
Abstract
Background
In patients with heart failure (HF), loop diuretics (LD) are recommended to relieve congestion and may be de-escalated if symptoms improve. However, long-term use of the same LD dose is sometimes required owing to potential congestion exacerbation. Therefore, we investigated the factors associated with LD de-escalation in patients with acute decompensated HF (ADHF) and the relationship between this de-escalation and initiating guideline directed medical therapy (GDMT) during hospitalization.
Methods
In this retrospective cohort study, patients with ADHF who were prescribed LD and GDMT at discharge were included. The primary endpoint was LD de-escalation at 6 months post-discharge. Factors associated with this de-escalation were extracted using multivariate analysis. The Cochran–Armitage trend test was used to analyze the relationship between the number of GDMT initiated during hospitalization and LD de-escalation.
Results
Of 193 eligible patients, 40.4% underwent LD de-escalation. Significant de-escalation-associated factors were age <75 years (odds ratio, 2.114; 95% confidence interval, 1.125-3.972), body mass index (BMI) ≥ 22.0 kg/m2 (2.022; 1.073-3.811), and no atrial fibrillation (1.948; 1.047-3.625). The LD de-escalation rate tended to increase with the number of angiotensin receptor-neprilysin inhibitor, mineralocorticoid receptor antagonists, and sodium-glucose transporter 2 inhibitors initiated during hospitalization (P = .013).
Conclusion
Younger age, high BMI, and no atrial fibrillation were LD de-escalation-associated factors in patients with ADHF. LD de-escalation post-discharge may occur more frequently if the number of GDMT with diuretic effects was increased during hospitalization.
Keywords
Introduction
Heart failure (HF) affects more than 64 million people worldwide and 1.2 million people in Japan.1,2 Additionally, its incidence continues to increase.1,2 The 1-year rehospitalization and all-cause mortality rates of patients with acute HF were as high as 29.4% and 22.3%, respectively, with poor prognosis. 3
HF has a chronic and progressive clinical course and becomes more serious with repeated acute exacerbations. 4 Acute decompensated HF (ADHF) is a condition characterized by cardiogenic pulmonary edema or systemic fluid retention due to rapid worsening of HF, which often requires hospitalization.4,5
Treatment with guideline directed medical therapy (GDMT) for patients with ADHF is initiated after their condition has been stabilized.4,5 These drugs include angiotensin receptor-neprilysin inhibitor (ARNI), mineralocorticoid receptor antagonists (MRA), sodium-glucose transporter 2 inhibitors (SGLT2i), and beta-blockers, which have been shown to decrease the risk of hospitalization and improve left ventricular ejection fraction (LVEF).4–6 Additionally, loop diuretics (LD) are recommended to improve symptoms for patients with signs and/or clinical symptoms of congestion.4–8
However, LD use activates the renin-angiotensin-aldosterone system (RAAS) and worsens renal function.9,10 Reportedly, long-term use of LD is associated with a poor prognosis in patients with HF. 11 Therefore, LD de-escalation is considered when the signs and/or symptoms of congestion improve.4,5 However, some patients use LD long-term without de-escalation after discharge because of concerns about exacerbation of congestion.
In a previous study on patients with stable chronic HF, it was reported that high systolic blood pressure, absence of peripheral congestion, and severe valvular disease were factors associated with LD dose reduction. 12 However, in patients with ADHF, LD de-escalation-associated factors after discharge have not been investigated. Clarifying these factors may lead to appropriate LD de-escalation.
Among the GDMT, ARNI, MRA, and SGLT2i have diuretic effects through different mechanisms of action.13,14 Each of the 3 drugs has been shown to reduce the LD dose or decrease the rate of new LD initiation in patients with HF.15–17 However, the relationship between the initiation of these 3 drugs and the LD de-escalation after discharge has not been clarified. Clarifying this relationship in patients with ADHF may lead to appropriate LD de-escalation.
To support appropriate LD de-escalation after discharge, we investigated the factors associated with LD de-escalation in patients with ADHF and the relationship between the initiation of ARNI, MRA, and SGLT2i during hospitalization and LD de-escalation.
