
Abstract
Background
Heart failure (HF) is common among older adults; however, data on phenotype distribution and real-world pharmacologic management remain limited. This study assessed the prevalence of guideline-directed medical therapy (GDMT) underuse across HF phenotypes and identified factors associated with GDMT underuse among older outpatients in Vietnam.
Methods
In this multicenter cross-sectional study, 504 outpatients aged ≥60 years with HF were enrolled. Patients were classified into HF with reduced ejection fraction (HFrEF), mildly reduced ejection fraction (HFmrEF), and preserved ejection fraction (HFpEF). HFmrEF and HFpEF were combined as a non-HFrEF group for analysis. Multivariable logistic regression was performed to identify factors independently associated with GDMT underuse.
Results
HFrEF, HFmrEF, and HFpEF accounted for 54.6% (n = 275), 13.3% (n = 67), and 32.1% (n = 162) of patients, respectively. GDMT underuse was observed in 49.8% of patients with HFrEF and 38.0% of those with non-HFrEF phenotypes. In HFrEF, hypertension was associated with lower GDMT underuse (odds ratio [OR] 0.38; 95% confidence interval [CI] 0.15-0.98), whereas chronic obstructive pulmonary disease (COPD) was associated with higher underuse (OR 4.42; 95% CI [1.38-14.2]). In non-HFrEF, diabetes mellitus was independently associated with lower GDMT underuse (OR 0.52; 95% CI [0.30-0.91]).
Conclusion
In this study, GDMT underuse was observed in nearly half of patients with HFrEF and over one-third of those with non-HFrEF phenotypes. In HFrEF, hypertension was associated with lower GDMT underuse and COPD with higher GDMT underuse, whereas in non-HFrEF, diabetes mellitus was independently associated with lower GDMT underuse.
Keywords
Introduction
Heart failure (HF) is a complex clinical syndrome associated with high morbidity and mortality, particularly among older adults. It substantially impairs functional capacity and quality of life, imposing a major burden on healthcare systems worldwide.1–3 HF is commonly classified according to left ventricular (LV) ejection fraction (LVEF) into three phenotypes: HF with reduced ejection fraction (HFrEF, LVEF ≤40%), HF with mildly reduced ejection fraction (HFmrEF, LVEF 41-49%), and HF with preserved ejection fraction (HFpEF, LVEF ≥50%). 4 This classification is essential for determining appropriate therapeutic strategies.4–7
Globally, HF affects an estimated 64 million individuals. 3 Although incidence rates have stabilized, prevalence continues to rise owing to improved survival and increased life expectancy. 8 More than two-thirds of patients with HF have multiple comorbidities, which exacerbate disease burden, impair quality of life, and increase the risks of hospitalization and mortality.9,10 Among adults aged 60 to 79 years, the prevalence of HF is approximately 6%, rising to nearly 11% among those aged 80 years or older. 11 Age-related risk factors, including hypertension, coronary artery disease, and diabetes, together with structural and functional cardiac changes, contribute to this increasing prevalence. 12 Furthermore, HF in older adults is frequently accompanied by frailty, cognitive impairment, and malnutrition, all of which complicate disease management and worsen clinical outcomes. 13
Managing HF in older adults remains a major clinical challenge. Current guideline recommendations are largely derived from clinical trials conducted in broader populations, thereby limiting their applicability to older patients. 14 Although novel pharmacologic therapies have demonstrated clinical benefits, evidence specific to older adults remains limited, and real-world implementation of guideline-directed medical therapy (GDMT) appears suboptimal.15,16 Concerns about drug safety, polypharmacy, and the underrepresentation of older adults in clinical trials may further limit optimal therapy. 17 In Vietnam, data on the epidemiology and treatment patterns of HF among older adults remain scarce. Therefore, this study aimed to determine the prevalence of GDMT underuse across HF phenotypes and to identify factors associated with GDMT underuse among older Vietnamese outpatients.
