
Abstract
Keywords
Introduction
Ischemic coronary heart disease (CHD) is the leading cause of death in developed countries. Recent European statistics established that CHD is directly responsible for 43% of all deaths in men and 55% of all deaths in women. 1 In addition, the prevalence of CHD is quickly increasing in developing countries, and it is expected to become the leading cause of death. 2 Cigarette smoking is a well-established and modifiable major risk factor that is closely associated with ischemic CHD, vice versa CHD is the leading cause of death between smokers.3,4 Though cigarette smoking is a modifiable and major risk factor for CHD, smoking cessation is not easy, and a large proportion of patients with CHD still continue smoking despite all recommendations and warnings.
Recent studies indicate that cigarette smoking has many negative effects on cardiovascular system. Smoking causes endothelial dysfunction,5,6 increases systemic inflammation 7 (via increasing interleukin 6, C-reactive protein, homocysteine, fibrinogen), changes the lipid profile and prepares an atherogenic milieu 8 (increases low-density lipoprotein cholesterol and triglycerides, decreases high-density lipoprotein cholesterol), promotes atherosclerotic progression by increasing oxidative stress, lipid peroxidation and mitochondrial damage,7,9 destabilizes atherosclerotic plaque by increasing matrix metalloproteinases, 10 and finally increases platelet activation and triggers coagulation cascade, which may result with atherothrombosis.11,12
In this study, we aimed to determine the impact of cigarette smoking on platelet function in patients with ischemic CHD and to evaluate whether aspirin can inhibit platelet activity triggered by this potential thrombogenic stimulus.
Materials and Methods
Patients
The study was approved by the local institutional ethics committee and all the participants gave informed consent before enrollment. We recruited a total of 40 patients (20 volunteer current smoker [49.4 ± 6.7 years old, 20% women) and 20 nonsmoker patients [56.7 ± 6.9 years old, 20% women]) with angiographically proven CHD, into the study. All patients were on follow-up with 300 mg daily aspirin from the chronic stable CHD outpatient clinic. Smoker patients were insisting to continue smoking despite all warnings and recommendations. We excluded patients with diabetes mellitus, chronic renal dysfunction, liver disease, cancer, established hematological diseases, and platelet function disorders (Glanzmann disease, etc).
Platelet Function Tests
Three samples of whole blood were obtained from patients via superficial veins of the arm. Two samples were collected in 3.8% sodium citrate (buffered, pH 5.5, Vacutainer, Becton Dickinson, Plymouth, UK) for platelet function tests, and the other sample was collected in ethylenediaminetetraacetic acid (EDTA) containing tube for complete blood count. The specimens were kept in room temperature and platelet function assays were processed within 1 hour of blood sampling.
Blood samples were obtained at least 12 hours after smoke-free period and 2 hours after aspirin intake from different arm’s veins. We studied platelet function at the morning, just before and 15 minutes after the first cigarette. All the participants smoked a single regular tobacco from the same commercially available pack. Platelet function was assessed by the Platelet Function Analyzer (PFA)-100 (Siemens Healthcare, Marburg, Germany) with collagen and epinephrine (Col/Epi) and collagen and adenosine diphosphate (Col/ADP) cartridges. Briefly, PFA-100 system simulates primary hemostasis in vitro conditions. The device aspirates 800 µL of whole blood anticoagulated with sodium citrate through an aperture of 147 µm in a capillary membrane coated with collagen. Blood samples interact with platelet activators (epinephrine or ADP) and collagen-coated membrane in the cartridges, and complete occlusion of the aperture by cloth occurs. The system measures the time required for total occlusion of the aperture by platelet plugs called closure time (CT) which demonstrates in vitro platelet function. The normal reference range for PFA-100 is accepted as 98 to 185 seconds with Col/Epi cartridges and 81 to 113 seconds with Col/ADP cartridges. 13 Aspirin responsiveness is defined as having a CT of <186 seconds with Col/Epi cartridges, despite regular aspirin therapy. 13 Coefficients of variation for within and between days were <10% and <15% when Col/ADP and Col/Epi cartridges were tested, respectively. A recent study that compared conventional aggregometry, PFA-100 and Ultegra (VerifyNow, Accumetrics, San Diego, California) systems reported high correlation (r 2 = .73-.86) between platelet analyzer readings and aggregation after administration of a single pill of aspirin. 14
In this study, compliance with aspirin therapy was ascertained by a personal interview.
