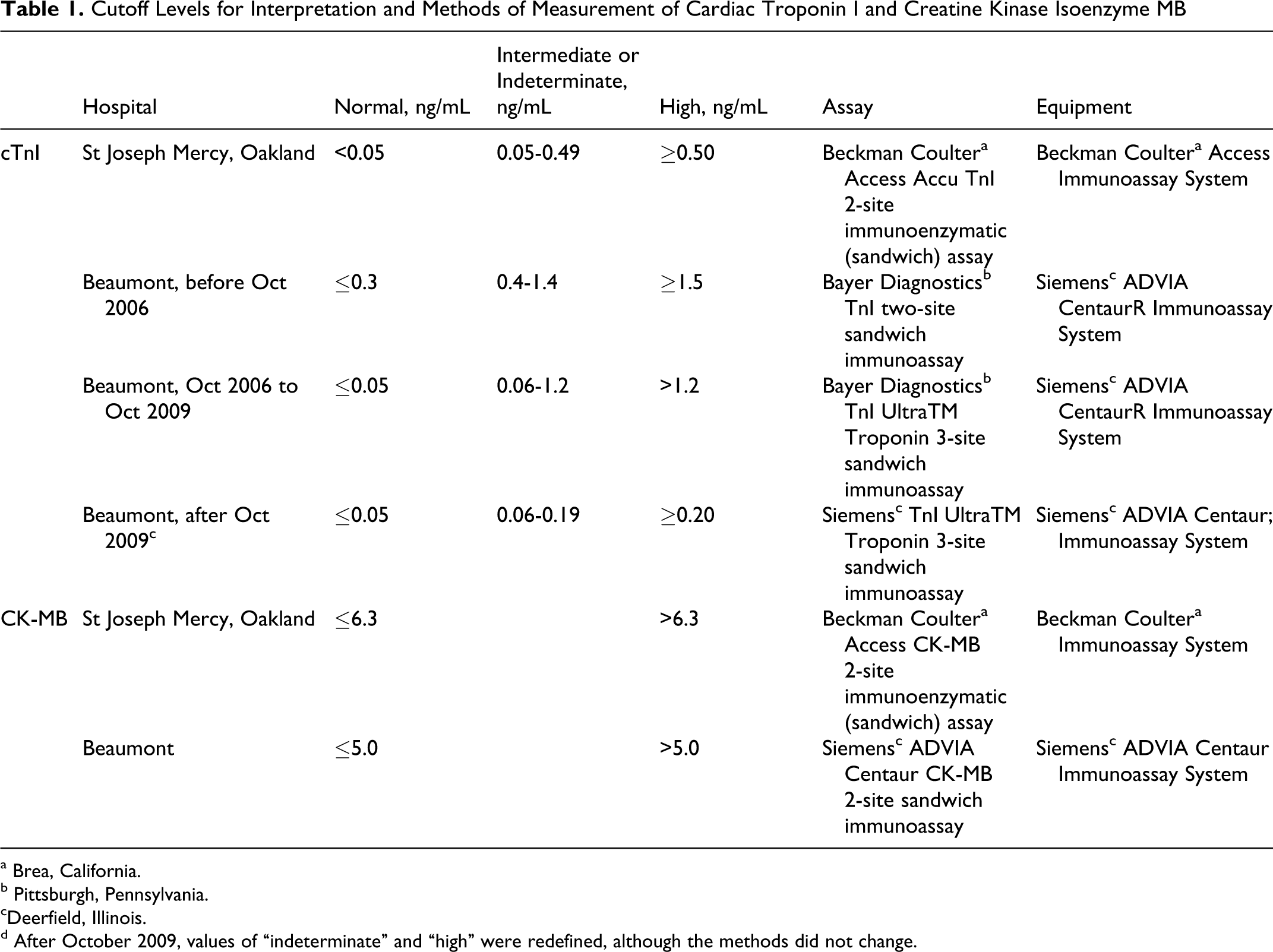
a Brea, California.
b Pittsburgh, Pennsylvania.
cDeerfield, Illinois.
d After October 2009, values of “indeterminate” and “high” were redefined, although the methods did not change.
Echocardiograms were obtained in 601 (69%) of 873 patients. Right ventricular dilatation by echocardiography was determined by a qualitative impression in 498 (83%) of 601 patients. Right ventricular/left ventricular (RV/LV) ratios were measured in 103 (17%) of 601 patients. An RV/LV ratio >1 was defined as RV dilatation. 19 Assessments of the RV were obtained from the echocardiographic reports.
Results
Among 873 stable patients with acute PE who had measurements of either cTnI or CK-MB, age was 67 ± 16 years (mean ± standard deviation) and 377 patients (43%) were males.
Cardiac Troponin I
Cardiac troponin I was high in 103 (12.1%) of 852 stable patients with PE. In 580 patients, both cTnI and RV size were measured with normal size RV in 406 patients and dilated RV in 174 patients. A high cTnI in combination with a normal RV size was shown in 42 (10.3%) of 406 patients (Figure 1). A high cTnI in combination with a dilated RV was shown in 48 (27.6%) of 174 patients (P < .0001). Values of cTnI above 50 times the normal cutoff were observed in 5 (0.6%) of 852 patients, irrespective of RV size, and in 2 (0.5%) of 406 with a normal size RV.