Materials and Methods
Study Design, Participants, and Data Collection
This multicenter cross-sectional study enrolled outpatients aged ≥60 years with a confirmed diagnosis of chronic HF from three cardiology clinics in Ho Chi Minh City, Vietnam: Thong Nhat Hospital, Military Hospital 175, and the University Medical Center. No longitudinal follow-up or assessment of clinical outcomes was performed. Patient recruitment was conducted between August 2024 and March 2025. Exclusion criteria included active malignancy, severe psychiatric disorders, or incomplete data. Clinical information was obtained through structured face-to-face interviews and a review of electronic medical records. All participants provided written informed consent prior to enrollment.
Sociodemographic and Geriatric Characteristics
Sociodemographic data were collected, including age, sex, and residential status. Body mass index (BMI) was categorized into four groups according to the World Health Organization guidelines for the Asia-Pacific region: underweight (<18.5 kg/m2), normal weight (18.5-22.9 kg/m2), overweight (23.0-24.9 kg/m2), and obese (≥25 kg/m2). 18 Functional status was assessed using the Katz Index of Activities of Daily Living (ADL) and the Lawton Instrumental ADL (IADL) scale. Participants were considered to have limitations in ADL or IADL if they reported difficulty performing at least one activity in either domain.19,20 Frailty was evaluated using the Program of Research to Integrate Services for the Maintenance of Autonomy 7 questionnaire, with a total score ≥3 indicating frailty. 21 Depression was assessed using the 15-item Geriatric Depression Scale, with a score ≥5 indicating depressive symptoms. 22 All geriatric assessments were conducted by trained geriatricians to enhance consistency and reliability.
Characteristics and Treatment of HF
HF was diagnosed according to the criteria of the European Society of Cardiology (ESC). 4 The New York Heart Association (NYHA) functional classification was assessed for all participants. Echocardiographic examinations were performed and interpreted by experienced cardiologists following established guidelines. 23 To reduce measurement variability, all echocardiographic results were independently reviewed by a second cardiologist, and all study sites used the same echocardiographic system (EPIQ 7C, Philips Healthcare). LVEF was calculated using Simpson's biplane method, and HF was categorized into three phenotypes based on LVEF. LV dilation and left atrial enlargement were defined as an LV internal diameter in diastole >55 mm and a left atrial diameter >40 mm, respectively. LV hypertrophy was identified when the LV mass index exceeded 115 g/m2 for men and 95 g/m2 for women. Pulmonary artery systolic pressure (PASP) and moderate-to-severe functional mitral regurgitation were also evaluated.
HF medications were documented based on participants’ current prescriptions at enrollment. Quadruple therapy was defined as the concurrent use of one renin–angiotensin system inhibitor (either an angiotensin-converting enzyme inhibitor [ACEI], angiotensin II receptor blocker [ARB], or angiotensin receptor–neprilysin inhibitor [ARNI]) combined with a beta-blocker, mineralocorticoid receptor antagonist (MRA), and sodium–glucose cotransporter-2 inhibitor (SGLT2 inhibitor). GDMT was defined as quadruple therapy for participants with HFrEF and the use of an SGLT2 inhibitor for those with HFmrEF or HFpEF, in accordance with contemporary guideline recommendations.5,6 In this study, “underuse” was defined as the absence of these recommended pharmacologic components at the time of assessment, irrespective of dose intensity, target dose achievement, titration status, treatment duration, or documented contraindications.
Sample Size Calculation
The sample size was calculated using a single population proportion formula: n = (Z1−α/2)2×p(1 − p)/d2, where n is the required sample size, Z1−α/2 = 1.96 (for α = 0.05, corresponding to a 95% confidence level), and d is the margin of error (set at 0.045). The value of P was set at .5 to yield the maximum variance, P(1 − P) = 0.25. With a 5% allowance for missing data, the minimum required sample size was 498 participants.
