
Abstract
The aim of this study was to assess the baseline platelet hyperactivity in patients with acute coronary syndrome (ACS) and correlate it with the disease severity and clinical outcome.
Participants and Methods:
This study was conducted on 60 patients with the first attack of non-ST-segment elevation ACS and 30 healthy controls. Patients were subdivided into 2 groups: group I: 40 patients with non-ST-segment elevation myocardial infarction (NSTEMI) and group II: 20 patients with unstable angina. All the studied patients were subjected to baseline platelet function analysis using platelet function analyzer 100 (PFA-100).
Results:
Group I patients showed significantly lower PFA-100 closure time (CT) than group II (P = .04) and control group (P = .03). The occurrence of complications in NSTEMI patients was associated with older age, hypertension, and shorter baseline collagen adenosine diphosphate PFA-100 CT (P < .05).
Conclusion:
NSTEMI patients proved to have enhanced platelet function that can be used as a predictor of the outcome.
Introduction
According to the report of World Health Organization (2011), 1 cardiovascular diseases are the number one cause of death globally. Ischemic heart disease has been reported to be responsible for about 21% of all deaths among Egyptians, 2 in 2002.
Acute coronary syndrome (ACS) is a major health problem and represents a large number of hospitalizations annually. 3 The ACS covers the spectrum of clinical conditions ranging from unstable angina (UA) to non-ST-segment elevation myocardial infarction (NSTEMI) and ST-segment elevation MI (STEMI). 4 Numerous lines of evidence suggest that platelets play a dominant pathogenic role in the development and outcome of ACS. 5 This complex syndrome can progress from plaque instability within an atherosclerotic artery to plaque rupture, exposing the highly procoagulant contents of the atheroma core to circulating platelets and coagulation proteins and culminating the formation of intracoronary thrombus resulting in the reduction of coronary blood flow, myocardial ischemia, and necrosis.6,7
Platelet function analyzer 100 (PFA-100) measures the time needed for a platelet plug to form after the activation of platelets by pathophysiological-relevant stimuli (eg, collagen and adenosine diphosphate or collagen and epinephrine). 8 The PFA-100 is simple to perform, rapid, and can test relatively small volumes (0.8 mL/cartridge) of citrated blood up to 4 hours from sampling. 9
Few studies have investigated platelet function before starting antiplatelet therapy in patients with ACS syndrome.5,10 Therefore, the aim of this study was to assess the baseline platelet hyperactivity in patients with ACS using PFA-100 and correlate it with the disease severity and clinical outcome.
Participants and Methods
Participants
This study was conducted on 60 non-ST-segment elevation ACS patients attending Ain Shams University Hospitals and 30 age- and sex-matched healthy individuals as a control group. The study protocol was approved by the local ethical committee of Ain Shams University, and an informed consent was obtained from each participant before enrollment.
Patients Group
It included 60 patients who had non-ST-segment elevation ACS; 40 males and 20 females with a male-to-female ratio of 2:1. Their ages ranged from 22 to 73 years, with mean age of 53.3 ± 10.9 years. Patients were subdivided into 2 groups: group I: 40 patients with first attack of NSTEMI (32 males and 8 females, with mean age of 51.6 ± 11.9 years); group II: 20 patients with first attack of UA (8 males and 12 females, with mean age of 56.9 ± 7.4 years). The diagnosis of NSTEMI was made when ischemia is sufficiently severe to cause myocardial damage that results in the release of biomarkers of myocardial necrosis into the circulation. In contrast, the patient was considered to have UA if no such biomarker can be detected in the bloodstream hours after the initial onset of ischemic chest pain. 4
Exclusion criteria included any acute illness or fever within 4 weeks prior to enrollment, history of major surgery, trauma or malignancy within the preceding 3 months, hepatic or renal dysfunction, low hematocrit, low platelet count, and patients on antiplatelet drugs for any reason. Patients with complicated MI or heart failure were also excluded.
Patients were followed up for 6 months to observe the development of complications (the occurrence of death secondary to cardiovascular causes and recurrent ACS). Acute coronary syndrome was defined by the presence of symptoms compatible with recurrent ischemia requiring rehospitalization and coronary angiography). Patients known to be diabetic were on oral hypoglycemic drugs only and none of them received insulin. Among the hypertensive patients, 5 were on indapamide, 5 were on amlodipine, 4 were on β-blockers, and 4 were on enalapril, while among the dyslipidemic patients, 4 were on statins and 4 were on irregular treatment.
