
Abstract
Dofetilide is a class III antiarrhythmic agent approved by the Food and Drug Administration for the conversion of atrial fibrillation and atrial flutter and maintenance of sinus rhythm in symptomatic patients with persistent arrhythmia. Drug trials showed neutral mortality in post–myocardial infarction patients and those with heart failure. This is a review of postmarket data, including real-world efficacy and safety in a variety of populations. Dofetilide has been used off-label with success in patients with paroxysmal atrial fibrillation and atrial flutter, as well as atrial tachycardia and ventricular tachycardia. The real-world acute conversion rate of atrial fibrillation and atrial flutter is higher than that reported in clinical trials. Dofetilide has an acceptable safety profile when initiated (or reloaded) under hospital monitoring and dosed according to creatinine clearance. Dofetilide is well tolerated and a good choice for patients with acceptable renal function and a normal QT interval, especially if atrioventricular nodal blockade needs to be avoided.
Introduction
Initial phase II studies of dofetilide occurred in the early 1990s. Dofetilide was approved by the Food and Drug Administration (FDA) in 1999 for conversion of atrial fibrillation (AF) and atrial flutter (AFl) and maintenance of sinus rhythm in symptomatic patients with AF and AFl of over 1-week duration. 1 Dofetilide is the only one of 4 oral potassium channel–blocking antiarrhythmic drugs available in the United States that is not a multichannel blocking agent. The 2014 AF guidelines for maintenance of sinus rhythm recommend dofetilide for first-line therapy in patients with or without structural heart disease. 2 Primarily due to an aging population, the incidence of AF continues to rise. Despite increased utilization and effectiveness of AF ablations, antiarrhythmic drug therapy is still widely used. Prerelease clinical studies indicated in-hospital initiation of dofetilide reduced the risk of life-threatening proarrhythmia. This article is a review of key studies in addition to postmarket data of efficacy and safety of this drug, as well as its off-label use by cardiologists. There may be renewed interest in dofetilide now that a generic, more affordable form is available and the fact that no new antiarrhythmic agent is near commercial approval.
Pharmacokinetics and Electrophysiologic Effects
Dofetilide is a class III antiarrhythmic agent that selectively blocks the IKr potassium ion channel, resulting in prolongation of the action potential. The drug also prolongs the effective refractory period, with a greater effect on the atria than the ventricles. These electrophysiologic effects are dose dependent. Dofetilide has no β-blocking or sodium channel–blocking properties, so it does not significantly decrease the heart rate, prolong the PR interval, or increase the QRS duration. The only drug effect seen on the surface electrocardiography (ECG) is QT prolongation. Dofetilide is hemodynamically well tolerated in patients with heart failure with no negative inotropic effect. 1,3
Dofetilide has an oral bioavailability of greater than 90%. Peak plasma concentration is reached 2 to 3 hours postdosing and is not affected by food. The half-life of the drug is 8 to 10 hours in the setting of a normal creatinine clearance (CrCl). Steady state is reached in 3 days. The majority (80%) of dofetilide is eliminated through the kidneys, with a small portion excreted in feces or metabolized by the CYP3A4 enzyme. Several drugs cannot be used in conjunction with dofetilide since they can significantly increase the plasma concentration of dofetilide. These drugs include verapamil, hydrochlorothiazide, and renal cation transport system inhibitors (Table 1). 1,3
Medications Contraindicated With Dofetilide.