Methods
Study Design and Patients
The retrospective cohort study included 461 patients hospitalized with ADHF at the Department of Cardiology, Showa Medical University Fujigaoka Hospital, between November 2020 and December 2023. The inclusion criteria were as follows: (1) patients diagnosed with ADHF based on the criteria in the HF guidelines,4,5,8 (2) patients in all LVEF categories, (3) those prescribed any of the GDMT at discharge, and (4) those prescribed LD at discharge. The GDMT included renin-angiotensin system (RAS) inhibitors, such as angiotensin-converting enzyme inhibitors (ACEi), angiotensin receptor blockers (ARB), and ARNI; MRA; SGLT2i; and beta-blockers. We excluded patients (1) who died within 6 months after discharge, (2) whose endpoints after discharge were unknown, (3) who were on hemodialysis, (4) who underwent surgical treatment for valvular disease within 6 months after discharge, and (5) with estimated glomerular filtration rate (eGFR) > 200 mL/min/1.73 m2. After excluding 268 patients, 193 patients were included in the analysis (Supplemental Figure 1).
This study was approved by the Ethics Committee at Showa Medical University, Japan (Approval No. 2023-215-A), which waived the requirement for informed consent owing to the retrospective nature of this study. Patients were informed that they could opt out of having their data used for research purposes on the Showa Medical University Fujigaoka Hospital's website.
Treatment of HF
The cardiologist prescribed HF medications following treatment guidelines.4–8 Adjustments to GDMT and LD during hospitalization and after discharge were made at the physician's discretion based on the patient's condition. The GDMT were defined as RAS inhibitors (ACEi/ARB/ARNI), MRA, beta-blockers, and SGLT2i.4–8
Data Collection
Data on patient characteristics, HF severity classification, laboratory data, and medications were collected from the medical records. Patient characteristics included age, sex, HF etiology, comorbidities, and history of HF hospitalization. The LVEF categories, clinical scenario, and New York Heart Association (NYHA) classification were used to classify HF severity at admission. The LVEF categories were collected as HF with reduced ejection fraction (HFrEF), HF with mildly reduced ejection fraction (HFmrEF), and HF with preserved ejection fraction (HFpEF). 4 Physical findings at discharge included body mass index (BMI), heart rate, and systolic and diastolic blood pressure. Laboratory data at discharge included white blood cell, hemoglobin, hematocrit, albumin, uric acid, blood urea nitrogen (BUN), creatinine (Cre), sodium, potassium, eGFR, and brain natriuretic peptide (BNP) levels. Additionally, data on BNP, BUN, and eGFR levels were collected at 6 months after discharge.
Information on the use of RAS inhibitors, beta-blockers, MRA, and SGLT2i was collected at admission, discharge, and 6 months after discharge. Information on the LD dose and use was also collected at admission, discharge, and 6 months after discharge.
Endpoint
The primary endpoint was “LD de-escalation,” which was defined as a reduction or discontinuation of LD dose at 6 months after discharge compared with that observed at discharge. “LD no de-escalation” was defined as no change or increase of LD dose at 6 months after discharge compared with that observed at discharge. In patients with missing data at 6 months after discharge, data on the nearest outpatient visit date around 6 months after discharge were collected.
Furthermore, for patients who were re-hospitalized for HF before the primary endpoint evaluation, data were collected at 6 months following their initial discharge. Based on previous studies,15,16,18 the timing for evaluating LD de-escalation was set at 6 months after discharge. Additionally, since congestion could exacerbate within 3 months after discharge,19,20 6 months after discharge, when congestion is likely to have improved, was considered an appropriate time to evaluate LD de-escalation.
The secondary endpoint was the occurrence of cardiovascular events, defined as a composite of cardiovascular death and HF rehospitalization, during the follow-up period from discharge to July 31, 2024.
Statistical Analysis
Sample Size
We estimated that a sample size of 185 patients would be required to detect an odds ratio (OR) of 2.0, with 80% statistical power at a significance level of 0.05 in an equivalence test of the hypothesis, assuming the LD de-escalation rate to be 10%. 12 Therefore, the study sample size was sufficient to obtain a valid conclusion.