Control Group
Thirty healthy age- and sex-matched participants free from any known or suspected disease were included in the study. They were 21 males and 9 females (male-to-female ratio 2.3:1) with mean age of 50.7 ± 5.6 years.
All the studied individuals were subjected to the assessment of risk factors: fasting and postprandial blood sugar, serum cholesterol level, triglyceride level, low-density lipoprotein, and high-density lipoprotein using Synchron CX-7 (Beckman, Switzerland), (for patients not known to be dyslipidemic, the lipid profile was reassessed at least 6 weeks after the initial event); complete blood count using Beckman Coulter (United States) and baseline PFA-100 using collagen adenosine diphosphate (CADP) on whole blood samples. For the patients group only, CK-MB using Synchron CX-7 and coronary angiography was performed for the evaluation of the number of vessels affected, type of lesion, and thrombolysis in myocardial infarction (TIMI) flow in the culprit artery.
Sampling
Venous blood (2 mL) was collected from patients (before the intake of antiplatelet drugs) and controls and anticoagulated with 3.2% sodium citrate in the proportion of 9:1. Blood samples for PFA-100 were measured within 2 hours after blood sampling.
Methods
The baseline platelet function was determined by the CADP PFA-100 (Dade Behring, Germany) using CADP cartridge.
Principle of the Test
The CADP PFA-100 measures the time needed for the platelet plug to form after the activation of platelets by collagen adenosine diphosphate. The PFA-100 creates an artificial vessel consisting of a sample reservoir, a capillary, and a biologically active membrane with a central aperture, coated with collagen adenosine diphosphate. The application of a constant negative pressure aspirates the anticoagulated blood of the sample from the reservoir through the capillary and the aperture. A platelet plug gradually occludes the aperture; as a consequence, the blood flow through the aperture gradually decreases and eventually stops. The time needed for blood flow interruption (ie, closure time [CT]) is recorded. The CADP cartridge was used as the primary outcome variable because unlike the collagen/epinephrine (CEPI) CT, its value is typically not confounded by aspirin intake.11,12
Statistical Analysis
The data were coded, entered, and processed on computer using Statistical package for Social Science program (SPSS; version 15) software package under Windows Vista operating system.
Student t test was used to assess the statistical significance of the difference between 2 population means in a study involving independent samples. Analysis of variance was used to test the difference about mean values of some parameters among multiple groups. Comparison of the effect of CK-MB on NSTEMI patients' fate was analyzed using nonparametric tests (Mann-Whitney). Pearson and Spearman correlation analyses were used to assess the strength of association between 2 quantitative variables. Chi-square test χ 2 and Fisher exact test were used to test the categorical variables. P < .05 was considered the cutoff value for significance.
Results
The results of the present study are shown in Tables 1 and 2. Group I patients showed statistically significant lower baseline CADP PFA-100 CT than group II and healthy control group (77.6 ± 20.4, 87.60 ± 10.2, and 86.2 ± 8.9 seconds, respectively; t = 2.057, P = .04 and t = 2.154, P = .03, respectively); however, group II showed no statistically significant difference from the healthy control group (t = .513, P = .6). Neither age nor gender showed statistically significant relation with baseline CADP PFA-100 CT (P = .3 and .4, respectively). In addition, none of the studied risk factors showed statistical significant relation with baseline CADP PFA CT (P > .05). The severity of coronary artery disease (CAD) was established based on the number of coronary vessels affected. Coronary angiography revealed the presence of single-vessel disease in 24 patients, 2-vessel disease in 30 patients, and 3-vessel CHD in 6 patients, with statistically significant difference in the baseline CADP PFA-100 CT (P = .02; Table 1).
Association Between CADP PFA-100 CT and Clinical Data in the Studied Patients.
