
Abstract
Paradoxical embolization is an uncommon but devastating complication of pulmonary embolism (PE). Awareness of this complication with prompt recognition and treatment could serve to preclude significant disability and death. Described is a case of PE associated with paradoxical embolism to the arteries of both upper extremities. While patent foramen ovale (PFO) is common, paradoxical embolism is infrequent but can involve almost any artery of the body. Discussed are the risk factors, clinical presentations, and diagnostic and treatment options for paradoxical embolism. Awareness of the potential for paradoxical embolization in patients with PE is essential to its prompt recognition and treatment.
Keywords
Introduction
Pulmonary embolism (PE) is an important problem in hospitalized patients. Thrombi within the pelvis and lower extremities are usually the source of emboli. With the elevation of right heart pressures resulting from PE, a patent foramen ovale (PFO) can transiently open and permit emboli to pass directly from the systemic venous to the systemic arterial circulation. Knowledge of the potential for this catastrophic complication can facilitate the prompt diagnosis and treatment of serious morbid events such as stroke, myocardial infarction, bowel ischemia, and gangrene of the extremities. We report a case of paradoxical pulmonary emboli which resulted in arterial occlusions in both upper extremities.
Case report
A 53-year-old male with a recent diagnosis of squamous cell carcinoma of the oropharynx underwent neoadjuvant chemotherapy and radiation treatment which was complicated by severe mucositis. A percutaneous endoscopic gastrostomy tube was placed to supplement inadequate oral intake. Two days postoperatively, he acutely developed nausea, dyspnea, left arm numbness and mottling, and reduced radial pulses bilaterally. An EKG demonstrated sinus tachycardia and a new right bundle brunch block. A computed tomographic angiography (CTA) scan of the chest revealed bilateral pulmonary emboli (Figure 1) and enlargement of the right ventricle (RV) with flattening of the interventricular septum. The patient was transferred to the intensive care unit for monitoring and anticoagulation and he remained hemodynamically stable. To investigate the new finding of decreased radial pulses, angiography of the aorta and upper extremities was performed and revealed an occlusion at the level of the left axillary artery with no distal reconstitution as well as occlusion of the right proximal brachial artery with reconstitution of flow at the distal brachial artery (Figure 2). The patient then underwent a successful catheter-directed thrombectomy of the upper extremity occlusions. Doppler ultrasound of his lower extremities demonstrated the presence of a right external iliac, femoral and popliteal deep vein thrombosis. A transthoracic echocardiogram (TTE) with contrast bubble study confirmed RV enlargement with severely reduced RV systolic function, right atrial dilatation, and a right-to-left shunt via a PFO. The patient underwent a percutaneous PFO closure with a Cardio SEAL occluder, had an insertion of inferior vena cava (IVC) filter, and was discharged home 8 days after the event on aspirin and enoxaparin. He returned to work 3 months after discharge.

Computed tomographic angiography of the chest showing clots in both pulmonary arteries.