Statistical Analysis
Baseline characteristics were summarized as frequencies and percentages for categorical variables and as mean ± standard deviation (SD) or median (interquartile range [IQR], 25th-75th percentile) for continuous variables, as appropriate. The Shapiro–Wilk test was used to assess the normality of continuous variables. Categorical variables were compared using the chi-square test or Fisher's exact test, as appropriate. Continuous variables were compared using one-way analysis of variance (ANOVA) or the Kruskal–Wallis test, depending on the data distribution. To identify factors associated with GDMT underuse, patients with HFmrEF and HFpEF were combined into a single non-HFrEF group, as these phenotypes share similar management strategies.5,6 Logistic regression analyses were performed to assess factors associated with GDMT underuse. Variables with a P-value <.05 in univariable analyses were considered for inclusion in the multivariable logistic regression models. All analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). A two-sided P-value <.05 was considered statistically significant.
Results
Among the 516 older patients with HF screened during the study period, 12 were excluded due to missing responses (n = 2), active malignancy (n = 6), severe psychiatric disorders (n = 3), or refusal to participate (n = 1). The study design and participant flow are presented in Figure 1. The final analysis included 504 older outpatients with HF, with a median age of 70 years (IQR 65-79; range, 60-94 years). The overall prevalence of HFrEF, HFmrEF, and HFpEF was 54.6% (n = 275), 13.3% (n = 67), and 32.1% (n = 162), respectively. GDMT underuse was observed in 49.8% of patients with HFrEF and 38.0% of those with non-HFrEF phenotypes.

Study design and participant flow.
Baseline characteristics stratified by HF phenotype are presented in Table 1. Median BMI increased across phenotypes, with values of 21.6, 22.5, and 22.9 kg/m2 in patients with HFrEF, HFmrEF, and HFpEF, respectively (P < .001). Geriatric impairments, including limitations in ADL and IADL, depression, and frailty, were most prevalent among patients with HFrEF. Significant differences were observed among the three phenotypes in the prevalence of diabetes mellitus, prior myocardial infarction, chronic coronary syndromes, atrial fibrillation, anemia, and renal dysfunction. No significant differences were observed in age, sex, or residential area.