Stratification
For convenience in clinical use, the continuous variables were dichotomized and treated as categorical variables. Patients were divided into 2 groups based on the cutoff values using the World Health Organization's definition for age (75 years), systolic blood pressure (140 mm Hg), and hemoglobin (13 and 12 g/dL in males and females, respectively). Two groups were also divided based on BMI (cutoff: 22.0 kg/m2) following the Japan Society for the Study of Obesity definition, 21 heart rate (cutoff: 70 bpm) based on the HF guideline, 6 log BNP (cutoff: 2.46) using Youden's index method, eGFR (cutoff: 60 mL/min/1.73 m2) according to the chronic kidney disease guideline, 22 albumin (cutoff: 3.5 g/dL) using the reference value for low nutrition, 23 and BUN/Cre (cutoff: 20) according to common clinical practice. 24 Other laboratory data were divided into 2 groups based on the upper or lower limits of the reference range values for clinical items published by the Japanese Clinical Laboratory Standards Council. 25 LD doses were converted to furosemide equivalents, as follows: furosemide 40 mg = azosemide 60 mg = trasemide 8 mg. 4
Factors Associated With LD De-escalation
Categorical variables are expressed as numbers and percentages, and continuous variables as median (min-max). Patient characteristics, clinical findings, and laboratory data were compared between the LD de-escalation and no de-escalation groups. The chi-square or Fisher's exact test was used for univariate analysis, and significant variables were entered into the multivariate analysis. No correlations were found between these factors. Furthermore, as covariates, log BNP and albumin, which are related to HF prognosis, and BUN/Cre, which reflects the degree of circulating blood volume due to diuretics, were entered in the multivariate analysis. The analysis was performed using logistic regression. Independent and significant factors associated with LD de-escalation were extracted using the stepwise method. Missing values were not imputed in this study. Statistical significance was set at P < .05. Statistical analysis was performed using SPSS version 28 (IBM, Tokyo, Japan).
Relationship Between LD De-escalation and Cardiovascular Events
Cardiovascular events curves of the LD de-escalation and no de-escalation groups were constructed using the Kaplan–Meier method and compared using the log-rank test.
Changes in Cardiac and Renal Function After Discharge
Within each group (LD de-escalation and no de-escalation), changes in log BNP, BUN, and eGFR levels were compared at discharge and at 6 months after discharge using the Wilcoxon signed-rank test. Furthermore, all 3 indicators at 6 months after discharge were compared between the LD de-escalation and no de-escalation groups using the Mann–Whitney U-test.
Relationship Between Initiation of ARNI, MRA, and SGLT2i and LD De-escalation
The proportions of patients who initiated any of ARNI, MRA, and SGLT2i during hospitalization were compared between the LD de-escalation and the no de-escalation groups using the chi-square test or Fisher's exact test. Furthermore, a multivariate analysis was performed using logistic regression to examine whether ARNI, MRA, and SGLT2i initiation were independently associated with LD de-escalation. Age, atrial fibrillation, BMI, hematocrit, albumin, BUN/Cre, and log BNP were entered into the multivariate analysis as adjusted factors. Although beta-blockers do not have a diuretic effect, their use at discharge was entered into the multivariate analysis as an adjustment factor to examine the effect of their use on LD de-escalation. The relationship between the number of ARNI, MRA, and SGLT2i initiated during hospitalization and LD de-escalation was analyzed using the Cochran–Armitage trend test.
To assess whether patients maintained the same regimen after discharge, we investigated the proportion of patients who used the same GDMT regimen at discharge and at 6 months after discharge. Additionally, to examine the effect of regimen changes on LD de-escalation, the proportion of regimen changes was compared between the LD de-escalation and no de-escalation groups using the chi-square test. Regimen changes were evaluated by comparing GDMT used at discharge and at 6 months after discharge, and classified into 4 groups: regimen change owing to a decrease in the number of GDMT, regimen change while maintaining the same number of GDMT, no change in either the number of GDMT and the regimen, and regimen change owing to an increase in the number of GDMT. ACEi and ARB were classified as the same regimen.
Subgroup Analysis Based on LVEF
Subgroup analysis was performed based on LVEF categories: HFrEF, HFmrEF, and HFpEF. For each LVEF subgroup, patient characteristics, clinical findings, and laboratory data were compared between the LD de-escalation and no de-escalation groups. The chi-square or Fisher's exact test was used for univariate analysis, and significant variables were entered into the multivariate logistic regression analysis. Independent and significant factors associated with LD de-escalation were extracted using the stepwise method. Additionally, for each LVEF subgroup, the proportions of patients who initiated any of ARNI, MRA, and SGLT2i during hospitalization were compared between the LD de-escalation and the no de-escalation groups using the chi-square test or Fisher's exact test.