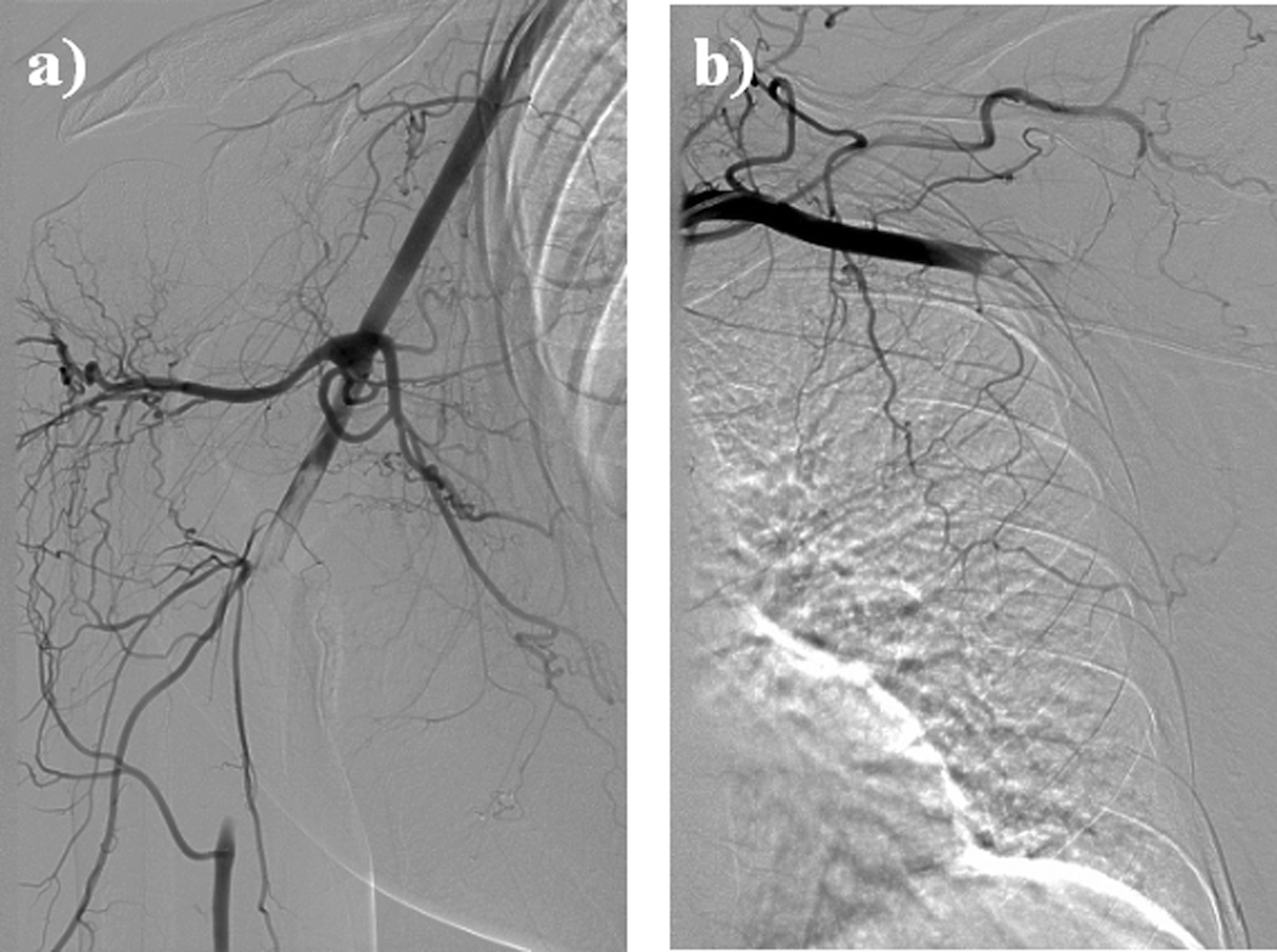
Angiography of both upper extremities showing (a) occlusion of the proximal right brachial artery with reconstitution of the flow at the level of the distal brachial artery and (b) occlusion of the left axillary artery with no reconstitution distally.
Discussion
The term paradoxical embolism refers to an arterial embolism that originates not from the systemic arterial circulation but paradoxically from the venous circulation. Clot transfer to almost any artery in the body usually occurs via an intracardiac communication (PFO or atrial septal defect) or intrapulmonary shunt. 1
Triggers and predisposing factors
Despite the high incidence of PFO (27.3% by autopsy), 2 paradoxical embolization is uncommon. The foramen ovale is most often physiologically closed by the left-to-right atrial pressure gradient, suggesting a requisite increase in right atrial pressure for the right-to-left shunt and interatrial passageway to occur. Not all patients with pulmonary thromboembolic disease and a PFO will develop paradoxical embolism. Indeed, other triggers and predispositions may well be involved. One trigger may be defecation, as suggested by reports of paradoxical embolism occurring during bathroom activities 1 and the associated Valsalva maneuvers. Another predisposing factor is a persistent Eustachian valve (EV) which may prevent closure of the foramen ovale and thus increase the risk for paradoxical embolization. 3 The EV is an endocardial fold at the junction of the IVC and right atrium that helps to direct blood flow to the foramen ovale and away from the tricuspid valve during fetal life. The EV typically regresses in postnatal life; however, it can persist in about 30% of adults in general and in 68% of patients with cryptogenic stroke. 3 The EV and PFO often co-exist in adulthood. 3
The presence of an atrial septal aneurysm (ASA; a significant bulging of the atrial septum through the fossa ovalis into the right atrium, left atrium, or both 4 ) in the setting of a PFO can increase the magnitude of shunting in patients with PE and has been suggested not only as a risk factor for paradoxical embolism 5 but also for refractory hypoxemia with PE. 5 Atrial septal aneurysms have been described in 0.2% to 4% of unselected patients undergoing transesophageal echocardiography but in 4% to 15% of patients with stroke. 6 Both PFO and ASA were significantly and synergistically associated with cryptogenic stroke. 6 The diameter of the PFO itself may be another independent risk factor for ischemic events. 7
While some case reports suggest that a PFO can potentially reduce clot burden in the pulmonary arteries and prevent massive PE, 8 the presence of a PFO is considered a risk factor for mortality in PE. One prospective study exploring the outcomes in patients with major PE showed increase in mortality (33% vs 14%), incidence of ischemic stroke (13% vs. 2.2%), and peripheral arterial embolism (15 vs. 0%) in patients with PFO compared to a control group with negative bubble echocardiography. 9 Another study noted that patients with hemodynamically significant PE in the setting of a PFO are more likely to have arterial hypoxemia, vascular occlusions, and an increased need for mechanical ventilation and vasopressor therapy; 10 despite these morbidities, no significant difference in the mortality from PE was noted between patients with and without a PFO.