Baseline Characteristics of Patients Stratified by Heart Failure Phenotype.
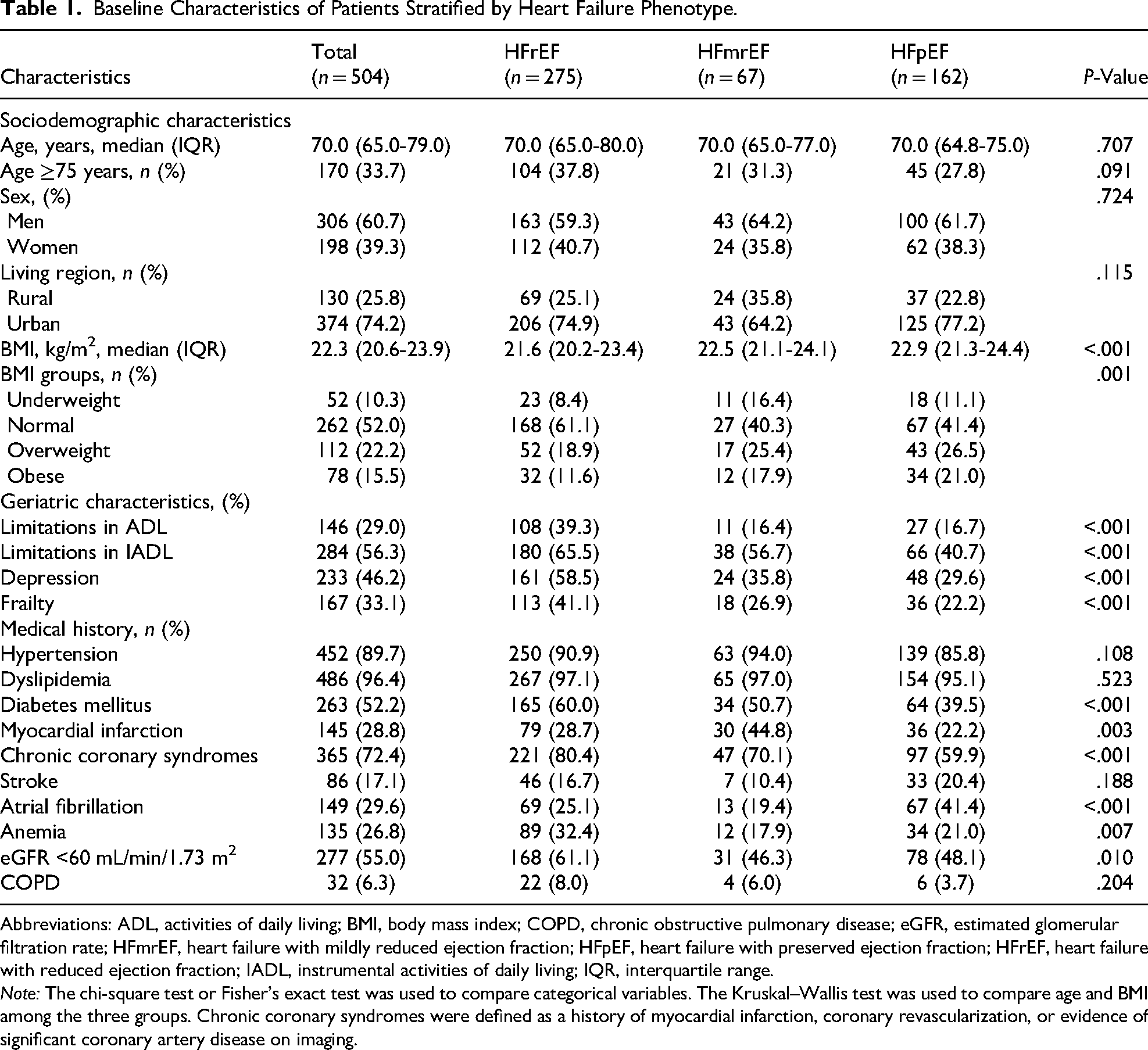
Abbreviations: ADL, activities of daily living; BMI, body mass index; COPD, chronic obstructive pulmonary disease; eGFR, estimated glomerular filtration rate; HFmrEF, heart failure with mildly reduced ejection fraction; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; IADL, instrumental activities of daily living; IQR, interquartile range.
Note: The chi-square test or Fisher's exact test was used to compare categorical variables. The Kruskal–Wallis test was used to compare age and BMI among the three groups. Chronic coronary syndromes were defined as a history of myocardial infarction, coronary revascularization, or evidence of significant coronary artery disease on imaging.
Echocardiographic and treatment characteristics by HF phenotype are shown in Table 2. Patients with HFrEF had more severe functional limitation, with a higher proportion classified as NYHA class III, and higher N-terminal pro–B-type natriuretic peptide (NT-proBNP) levels than those with HFmrEF or HFpEF (P < .001). Regarding pharmacological treatment, ARNIs, MRAs, SGLT2 inhibitors, and loop diuretics (furosemide) were prescribed more frequently in the HFrEF group. In contrast, ACEIs or ARBs were more commonly used in patients with HFmrEF and HFpEF.
Clinical Characteristics and Treatment Patterns by Heart Failure Phenotype.

Abbreviations: ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; ARNI, angiotensin receptor–neprilysin inhibitor; HFmrEF, heart failure with mildly reduced ejection fraction; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; IQR, interquartile range; LA, left atrium; LVEF, left ventricular ejection fraction; LVH, left ventricular hypertrophy; MR, mitral regurgitation; MRA, mineralocorticoid receptor antagonist; NYHA, New York Heart Association; PASP, pulmonary artery systolic pressure; SGLT2 inhibitor, sodium–glucose cotransporter-2 inhibitor.
Note: The chi-square test was used to compare categorical variables. The Kruskal–Wallis test was used to compare NT-proBNP and LVEF among the three groups.