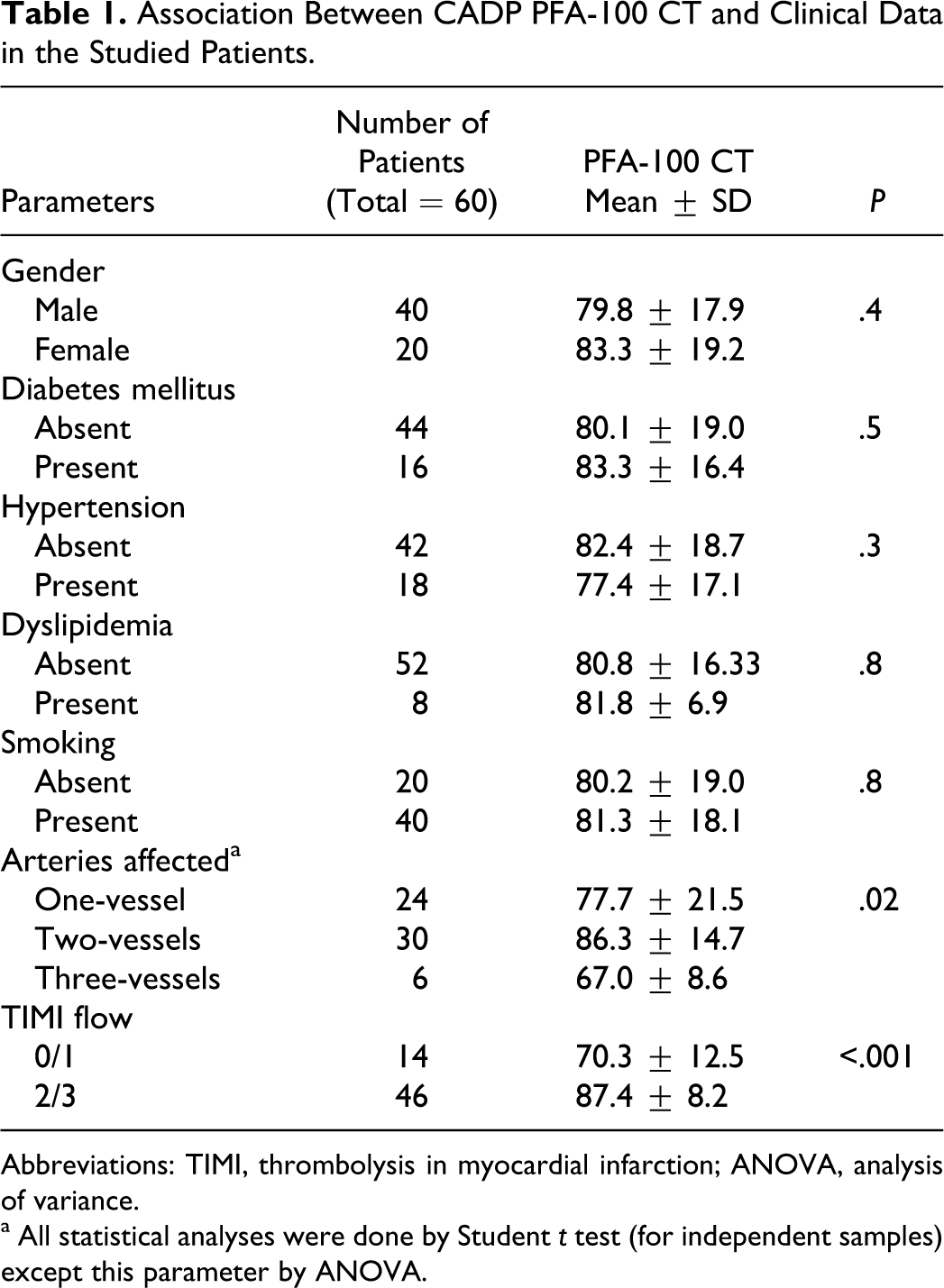
Abbreviations: TIMI, thrombolysis in myocardial infarction; ANOVA, analysis of variance.
a All statistical analyses were done by Student t test (for independent samples) except this parameter by ANOVA.
Impact of Different Factors on the Fate of the Patients With NSTEMI.