Statistical Analyses
Categorical variables are presented as frequencies and percentages. Chi-square test and Fisher exact test are been used to compare categorical variables. Mean values and standard deviations are been calculated for continuous variables. Student t test and Mann-Withney U test are used to compare continuous variables. To adjust the role of each parameter on platelet function, a multivariate analysis (forward stepwise Cox regression analysis) is performed. Serial platelet function assay data are analyzed by paired samples t test. Relation between the platelet function and cigarette smoking is been evaluated with chi-square test. A P value of ≤.05 is accepted as statistically significant.
Results
Post aspirin platelet hyperactivity was present in 4 smoker (20%) and 3 nonsmoker (15%) patients at the beginning. Baseline patient characteristics are shown in Table 1.
Baseline Characteristics of the Patients and Controls
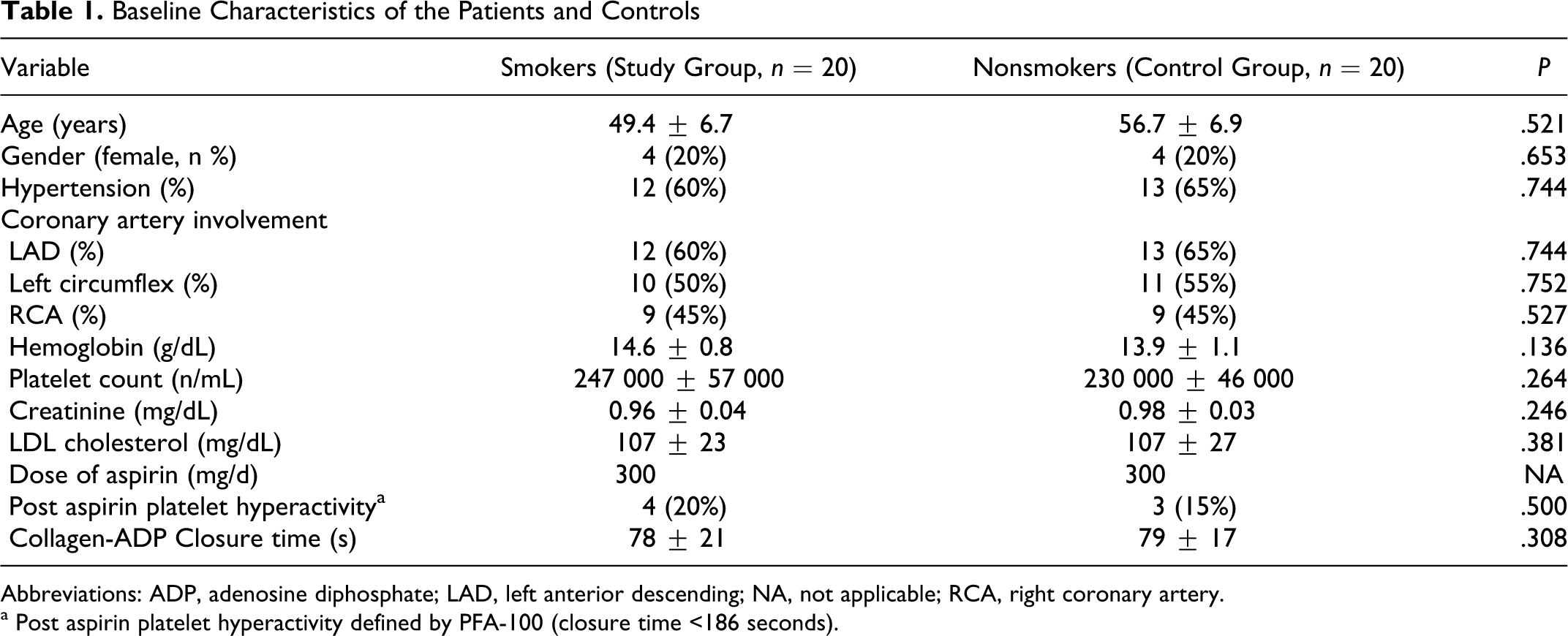
Abbreviations: ADP, adenosine diphosphate; LAD, left anterior descending; NA, not applicable; RCA, right coronary artery.
a Post aspirin platelet hyperactivity defined by PFA-100 (closure time <186 seconds).