Factors associated with GDMT underuse are shown in Tables 3 and 4. In multivariable logistic regression analyses, hypertension was associated with lower GDMT underuse (odds ratio [OR] 0.38; 95% confidence interval [CI] 0.15-0.98; P = .045), whereas chronic obstructive pulmonary disease (COPD) was associated with higher GDMT underuse among patients with HFrEF (OR 4.42; 95% CI [1.38-14.2]; P = .012). Among patients in the non-HFrEF group, diabetes mellitus was independently associated with lower SGLT2 inhibitor underuse (OR 0.52; 95% CI [0.30-0.91]; P = .022).
Factors Associated With Quadruple Therapy Underuse Among Patients With HFrEF (n = 275).
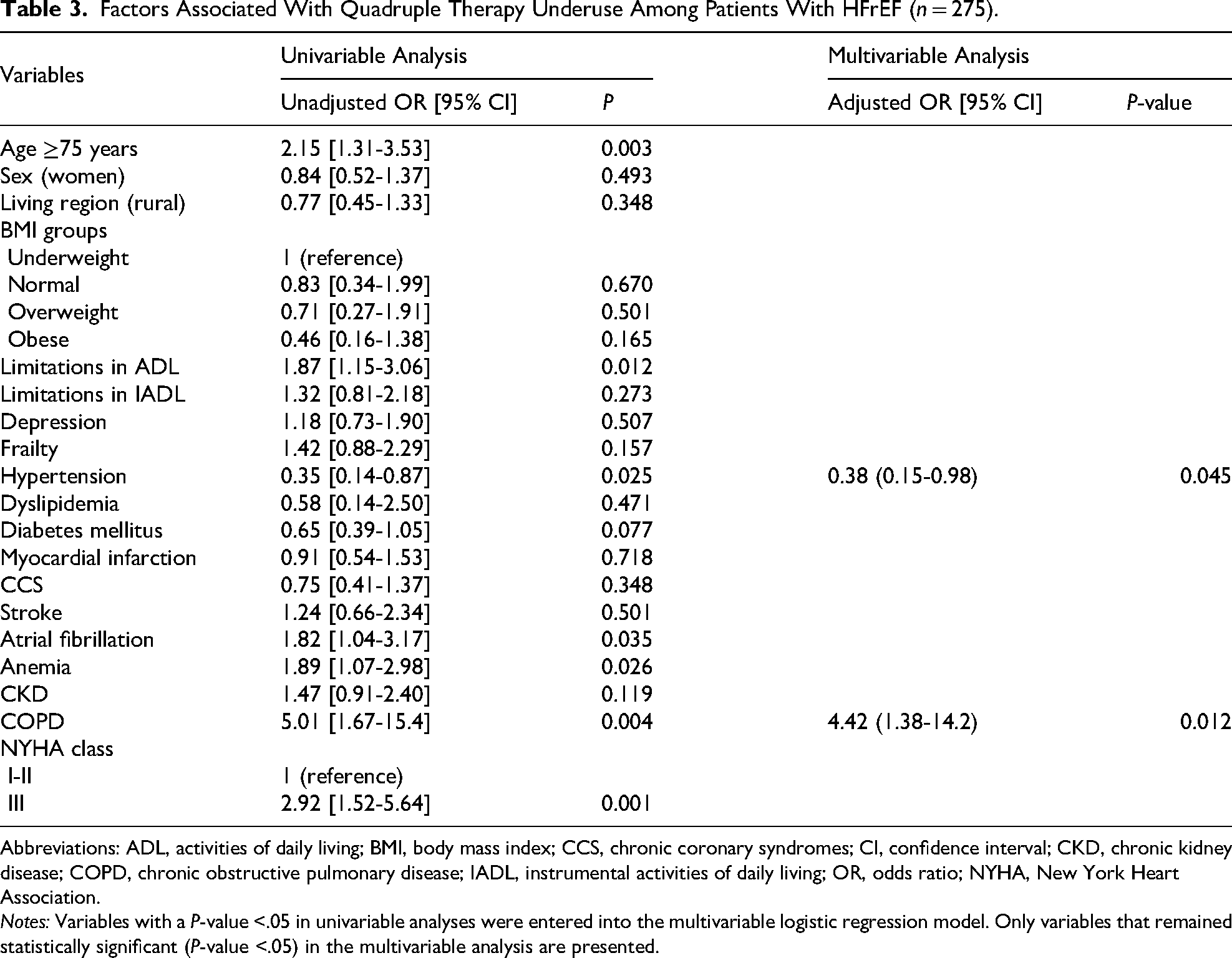
Abbreviations: ADL, activities of daily living; BMI, body mass index; CCS, chronic coronary syndromes; CI, confidence interval; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; IADL, instrumental activities of daily living; OR, odds ratio; NYHA, New York Heart Association.