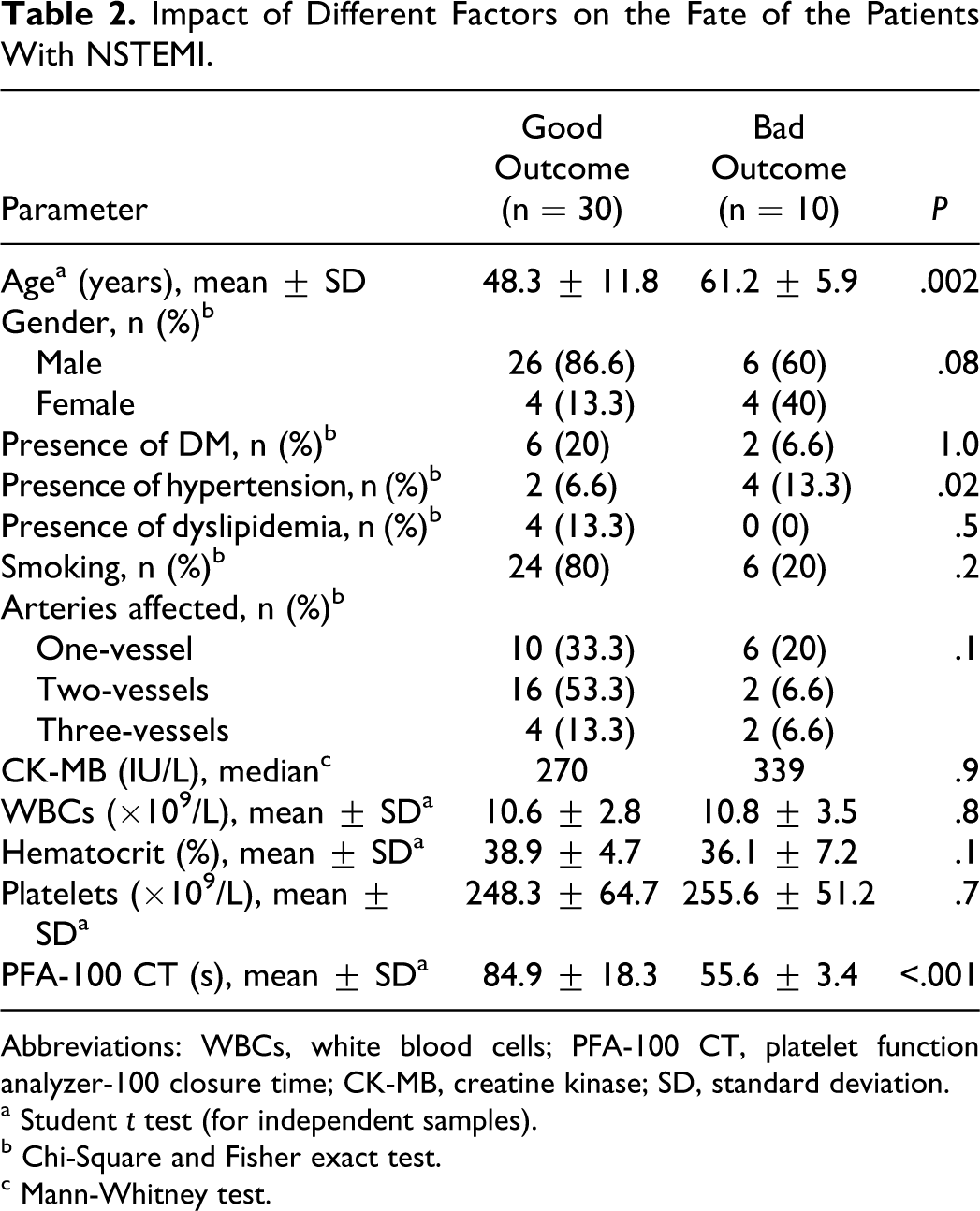
Abbreviations: WBCs, white blood cells; PFA-100 CT, platelet function analyzer-100 closure time; CK-MB, creatine kinase; SD, standard deviation.
a Student t test (for independent samples).
b Chi-Square and Fisher exact test.
c Mann-Whitney test.
The culprit artery lesion was further evaluated according to its morphology and divided into 2 groups: type A lesion (simple lesion) as 1 group and types B and C lesions (complex lesions) as another group. Group I included 24 patients with type C, 8 patients with type B, and 8 patients with type A lesion. Group II included 8 patients with type C, 5 patients with type B, and 7 patients with type A lesion with statistically nonsignificant difference between the 2 groups (P = .2). Intracoronary thrombus in the culprit artery was found in 20 patients in group I compared with 7 patients in group II (P = .2). Regarding the TIMI flow in the culprit artery; in group I, 12 patients had TIMI flow 0/1 and 28 patients had TIMI flow 2/3, but in group II, only 2 patients had TIMI flow 0/1 and 18 patients had TIMI flow 2/3 (P = .1). However, the initial TIMI flow grading system shows a statistically significant difference regarding baseline CADP PFA-100 CT being lower in TIMI 0/1 patients than in TIMI 2/3 patients (Table 1).