Results
Patient Characteristics
The patient characteristics are shown in Table 1. The median age was 77 years (min-max; 34-96), and 120 (62.2%) were male. There were 35 (18.2%) patients who had a history of HF hospitalization and 110 (57.0%) patients with LVEF < 40% at admission. The median BMI and BNP levels at discharge were 20.8 (13.2-45.5) kg/m2 and 251.9 (7.8-3211.9) pg/dL, respectively, and the furosemide equivalent dose at discharge was 20 (10-140) mg (Supplemental Table 1).
Baseline Patient Characteristics at Admission and Discharge.

Abbreviations: BMI, body mass index; BNP, brain natriuretic peptide; BUN/Cre, blood urea nitrogen to creatinine ratio; COPD, chronic obstructive pulmonary disease; CS, clinical scenario; eGFR, estimated glomerular filtration rate; HF, heart failure; HFmrEF, heart failure with mildly reduced ejection fraction; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association; WBC, white blood cell.
Endpoint
The primary endpoint was achieved in 78 (40%) patients (Supplemental Figure 1). Among them, 33 (17%) and 45 (23%), respectively, had their LD dose reduced or discontinued. Additionally, 11 patients were re-hospitalized for HF before the primary endpoint evaluation.
Comparison of Patient Characteristics Between the LD De-escalation and the No De-escalation Groups
The proportions of patients with age <75 years, BMI ≥ 22.0 kg/m2, absence of atrial fibrillation, and high hematocrit level at discharge were significantly higher in the LD de-escalation group than in the no de-escalation group (Table 2). The eGFR and BNP levels did not significantly differ between the 2 groups (Table 2). Furosemide equivalent dose at discharge was not significantly different between the 2 groups (median [min-max], LD de-escalation group vs no de-escalation group, 20 [10-80] vs 20 [10-140], P = .644).
Comparison of Patient Characteristics in the LD De-escalation and the No De-escalation Groups.

Abbreviations: BMI, body mass index; BNP, brain natriuretic peptide; BUN/Cre, blood urea nitrogen to creatinine ratio; COPD, chronic obstructive pulmonary disease; CS, clinical scenario; eGFR, estimated glomerular filtration rate; F, female; HF, heart failure; HFmrEF, heart failure with mildly reduced ejection fraction; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; LD, loop diuretics; LVEF, left ventricular ejection fraction; M, male; NYHA, New York Heart Association.
Factors Associated With LD De-escalation
In the multivariate analysis, age <75 years, BMI ≥ 22.0 kg/m2, and absence of atrial fibrillation were independent significant factors associated with LD de-escalation after discharge (Table 3).
Factors Associated With LD De-escalation After Discharge in Patients With ADHF.

Age, atrial fibrillation, BMI, hematocrit, albumin, BUN/Cre, Log BNP at discharge were entered into the multivariate analysis.
Abbreviations: ADHF, acute decompensated heart failure; β, beta coefficient; BMI, body mass index; BNP, brain natriuretic peptide; BUN/Cre, blood urea nitrogen to creatinine ratio; CI, coefficient interval; LD, loop diuretics; OR, odds ratio.
Relationship Between LD De-escalation and Cardiovascular Events
The rate of cardiovascular events was significantly lower in the LD de-escalation group than in the no de-escalation group (P = .045; Figure 1). The median follow-up period was 419 days (5-1314). Forty-one (21%) patients had cardiovascular events (cardiovascular deaths: 10 patients [5%]) during the follow-up period. The median time from discharge to a cardiovascular event occurring was 214 days (5-916).

Cardiovascular events curves for patients with ADHF in the LD de-escalation and no de-escalation groups.
Changes in Cardiac and Renal Function After Discharge
In the LD de-escalation group, log BNP at 6 months after discharge was significantly lower than that at discharge (Table 4). In the no de-escalation group, BUN at 6 months after discharge was significantly higher than that at discharge, whereas no significant change was observed in the LD de-escalation group. In the no de-escalation group, eGFR at 6 months after discharge was significantly lower than that at discharge, whereas no significant change was observed in the LD de-escalation group.
Changes in Cardiac and Renal Function After Discharge in Patients With ADHF.

Abbreviations: ADHF, acute decompensated heart failure; BNP, brain natriuretic peptide; BUN, blood urea nitrogen; eGFR, estimated glomerular filtration rate; LD, loop diuretics.