Notes: Variables with a P-value <.05 in univariable analyses were entered into the multivariable logistic regression model. Only variables that remained statistically significant (P-value <.05) in the multivariable analysis are presented.
Factors Associated With SGLT2 Inhibitor Underuse Among Patients With Non-HFrEF (n = 229).

Abbreviations: ADL, activities of daily living; BMI, body mass index; CCS, chronic coronary syndromes; CI, confidence interval; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; IADL, instrumental activities of daily living; OR, odds ratio; NYHA, New York Heart Association.
Notes: Variables with a P-value <.05 in univariable analyses were entered into the multivariable logistic regression model. Only variables that remained statistically significant (P-value <.05) in the multivariable analysis are presented.
Discussion
This multicenter cross-sectional study describes HF phenotypes and treatment patterns among older outpatients in Vietnam. HFrEF was the most prevalent phenotype. GDMT underuse was observed in nearly half of patients with HFrEF and in more than one-third of those with non-HFrEF phenotypes. In HFrEF, hypertension was associated with lower GDMT underuse and COPD with higher GDMT underuse, whereas in non-HFrEF, diabetes mellitus was associated with lower GDMT underuse. These findings suggest phenotype-specific patterns of GDMT implementation in this older population.
HF Phenotype Distribution, Clinical Characteristics, and Treatment
The epidemiology of HF varies considerably across regions worldwide.2,3 Although most epidemiological data originate from Western and high-income countries, evidence from low- and lower-middle-income Asian nations, particularly among older patients, remains limited. 24 In Vietnam, our study identified a predominance of HFrEF, suggesting a relatively higher burden of systolic dysfunction among older Vietnamese patients with HF. This finding differs from previous reports describing a higher prevalence of HFpEF, particularly in older populations. 25 These discrepancies may reflect regional differences in comorbidity patterns and HF risk factors.
First, myocardial ischemia is a major etiology of HFrEF, 26 and ischemic heart disease remains a leading cause of HF in many Asian countries.27,28 Consistent with this, we observed a higher prevalence of chronic coronary syndromes among patients with HFrEF compared with those with HFmrEF or HFpEF. Second, prior epidemiological studies have demonstrated an association between obesity and HFpEF. 29 Although obesity was most prevalent among patients with HFpEF in our study, its overall prevalence was lower than that reported in previous studies of older HF populations. 30 This may partly explain why HFpEF was not the predominant phenotype in our study. Overall, these findings suggest that the distribution of HF phenotypes among older Vietnamese outpatients may be influenced by regional characteristics, with HFrEF being the most prevalent phenotype.
The clinical characteristics observed across HF phenotypes in this study showed distinct patterns. Patients with HFrEF more frequently presented with ischemic heart disease, diabetes mellitus, and chronic kidney disease, whereas those with HFpEF were more likely to be overweight or obese and exhibited a higher prevalence of atrial fibrillation. These trends are consistent with findings from large-scale HF registries, which have shown that higher LVEF is associated with greater burdens of obesity and metabolic syndrome. 31 In addition, our study demonstrated a high prevalence of geriatric syndromes that varied across HF phenotypes. Notably, patients with HFrEF exhibited greater functional and psychosocial vulnerability, which differs from previous studies reporting no significant differences in frailty or cognitive impairment between HFrEF and HFpEF. 32 This discrepancy may reflect population-specific differences, as frailty in Western studies is often linked to obesity among patients with HFpEF, a phenotype less common in Southeast Asian populations due to generally lower BMI and fat mass. 3 Given the substantial burden of multimorbidity and geriatric syndromes observed, a comprehensive and multidisciplinary approach to HF management may help optimize care for older patients.