We determined a significant increase in platelet aggregation by the PFA-100 after smoking a single cigarette (P = .004). Closure time became shorter after smoking in patients with and without baseline post aspirin platelet hyperactivity. After smoking, 4 more patients had short Col/Epi CTs below the predefined limit and became aspirin nonresponders (P = .004). Figure 1 shows pre- and post-smoking CTs measured with Col/Epi and Col/ADP cartridges. No significant differences in demographics, hematological, and biochemical parameters were determined between aspirin responders and nonresponders. Closure time determined by the use of Col/ADP cartridges were 80 ± 22 seconds and 72 ± 14 seconds in aspirin responder and nonresponder smoker patients, respectively. Baseline characteristics of smoker patients are shown in Table 2.
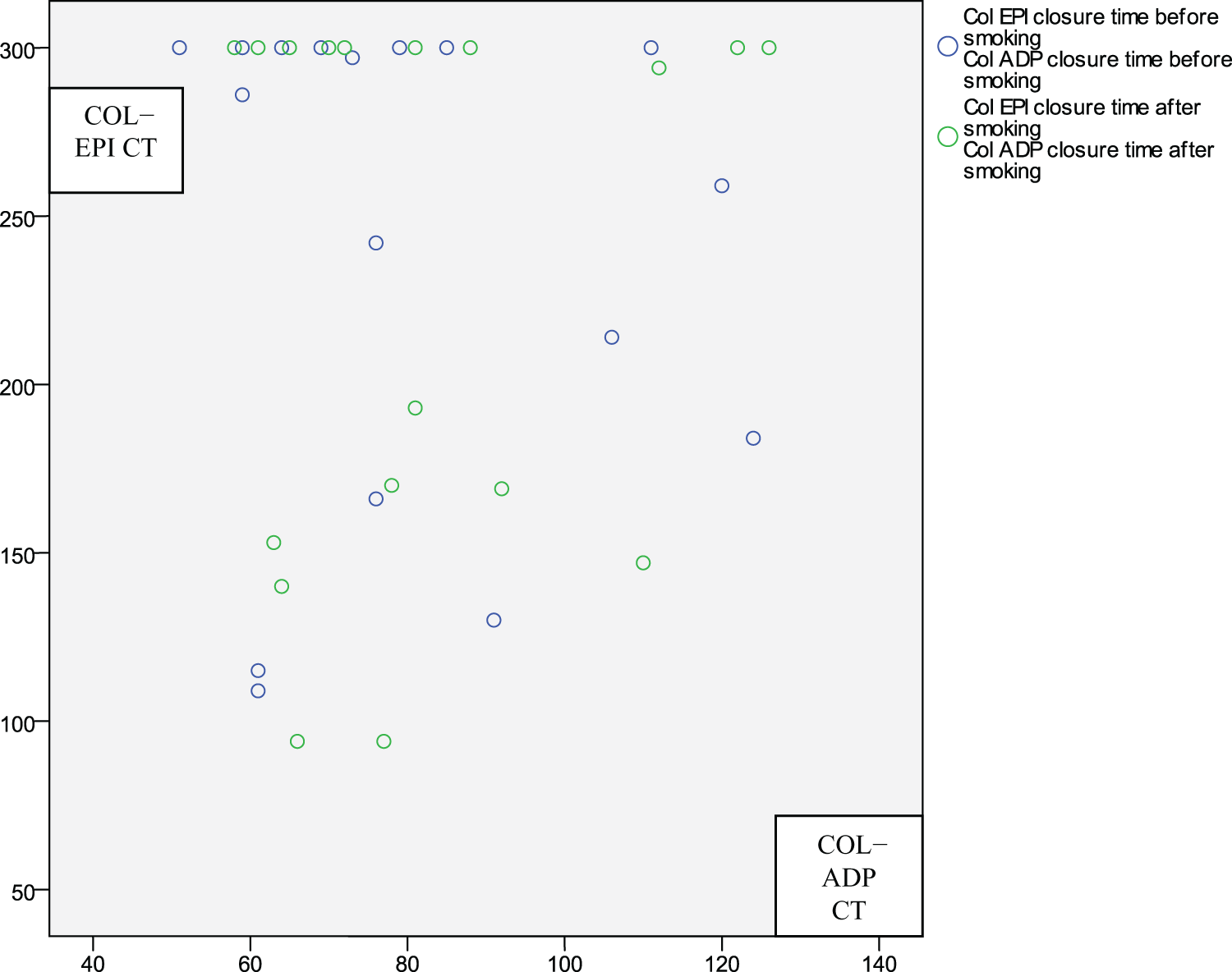
Closure time before and after smoking. Col EPI indicates collagen and epinephrine; Col ADP, collagen and adenosine diphosphate.