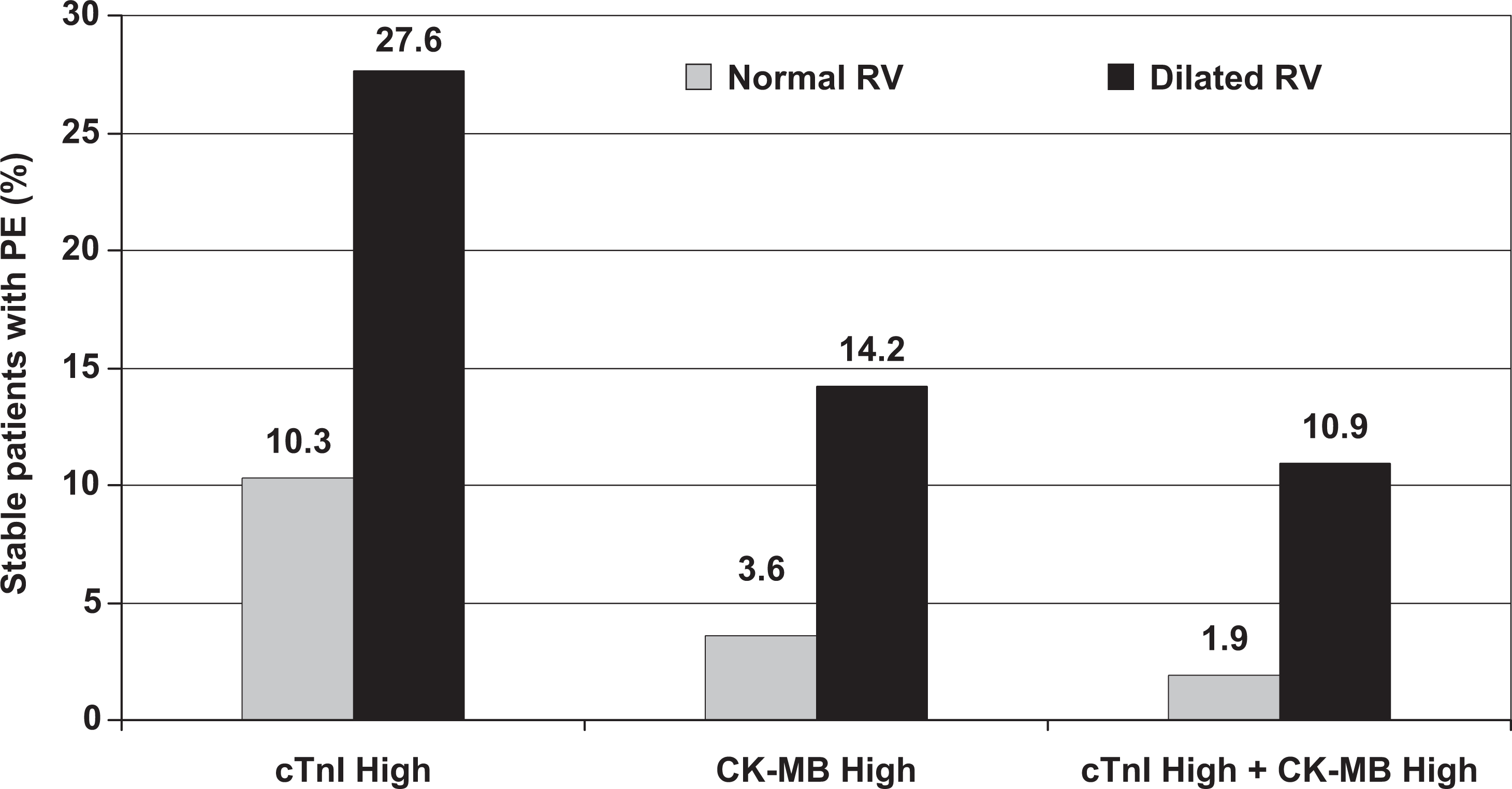
Proportion of stable patients with acute pulmonary embolism (PE) With various combinations of high cardiac troponin I (cTnI), high creatine kinase isoenzyme MB (CK-MB), and normal size or dilated right ventricle (RV).
Creatine Kinase MB Isoenzyme
Creatine Kinase MB Isoenzyme was high in 30 (5.0%) of 606 stable patients with PE. In 413 patients, both CK-MB and RV size were measured. A high CK-MB in combination with a normal RV size was shown in 10 (3.6%) of 279 patients (Figure 1). A high CK-MB in combination with a dilated RV was shown in 19 (14.2%) of 134 patients (P = .0003). Values of CK-MB above 2 times the normal cutoff were shown in 4 (0.7%) of 606 patients and 0 (0%) of 279 patients (Figure 1) with a normal size RV.