Understanding the therapeutic landscape of HF in older patients suggests a gap between evidence-based recommendations and real-world practice. In this study, patients with HFpEF were less likely to receive ARNIs and MRAs compared with those with HFmrEF and HFrEF. This disparity may reflect the limited and inconclusive evidence supporting the clinical efficacy of these agents in HFpEF populations. 6 Moreover, the use of SGLT2 inhibitors was highest among patients with HFrEF and gradually declined across HFmrEF and HFpEF phenotypes. This pattern parallels the decreasing prevalence of diabetes mellitus across these subgroups and may also reflect historical prescribing patterns, as SGLT2 inhibitors were initially approved for glycemic control rather than HF-specific indications. Loop diuretics were most frequently prescribed in the HFrEF group, which may be related to the greater disease severity observed in these patients, as indicated by higher NT-proBNP concentrations and poorer NYHA functional class. Collectively, these findings underscore the importance of strategies aimed at enhancing GDMT implementation and promoting equitable delivery of evidence-based care in this older population.
Prevalence and Factors Associated With GDMT Underuse
Current clinical guidelines recommend quadruple therapy for patients with HFrEF and the use of SGLT2 inhibitors for those with HFmrEF and HFpEF to reduce HF-related morbidity and mortality.4–6 The STRONG-HF trial reported that early and intensive up-titration of guideline-recommended therapies was associated with improved clinical outcomes, supporting the potential prognostic relevance of timely optimization. 33 Moreover, recent pharmacologic analyses have supported early and parallel initiation of foundational therapies rather than delayed stepwise escalation.34,35
Despite these established benefits, the adoption of GDMT remains suboptimal worldwide. Data from the CHAMP-HF registry indicated that 27% to 67% of outpatients with HFrEF did not receive recommended therapies. 36 In a large U.S. study, only 3% of patients with HFrEF were prescribed quadruple therapy, and 4.7% of those with HFpEF received an SGLT2 inhibitor. GDMT utilization tended to be higher among patients with atherosclerotic cardiovascular disease or diabetes mellitus, whereas socioeconomic factors were not significantly associated. 37 Similarly, data from a Canadian administrative database showed that only one-fifth of older patients with HFrEF received triple therapy, with higher prescription rates observed among women, those younger than 80 years, individuals with fewer comorbidities, and patients managed in academic or rural healthcare settings. 38 Overall, barriers to optimal GDMT implementation appear multifactorial and may be broadly categorized into patient-related (eg, comorbidities), treatment-related (eg, adverse effects, contraindications), and healthcare system–related (eg, access to specialists, cost) factors.39–41 Addressing these barriers through targeted strategies may help improve the uptake and equity of evidence-based HF care, particularly in ageing and resource-limited populations.
Among older patients with HFrEF, our study found that hypertension was associated with a higher likelihood of receiving quadruple therapy, whereas COPD was associated with a lower likelihood. Hypertension is a major risk factor for the development of HFrEF in older patients. 42 In its early stages, hypertension primarily induces LV diastolic dysfunction, whereas progressive vascular remodeling, ischemic injury, and age-related myocardial changes may contribute to the development of LV systolic dysfunction over time.14,42 According to ESC hypertension guidelines, renin–angiotensin system inhibitors, such as ACEIs and ARBs, are recommended as first-line antihypertensive therapy. 43 These agents are also core components of quadruple therapy for HFrEF management. 5 This overlap in therapeutic indications may partly explain the higher use of quadruple therapy among hypertensive patients with HFrEF compared with those without hypertension (Supplemental Table S1). Conversely, the lower prescription of quadruple therapy in patients with COPD may be related to reduced use of beta-blockers in this population (Supplemental Table S1). Although the Global Initiative for Chronic Obstructive Lung Disease does not consider beta-blockers contraindicated in patients with COPD, 44 concerns regarding potential pulmonary adverse effects may influence prescribing practices.