Diagnosis
In order to make a presumptive diagnosis of paradoxical embolism, the clinician needs to detect (1) a venous thrombosis or PE, (2) an arterial thrombosis, and (3) a right to left communication. At the current time, echocardiography is not routinely recommended in the evaluation of the hemodynamically stable patient with PE; however, it can be useful as a risk assessment tool in helping to identify right ventricular dysfunction, pulmonary hypertension, PFO, and free-floating right-heart thrombi. 11 Goldhaber 11 has suggested that the finding of an increased right atrial pressure in the setting of PE should prompt evaluation for a PFO. A bubble TTE, bubble transesophageal echocardiogram (TEE) coupled with Valsalva maneuver, and transcranial dopplers (TCD) have been used in the identification of intracardiac right-to-left shunt. Di Tullio etal 12 adopted bubble TEE as the “gold standard” in detecting PFO and described a 68% sensitivity and 100% specificity of TCD, and only 47% sensitivity and 100% specificity of bubble TTE. Other authors, however, suggest that contrast TTE is sufficient in the evaluation of right-to-left shunt. 13 It is important to properly perform the Valsalva maneuver with image capturing not only before and during bubble injection but also during the release of the Valsalva when there is a transient rise in the right atrial pressure. 13
Multidetector CTA has largely replaced pulmonary angiography as the reference standard in the diagnosis of acute PE. 14 Computed tomographic angiography can not only detect PE but can also occasionally identify systemic arterial thrombi, thus facilitating the diagnosis of paradoxical embolism. 15 The presence of a PFO can result in insufficient contrast enhancement of the pulmonary artery along with a premature and intense enhancement of the thoracic aorta in deep inspiration scans. 15 Such an observation should alert the radiologist and clinician to the possibility of an intracardiac shunt. Computed tomographic angiography can also identify predisposing conditions for paradoxical embolism such as ASA as well as signs of RV overload (increased RV/LV ratio, interventricular septal shift, IVC contrast reflux, and enlargement of the IVC, azygos vein, or right atrium). 16
Treatment
The treatment of paradoxical embolism typically consists of anticoagulation, thrombolysis or thrombectomy, and the insertion of an IVC filter if otherwise indicated. From the available literature, it is not clear whether an intervention to close the PFO is obligatory; however, it would seem a reasonable option in selected patients at high risk for thrombosis recurrence. Traditionally, PFO repair was done surgically and surgical repair remains an option when patients are taken for open thrombectomy. Currently, paradoxical embolization is one of the most commonly accepted indications for percutaneous PFO closure which is minimally invasive, permits rapid recovery, and carries low risk of complications. 17
The detection of thrombi entrapped in the PFO during life is rare. 18 When this is found simultaneously with arterial embolism, it makes a definitive diagnosis of paradoxical embolism, otherwise, it is termed impending paradoxical embolism. How to deal with the clot straddling the PFO is an open question and recent review has been published. 18 Most case reports of such impending paradoxical embolism describe a surgical approach to the treatment. Thrombolysis was more frequently chosen over surgery in the higher risk group and in such cases was associated with greater mortality. 18 One concern with thrombolysis is the fragmentation of clot and the peripheral migration of emboli. 19 In patients with a contraindication to surgery or thrombolysis, success has been reported with unfractionated heparin. 18 Occasionally, clot trapped in PFO does not cause any ill effects and resolves without intervention. 20
Conclusion
We described a case of paradoxical embolism with resultant arterial occlusions in the upper extremities. Prompt recognition and treatment in our patient helped to prevent serious disability and possibly mortality. Despite the infrequency of this complication and the absence of uniform guidelines on management, an awareness of paradoxical embolization is critical for early diagnosis and treatment.
Footnotes
Acknowledgments
The authors thank Stephen Smith MB, BS, PhD, Division of Pulmonary & Critical Care Medicine, OHSU.
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.