Aspirin Response and Baseline Characteristics of Smoker Patients
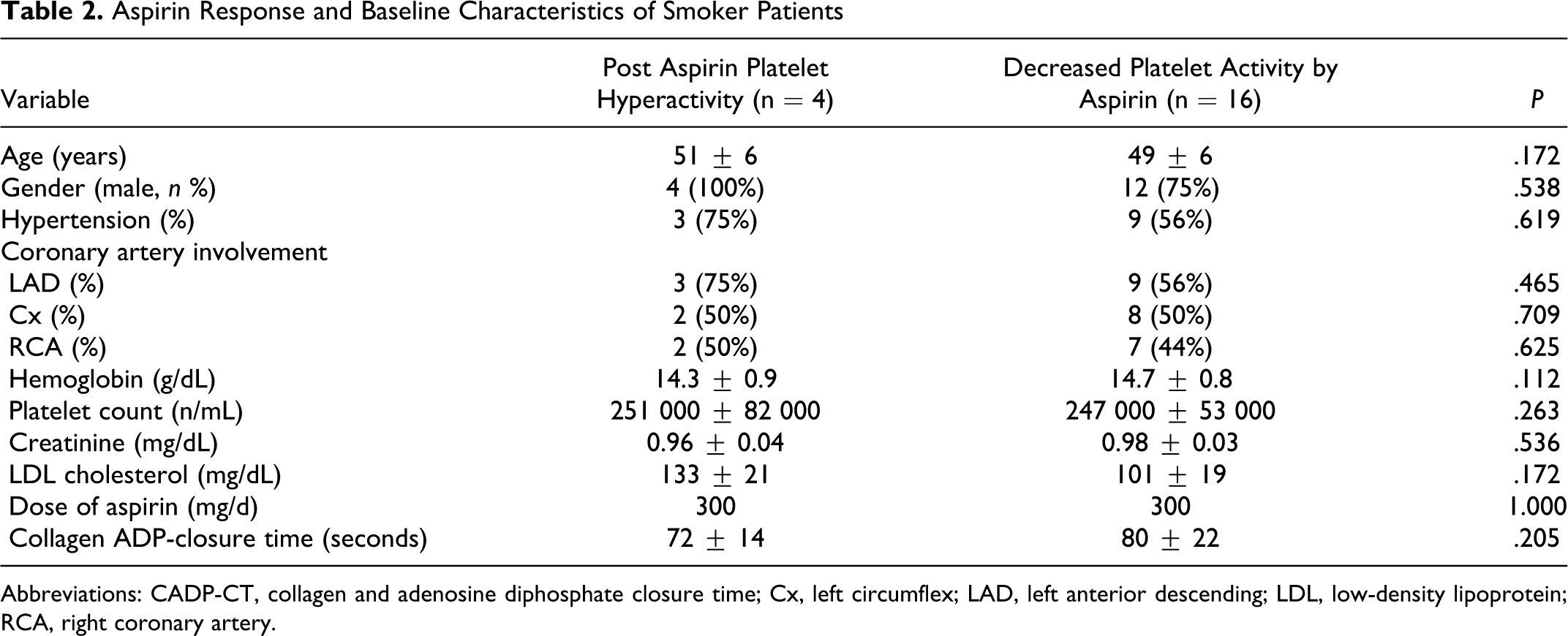
Abbreviations: CADP-CT, collagen and adenosine diphosphate closure time; Cx, left circumflex; LAD, left anterior descending; LDL, low-density lipoprotein; RCA, right coronary artery.
Closure time measured with Col/ADP cartridges did not change significantly after smoking 79 ± 21seconds versus 81 ± 18 seconds (P = .416). Impact of smoking on PFA-100 Col/Epi and Col/ADP CTs is shown in Table 3.
Platelet Function and Cigarette Smoking

Abbreviations: ADP, adenosine diphosphate; CT, closure time.
a Range of closure time.
b By paired samples t test.
Discussion
In this study, we determined that smoking, even a single cigarette, may increase platelet activity in aspirin responder and nonresponder patients with stable ischemic CHD. Unfortunately, aspirin failed to prevent this smoking-induced platelet activation. Our results emphasize one more time the importance of smoking cessation in patients with CHD. Antithrombotic therapy of patients with CHD who continue smoking merits careful evaluation since these individuals may have increased platelet activity that cannot be inhibited by aspirin. Further and personalized antithrombotic regimens may have potential indication in smoker CHD patients.