P values for comparison at discharge and 6 months after discharge within the same group (Wilcoxon signed-rank test).
P values for comparison between the LD de-escalation and no de-escalation groups at 6 months after discharge (Mann–Whitney U-test).
Relationship Between Initiation of ARNI, MRA, and SGLT2i and LD De-escalation
The proportions of patients who initiated any of ARNI, MRA, and SGLT2i during hospitalization were significantly higher in the LD de-escalation group than in the no de-escalation group (Table 5). After adjusting for covariates, the initiation of any of these drugs during hospitalization remained independently and significantly associated with LD de-escalation after discharge (OR, 2.509; 95% confidence interval, 1.073-5.868). Furthermore, even after adjusting for covariates and beta-blocker use, the association remained independent and significant (2.485; 1.029-6.001). The proportion of patients with de-escalated LD dose after discharge tended to increase with the number of ARNI, MRA, and SGLT2i initiated during hospitalization (P = .013; Table 6).
Relationship Between Initiation of ARNI, MRA, and SGLT2i and LD De-escalation After Discharge.
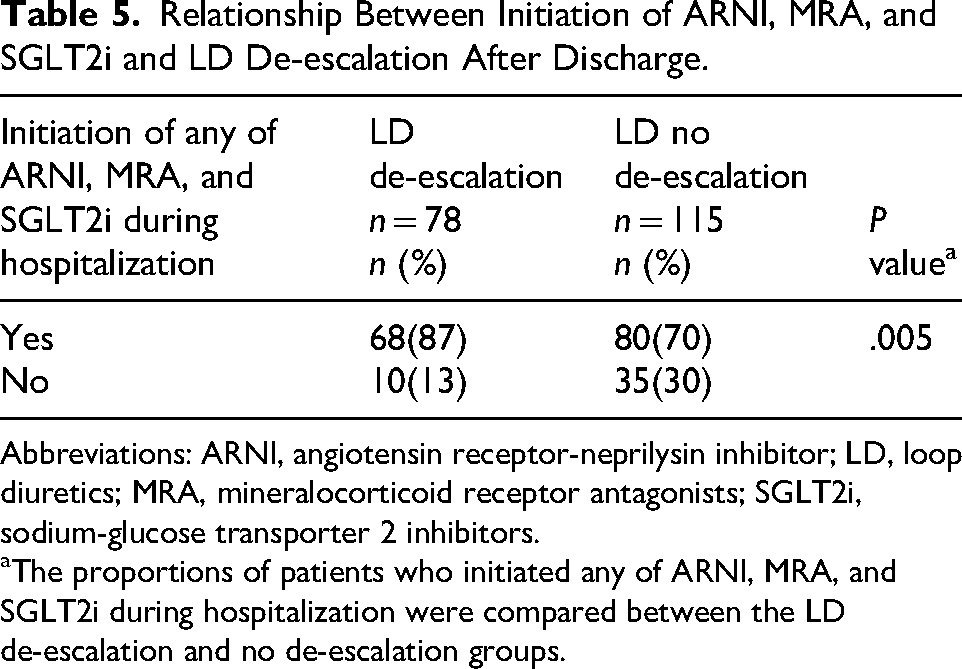
Abbreviations: ARNI, angiotensin receptor-neprilysin inhibitor; LD, loop diuretics; MRA, mineralocorticoid receptor antagonists; SGLT2i, sodium-glucose transporter 2 inhibitors.
The proportions of patients who initiated any of ARNI, MRA, and SGLT2i during hospitalization were compared between the LD de-escalation and no de-escalation groups.
Relationship Between the Number of ARNI, MRA, and SGLT2i Initiated and LD De-escalation After Discharge.

Data are shown as the number of patients (percentage).
Abbreviations: ARNI, angiotensin receptor-neprilysin inhibitor; LD, loop diuretics; MRA, mineralocorticoid receptor antagonists; SGLT2i, sodium-glucose transporter 2 inhibitors.
P values for linear trend relation between the number of ARNI, MRA, and SGLT2i initiated during hospitalization and LD de-escalation after discharge.
The relationship between changes in GDMT regimen after discharge and LD de-escalation is shown in Supplemental Table 2. Overall, 109 (56%) patients maintained the same GDMT regimen at 6 months after discharge. Changes in the GDMT regimen after discharge were not significantly different between the LD de-escalation and no de-escalation groups.