Cardiac Troponin I and CK-MB
Among 585 patients who had measurements of both cTnI and CK-MB, but not necessarily RV size, various combinations of cTnI and CK-MB are shown in Table 2. Both a high cTnI and high CK-MB were shown in 20 (3.4%) of 585 patients. In 392 patients, cTnI, CK-MB, and RV size were measured. A high cTnI plus high CK-MB in combination with a normal RV size was shown in 5 (1.9%) of 264 patients (Figure 1). A high cTnI plus high CK-MB in combination with a dilated RV was shown in 14 (10.9%) of 128 patients (P = .0002). Cardiac Troponin I above 50 times the normal cutoff combined with CK-MB above 2 times the normal cutoff were shown in 0 (0%) of 585 and 0 (0%) of 264 patients with normal size RV.
Cardiac Troponin I and Creatine Kinase Isoenzyme MB in Stable Patients With Pulmonary Embolism
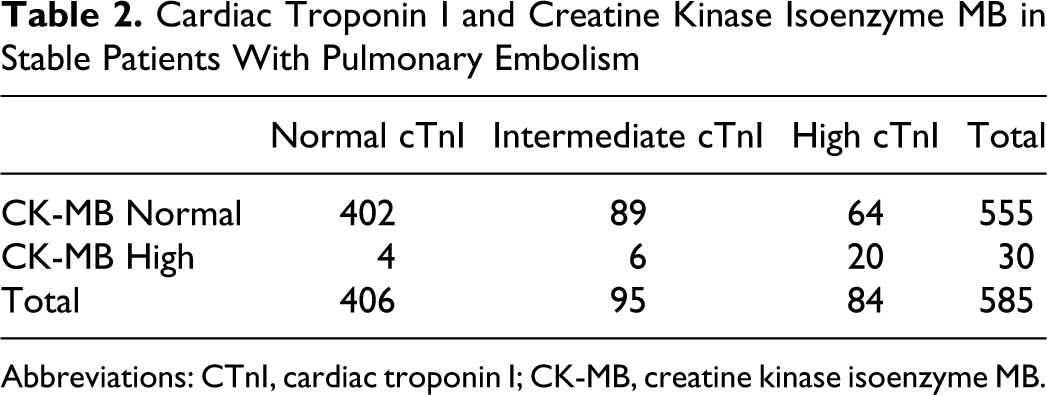
Abbreviations: CTnI, cardiac troponin I; CK-MB, creatine kinase isoenzyme MB.
Discussion
A high cTnI and CK-MB in stable patients with normal RV size was uncommon (1.9%). Proportions of patients with high levels of cTnI and CK-MB and normal size RV all differed significantly from those with a dilated RV. It would seem that the prevalence of high levels of cTnI and CK-MB is dependent on RV size.
We focused on cTnI levels that were definitely elevated and abnormal as opposed to any value above the normal cutoff that some laboratories define as an intermediate elevation. Douketis et al in 2002 described 1 (4.2%) of 24 patients with acute PE who had elevated cTnI level consistent with myocardial infarction, 5 and in 2004 Douketis et al described 16 (3.5%) of 458 patients with such cTnI levels. 6 These were less than we observed, 12.1%, among 852 patients in this investigation. La Vecchia et al, however, among 48 patients with PE, described 29.2% with such elevations of cTnI, but some of these patients were unstable. 20
Kucher et al 21 and Punukollu et al 7 described 26.4% and 21.1% of stable patients with PE who had any elevation of cTnI with RV enlargement and/or dysfunction. Others described this combination among unstable as well as stable patients.4,20,22–27 We were unable to identify investigations of patients with PE in which levels of cTnI consistent with acute myocardial infarction in combination with RV size were described.
Elevated levels of CK-MB were reported in 7.7% patients with PE by Adams et al, which was similar to our findings (5.0%), although they included unstable as well as stable patients. 28 Others, among stable patients with PE, showed a higher proportion with elevations of CK-MB, 12.3% and 26.5%.7,8 Konstantinides et al reported 15.1%, but some patients were unstable. 1 We found no investigations in which the proportion of patients with PE who had both an elevated cTnI and CK-MB was described.
Strengths of this investigation are the large number of included patients (873), although data in various subcategories of patients were frequently missing. We are not aware of any other investigations in which combinations of cardiac biomarkers and RV size were assessed in patients with PE. Weaknesses are that the investigation was retrospective. Echocardiographic evidence of RV enlargement was usually based on the impression of the reader rather than objective measurement. Levels of cTnI were measured by different techniques at the participating hospitals. Values of cTnI that were assessed as elevated changed during the period of the investigation.
In conclusion, a high cTnI at levels consistent with acute myocardial infarction, plus high CK-MB are uncommon in stable patients with acute PE in whom the RV is not dilated. In patients with such findings, the diagnosis of PE is unlikely, and other diagnoses, particularly acute coronary syndrome, should be considered before pursuing a diagnosis of PE.
Footnotes
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
The authors received no financial support for the research and/or authorship of this article.