Among non-HFrEF patients (ie, those with HFmrEF or HFpEF), diabetes mellitus was associated with greater use of SGLT2 inhibitors. Initially introduced for glycemic control, SGLT2 inhibitors are now recognized for their cardiovascular benefits across the HF spectrum, irrespective of diabetes status.45,46 The higher utilization of SGLT2 inhibitors among diabetic patients in our study may therefore reflect prescribing practices targeting both metabolic and cardiovascular considerations.
This study has several limitations that should be acknowledged. First, the sample size within each HF phenotype was relatively modest, particularly for patients with HFmrEF and HFpEF, which may limit statistical precision and generalizability. Second, information on medication dosage and up-titration strategies was not available, limiting the assessment of dose optimization and the dynamic process of GDMT implementation. Third, given the observational cross-sectional design, causal relationships cannot be inferred, and the specific reasons underlying GDMT underuse were not captured. Fourth, the etiology of HF was not definitively characterized due to its multifactorial nature and the high burden of comorbidities among older patients. Fifth, device-based therapies, such as cardiac resynchronization therapy implantation, as well as information on iron deficiency and its management, were not evaluated because of their limited availability in the study setting. Sixth, social determinants of health, including income, educational level, and healthcare access, were not assessed, although these factors may influence treatment patterns. Finally, as longitudinal follow-up was not performed, the association between GDMT implementation and clinical outcomes such as mortality or hospitalization could not be evaluated. Future prospective studies may help clarify the prognostic implications of GDMT across HF phenotypes in older patients.
Conclusions
To our knowledge, this study is among the first multicenter investigations to characterize the prevalence, clinical features, and factors associated with GDMT underuse across HF phenotypes among older outpatients in Vietnam. HFrEF was the predominant phenotype in this population. Among patients with HFrEF, hypertension was associated with lower GDMT underuse, whereas COPD was associated with higher GDMT underuse. In patients with non-HFrEF phenotypes, diabetes mellitus was independently associated with lower SGLT2 inhibitor underuse. These findings suggest potential areas for improving GDMT implementation in older patients, particularly through careful consideration of comorbid conditions that may influence prescribing practices.
Supplemental Material
sj-docx-1-cpt-10.1177_10742484261438177 - Supplemental material for Underuse of Guideline-Directed Medical Therapy Across Heart Failure Phenotypes in Older Outpatients: A Multicenter Cross-Sectional Study in Vietnam
Supplemental material, sj-docx-1-cpt-10.1177_10742484261438177 for Underuse of Guideline-Directed Medical Therapy Across Heart Failure Phenotypes in Older Outpatients: A Multicenter Cross-Sectional Study in Vietnam by Huan Thanh Nguyen, MD, PhD, Huong Thi Mai Nguyen, MD, MS, Kieu Dang Phuong Nguyen, MD, MS, and Duc Thien Tran, MD, MS in Journal of Cardiovascular Pharmacology and Therapeutics
Footnotes
Acknowledgments
The authors thank all participating patients and the clinical staff of Thong Nhat Hospital, Military Hospital 175, and the University Medical Center, Ho Chi Minh City, Vietnam, for their valuable support in patient recruitment and data collection.
Ethical Considerations
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. The study protocol was approved by the Ethics Committee of the University of Medicine and Pharmacy at Ho Chi Minh City (Reference No. 2049/DHYD-HDDD). All participants provided written informed consent prior to enrollment, and participant anonymity was maintained throughout data collection and analysis.
Consent to Participate
Written informed consent was obtained from all participants included in the study.
Consent for Publication
All participants provided consent for publication. All authors reviewed and approved the final version of the manuscript and agreed to its submission for publication.
Author Contributions
HTN designed the study; HTN, HTMN, and KDPN collected the clinical data, verified data accuracy, and performed the statistical analyses; HTN and DTT drafted and critically revised the manuscript. All authors read and approved the final manuscript.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request. 47
Supplemental Material
Supplemental material for this article is available online.