Subgroup Analysis Based on LVEF
The results of the univariate and multivariate analyses for each LVEF subgroup are shown in Supplemental Tables 3 and 4. Factors independently and significantly associated with LD de-escalation after discharge varied by LVEF subgroup: a high hematocrit level at discharge in the HFrEF group; ischemic etiology and BMI ≥ 22 kg/m2 in the HFmrEF group; and NYHA class II-III at admission in the HFpEF group (Supplemental Table 4). Additionally, the proportions of patients who initiated any of ARNI, MRA, and SGLT2i during hospitalization were significantly higher in the LD de-escalation group than in the no de-escalation group in the HFmrEF subgroup (Supplemental Table 5).
Discussion
This study showed that age <75 years, BMI ≥ 22.0 kg/m2, and absence of atrial fibrillation were associated with LD de-escalation after discharge. Additionally, the de-escalation tended to be more frequent with increasing the number of ARNI, MRA, and SGLT2i initiated during hospitalization. To our knowledge, this is the first study showing the factors associated with LD de-escalation and a relationship between initiation of ARNI, MRA, and SGLT2i during hospitalization and LD de-escalation in patients with ADHF. In patients with these factors, appropriate de-escalation in LD dose after discharge may prevent worsening of renal function or HF exacerbation. Additionally, proactive initiation of ARNI, MRA, and SGLT2i during hospitalization may lead to LD de-escalation, which may improve prognosis for patients with HF.
Notably, the 3- to 6-months period after discharge is a high-risk period for HF rehospitalization and death for patients with ADHF. 26 Various HF management strategies should be implemented early post-discharge to prevent events during this period.4,5,7,8 HF management in this early post-discharge period includes frequent follow-up to check for congestive symptoms, blood laboratory values, and hemodynamics, as well as adjusting the LD dose and starting and/or up-titrating the dose of the GDMT.4–8 This period is also a time of frequent evaluation of GDMT and LD. The number of patients on long-term LD use increases if the LD dose is not appropriately reduced or discontinued. Long-term LD use worsens the prognosis of HF owing to RAAS activation and worsening renal function. Therefore, LD de-escalation should be considered in the early post-discharge period.
Older age was associated with no change or an increase in LD dose. Older adults are prone to pulmonary edema caused by structural modifications during the aging process.27–30 Furthermore, they are more likely to develop peripheral edema due to decreased renal function, malnutrition, and decreased muscle activity.31–34 Hence, their LD dose may have been maintained or increased because they were more prone to systemic fluid retention.
Low BMI was associated with no change or an increase in LD dose. Patients with HF who have low BMI may be prone to repeated HF exacerbations, leading to a higher risk of all-cause mortality and cardiovascular death. 35 Additionally, it was reported in a study that patients with HF who have lower BMI have a lower rate of using ACEi or ARB, beta-blockers, and MRA at discharge than patients with higher BMI.35,36 In this study, patients with BMI < 22.0 kg/m2 were less likely to be initiated on ≥3 GDMT at discharge (BMI ≥ 22.0 kg/m2 vs <22.0 kg/m2; 84% vs 67% P = .009). A network meta-analysis demonstrated that a higher number of GDMT combinations was associated with a lower risk of cardiovascular events. 37 Therefore, patients who had lower BMI were not using GDMT, which may have increased HF exacerbation risk and possibly led to the maintenance or increase of their LD dose.
Atrial fibrillation was associated with no change or an increase in LD dose. Patients with HF and atrial fibrillation develop an increase in left atrial pressure and left ventricular filling pressure.38,39 Additionally, those with long-standing persistent atrial fibrillation had reduced capacity to produce atrial natriuretic peptide (ANP) owing to left atrial fibrosis. 40 Therefore, patients with comorbid atrial fibrillation may have had their LD dose maintained or increased because they could have elevated left atrial pressure or reduced ability to benefit from the action of ANP.