The influences of cigarette smoking on platelets can be evaluated under 2 different titles; acute and chronic impacts. However, these effects are mostly intimate and it is substantially difficult to distinguish one from the other. In this respect, the impact of cigarette smoking on platelet function has been previously studied, but different studies established controversial findings. For example, a recent study suggested that although physical exercise and smoking increased the levels of plasma catecholamines in patients treated with and without β-blockers, these stimuli did not enhance platelet aggregation stimulated by ADP,
In contrast numerous studies suggested that cigarette smoking increased platelet aggregation. A flow cytometric study established the presence of in vivo platelet activation immediately after smoking and a significant number of circulating platelets that are already in activated state in chronic smokers. 18 Hung and colleagues investigated the role of cigarette smoking on platelet function and determined that cigarette smoking acutely increases platelet aggregation and thrombus formation in patients with CHD. 12 Habitual cigarette smoking also changes platelet thromboxane A2 metabolism and causes alteration of susceptibility to aspirin’s antiplatelet effects. 19 The controversial findings determined in different studies with similar patient characteristics and populations may be partially explained by the use of different methods in the assessment of platelet function. To compare these studies performed by different platelet function tests may cause another source of controversy.
A recent study that enrolled 102 patients 24 hours after peripheral, coronary, or carotid artery stenting determined the presence of significantly lower P2Y12 reaction units by the VerifyNow system, suggesting enhanced clopidogrel-mediated platelet inhibition, in current smoker patients when compared to nonsmokers (P = .028). 20 However, in the same study aspirin-mediated platelet inhibition has been found to be similar between nonsmokers and former smokers or current smokers (P > .3). Multivariate regression analysis showed that cigarette smoking has been independently associated with posttreatment ADP-induced platelet reactivity (P = .026). 20 Enhanced clopidogrel-mediated platelet inhibition in smokers has also been supported by another evidence. 21 This phenomenon was explained to a certain extent with induction of cytochrome P450 enzyme system by cigarette smoking. 22 A substudy of the CHARISMA (Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management, and Avoidance) trial emphasized that clopidogrel therapy may be more effective and even increase bleeding risk in current smokers than in nonsmokers. 23 The study by Addad et al, in a small cohort of patients with stable CHD under aspirin therapy established significantly shortening of Col/Epi CT after cigarette smoking. However, this phenomenon was not determined in clopidogrel-treated patients. 24
In our study, we determined a trend of enhanced platelet aggregation within minutes after smoking a single cigarette. Aspirin failed to eliminate this source of platelet stimulation at the dose of 300 mg. This increase in platelet aggregation is important since it is detectable even in a small patient population and after a single cigarette. A projection of this increased aggregation trend in the smoker ischemic CHD patient population may indicate how many patients are at risk of new thrombotic events. In our study, none of the patients were on clopidogrel therapy, nevertheless, PFA-100 system cannot determine clopidogrel’s antiplatelet effect by its commercially available cartridges.
Currently, routine assessment of platelet function in patients with CHD treated with aspirin is not recommended for all patients but may perhaps be used in a variety of individuals who are at high risk of thrombosis, for example, patients with recent stent thrombosis or in those undergoing unprotected left main coronary artery or left main bifurcation interventions. 25 Active smokers may be another potential candidates for platelet function assay-guided antiplatelet therapy.
Our study had also some limitations. We used a single point of care test in the assessment of platelet function, and compliance with antithrombotic therapy was evaluated by a questionnaire. Furthermore, although the sample size was sufficient for statistical analyses and slightly bigger than recent studies it was still small. Howsoever patients with ischemic CHD continued smoking, we observed that they do not want to be enrolled in these kinds of studies.
We determined an interesting trend indicating that smoking may increase platelet aggregation in patients with ischemic CHD, and secondary atherothrombotic prevention strategy recruiting aspirin did not prevent this platelet hyperactivity. Patients with ischemic heart disease should avoid cigarette smoking though enhanced platelet aggregation may lead to atherothrombotic complications (ie, acute coronary syndromes). Of note, further antithrombotic agents for example clopidogrel may have potential indication in patients with CHD who insist to continue cigarette smoking since recent evidence indicates that clopidogrel is not negatively influenced by cigarette smoking, vice versa its efficiency may even increase due to increased enzymatic activation in the liver. Novel antithrombotics with different action mechanisms may also have potential indications in smoker CHD patients.
Footnotes
Acknowledgments
The study was supported by Istanbul University Scientific Research Projects Unit and Turkish Society of Cardiology, a nonprofit association and a member of the European Society of Cardiology.
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: The study was supported by Istanbul University Scientific Research Projects Unit and Turkish Society of Cardiology.