The correlation between baseline CADP PFA-100 CT and CK-MB level at hospital admission in NSTEMI patients was statistically non-significant (P = .9). Besides, statistically nonsignificant correlations were found between baseline CADP PFA-100 CT and white blood cell count, hematocrit value, and platelet count (P = .3, .4, .3, and .8, respectively).
As regards the impact of different factors on the outcome of the patients with MI, the occurrence of complications in NSTEMI patients were associated with older age, hypertension, and shorter baseline CADP PFA-100 CT (P < .05; Table 2).
Discussion
Platelet activation is implicated in the genesis of ACS. 13 In this study, we found that NSTEMI patients proved to have enhanced baseline platelet function (before intake of antiplatelet drugs) than patients with UA and normal control group. This is in accordance with Frossard et al 10 who studied 212 aspirin-pretreated and aspirin-naive patients with symptoms suggestive of ACS using both CEPI and CADP. This could be explained by that MI initiation due to the disruption of the atheromatous plaque with subsequent exposure of core constituents such as lipids, smooth muscles, and foam cells leads to local generation of thrombin and deposition of fibrin. This in turn promotes platelet activation. 14
In accordance with Carcao et al 15 and Sestito et al 16 who studied apparently healthy individuals, no relation was found between baseline PFA-100 CADP-CT and either age or gender of the patients in this study. Moreover, inline with other studies,5,10,17 we found nonsignificant associations between baseline PFA-100 CADP CT and diabetes mellitus, hypertension, dyslipidemia, and smoking. This could be due to the proper control of these risk factors by routine medical treatment. However, further studies on the effect of this treatment on the baseline platelet function assessed by PFA-100 CT are needed.
Regarding the association between the baseline PFA CT and CAD severity as assessed by the number of blood vessels affected, in contrast to Rosiak et al, 17 we found significant difference regarding PFA-100 CADP-CT between patients with 1-, 2-, and 3-vessel disease where patients with 3-vessel disease had the shortest CT. This is because they used PFA-100 to monitor the effectiveness of antiplatelet therapy.
As for the correlation between baseline PFA-100 CADP-CT, hematocrit, leucocyte count, and platelet count, we did not find significant correlations between PFA-100 CADP-CT and the above-mentioned parameters. However, it should be noted that low hematocrit and low platelet counts were exclusion criteria for our patients. In fact, all these parameters may affect the PFA-100 CT, particularly when levels fall below normal. 18
In our study, regarding the predictive value of baseline PFA-100 CADP-CT on the degree of myocardial necrosis, we found insignificant correlation between baseline PFA-100 CADP-CT and serum level of CK-MB in NSTEMI patients. On the contrary, Frossard et al 10 found that both CADP-CT and CEPI-CT were predictive of the degree of myocardial necrosis as measured by the peak levels of CK-MB and troponin-T. This could be explained by that assessing CK-MB was done in our patients during hospital admission, and it was impossible to obtain the blood samples exactly at the same time for all participants.
In this work, the baseline PFA-100 CADP-CT could predict the negative outcome in patients with ACS; the shorter the baseline PFA-100 CADP-CT, the more liable the development of complications. This is in line with Fuchs et al 5 and Gianetti et al 19 who used both CEPI and CADP cartridges, and they found significant association between platelet function and the development of adverse cardiovascular events during the follow-up period despite antiplatelet drugs intake. The CEPI cartridge is similar to CADP but differs in being highly sensitive to aspirin therapy. 9
Study Limitation
One limitation of the present study, which deserves consideration is the assessment of baseline platelet function in patients taking medications for control of risk factors. Although there were no available research for their effect on baseline PFA-100 CT till now and almost all studies for assessment of platelet function in patients with ACS could not exclude the intake of these drugs, however, further studies could provide additional information.
It is worth noting that the relatively small sample size particularly with complex subgroup analysis as in patients with dyslipidemia and those with 3-vessel affection warrants further studies on larger number of patients.
We concluded that NSTEMI patients proved to have enhanced baseline platelet function that can be used as a predictor of the outcome. Correct identification of patients with increased baseline platelet activation may enable implementation of alternative treatment strategies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.