Some patients with HF have worsened congestion after reducing their LD dose. 41 Additionally, continuous LD use causes a decline in renal function. 9 Thus, we investigated the worsening of congestion, the occurrence of cardiovascular events, and the worsening of renal function after discharge in patients with ADHF. The results showed that, in the LD de-escalation group, BNP decreased, whereas BUN and eGFR remained unchanged. Additionally, the occurrence of cardiovascular events was lower in the LD de-escalation group than in the no de-escalation group. These results suggest that the LD de-escalation group had improved congestion after discharge, their renal function did not worsen, and they were a population with a low risk for cardiovascular events. Therefore, it is believed that those with the factors identified in this study can reduce their LD dose without experiencing worsening congestion after discharge.
This study revealed that LD de-escalation after discharge may occur more frequently when the number of ARNI, MRA, and SGLT2i initiated during hospitalization was increased. Diuretic effects of ARNI, MRA, and SGLT2i have different mechanisms, respectively.13,14 Therefore, the use of increasing combinations of these drugs would have enhanced the diuretic effect owing to their additive effect. Furthermore, the diuretic effect may have been enhanced by combining these drugs and LD. Moreover, these 3 drugs may have suppressed worsening congestion by improving cardiac remodeling and recovering cardiac function.42–44 Thus, increasing the number of ARNI, MRA, and SGLT2i initiated during hospitalization may reduce the LD dose required after discharge owing to their diuretic effects and improvement in cardiac remodeling.
Limitations
This study had some limitations. First, information on the disease duration of atrial fibrillation was not collected. The degrees of congestion in patients with HF who had atrial fibrillation differed depending on disease duration, which may have affected LD de-escalation. Second, because this was a retrospective observational study, the number of outpatient visits after discharge may have differed among patients; thus, the impact of LD de-escalation could not be examined. Third, because this was a single-center study, the external validity of the identified factors could not be evaluated. Fourth, as data on the dosage of GDMT were not collected, their influence on LD de-escalation could not be examined. Fifth, the differing results of the subgroup analysis based on LVEF categories may have been influenced by the small sample size. Sixth, since LVEF data were not collected before and after hospitalization, subgroup analysis to distinguish HF with improved ejection fraction from HFpEF or HFmrEF could not be performed.
Conclusion
Age <75 years, BMI ≥ 22.0 kg/m2, and absence of atrial fibrillation were factors associated with LD de-escalation after discharge in patients with ADHF. These factors are useful indicators for selecting patients with ADHF who can de-escalate their LD dose after discharge. Additionally, the de-escalation after discharge may occur more frequently if the number of ARNI, MRA, and SGLT2i initiated during hospitalization was increased. These findings may lead to appropriate LD de-escalation after discharge in patients with ADHF.
Supplemental Material
sj-docx-1-cpt-10.1177_10742484261431652 - Supplemental material for Factors Associated With Loop Diuretic De-escalation in Patients With Acute Decompensated Heart Failure: The Influence of Guideline Directed Medical Therapy Initiation
Supplemental material, sj-docx-1-cpt-10.1177_10742484261431652 for Factors Associated With Loop Diuretic De-escalation in Patients With Acute Decompensated Heart Failure: The Influence of Guideline Directed Medical Therapy Initiation by Satoshi Hanazawa, B.Pharm, Noriko Kohyama, PhD, Erika Iwasaki, PhD, Kenta Muraoka, PhD, Mayumi Inamoto, PhD, Mio Ebato,MD, PhD, Hiroshi Suzuki, MD, PhD, and Mari Kogo, PhD in Journal of Cardiovascular Pharmacology and Therapeutics
Footnotes
Acknowledgments
The authors are grateful to Ami Takashima for her efforts in collecting the data.
Ethical Considerations
This study was approved by the Ethics Committee on Showa Medical University (Approval No. 2023-215-A). This study was conducted in accordance with the principles of the Declaration of Helsinki.
Consent to Participate
Patients were informed that they could opt out of having their data used for research purposes on the Showa Medical University Fujigaoka Hospital's website.
Author Contributions
Conceptualization: SH, NK, EI, KM, MI, ME, HS, and MK; Data curation: SH and KM; Formal analysis: SH, NK, and EI; Methodology: SH, NK, EI, MI, ME, HS, and MK; Resources: SH and MK; Investigation: SH and KM; Visualization: SH and EI; Writing—original draft: SH, NK, EI, and MK; Writing—review & editing: SH, NK, EI, KM, MI, ME, HS, and MK; Project administration: NK and MK; Supervision: NK and MK. All authors read and approved the final version.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to patient confidentiality but are available from the corresponding author on reasonable request.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.