Clinical Trials in AF
Based on the data from 3 main randomized, double-blind, placebo-controlled studies, the efficacy and safety of dofetilide was established. The European and Australian Multicenter Evaluative Research on Atrial fibrillation Dofetilide (EMERALD) trial was one of the efficacy trials. It included 671 patients with persistent AF (median duration: 3 months), randomized to dofetilide twice daily, sotalol 80 mg twice daily, or placebo. The doses of dofetilide used were 500, 250, or 125 μg twice daily, adjusted for QT prolongation and renal dysfunction. Patients were monitored in the hospital for 3 days, and those who did not convert to sinus rhythm with medical therapy by the third hospital day were electrically cardioverted. In this study, more patients were chemically converted to sinus rhythm within 72 hours of dofetilide initiation than those given placebo. This conversion occurred in a dose-dependent manner. Conversion rates were 6.1%, 9.8%, and 29.9% on 125, 250, and 500 μg dofetilide twice daily, respectively. Patients on placebo experienced a 1.2% spontaneous conversion rate. At 3, 6, and 12 months, high-dose dofetilide was significantly better in maintaining sinus rhythm than low-dose dofetilide and sotalol. High-dose dofetilide patients were more likely to remain in sinus rhythm at the end of 1 year (66%) compared to placebo group (21%) or the sotalol group (50%). The incidence of serious adverse effects was similar in all groups. 4
The Symptomatic Atrial Fibrillation Investigative Research on Dofetilide (SAFIRE-D) study was another major efficacy trial where 325 patients who had been in AF or AFl for 2 weeks to 6 months were hospitalized and randomized to either placebo or 125, 250, or 500 μg dofetilide adjusted to QTc monitoring and renal function. Pharmacological cardioversion rates for 250 and 500 μg dofetilide were 9.8% and 29.9%, respectively, significantly higher when compared to placebo (1.2%). About 70% of patients who converted to sinus rhythm did so within the first 24 hours. Based on this study, dofetilide 500 μg twice daily was found to be significantly effective in maintaining sinus rhythm, with 50% of patients remaining in sinus rhythm at 6 months and 47% at 1 year. Only 30% and 20% of patients on placebo were still in sinus rhythm at 6 months and 1 year, respectively. Lower doses of dofetilide were not found to be significantly effective in maintaining sinus rhythm. 5
The Danish Investigations of Arrhythmia and Mortality on Dofetilide (DIAMOND) studies consisted of 2 separate double-blind, placebo-controlled trials designed to evaluate the safety of dofetilide in 2 high-risk patient populations: congestive heart failure (DIAMOND-CHF) 6 or recent myocardial infarction (DIAMOND-MI). 7 These did not assess drug efficacy, and only 16% of these patients had persistent AF. All patients in these 2 studies were hospitalized and randomized to either dofetilide 500 μg twice daily or placebo. The protocol called for patients in AF/AFL to receive 250 μg twice-daily dofetilide.
In the DIAMOND-CHF study, patients with left ventricular systolic dysfunction (ejection fraction <35%) were included; 762 patients were randomly assigned to receive dofetilide and 756 to receive placebo in double-blind study. All-cause mortality occurred in 41% of dofetilide-treated patients compared with 42% of patients in placebo group (P = .56). In patients with congestive heart failure and reduced left ventricular function, dofetilide was effective in converting AF to sinus rhythm, preventing AF recurrence and reducing the risk of hospitalization for worsening heart failure. However, the drug had no effect on mortality. 6
In the DIAMOND-MI study, 1510 patients with severe left ventricular dysfunction (ejection fraction <35) and recent myocardial infarction (MI) were enrolled in a randomized, double-blind study comparing dofetilide with placebo. In patients with severe left ventricular dysfunction and recent MI, dofetilide treatment did not affect all-cause mortality, cardiac mortality, or total arrhythmic deaths. 7
Role of Dofetilide in Acute Cardioversion of Atrial Arrhythmias
The use of intravenous dofetilide in the acute conversion of AF and AFl has been looked at by several groups. 8 -10 In a study by Falk et al, 8 91 patients with either sustained AF or AFl were randomized to either placebo or administration of lower dose (4 μg/kg) or higher dose (8 μg/kg) of dofetilide. Pharmacological cardioversion to sinus rhythm was observed in 0%, 12.5%, and 31%, respectively, in these groups. These data are similar to the conversion rates in the SAFIRE-D study using oral dofetilide. Conversion was more frequently noted in the smaller subset of patients with AFl as compared to those with AF. Norgaard and colleagues saw considerably higher conversion rates of 64% to sinus rhythm with the use of the higher dose of 8 μg/kg. 9 Acute conversion of AF/AFl with intravenous dofetilide in the acute postoperative period following coronary artery bypass surgery also carries conversion rates of 44% and 36% using the higher dose or lower dose, respectively. 10 Although better than placebo (24%), these differences did not reach statistical significance in this particular study. These data were all from premarketing studies using intravenous dofetilide, which are not available in the United States.
Real-world data on oral dofetilide’s effectiveness in pharmacological conversion of AF/AFL are limited. However, there is evidence that the conversion rate is actually higher than what was reported in the clinical trials. 5 A retrospective study of 80 patients at our institution revealed chemical conversion in 61%. In this group, 51 patients had persistent AF/AFL, and 29 were paroxysmal. 11 Cotiga et al reviewed 80 patients with persistent AF who received dofetilide at a New York City hospital and found a 77% chemical conversion rate. The pharmacological conversion success rate increased with higher doses: 20% on 125 μg, 44% on 250 μg, and 85% on 500 μg. Additionally, a larger left atrium and longer time in AF predicted pharmacological cardioversion failure in their population, with an average duration of only 19 days in AF. 12 Prystowsky et al reported a 63% medical conversion rate of 69 patients, the majority of which were in persistent AF with a mean duration of 68 days. 13 Another retrospective cohort of over 200 patients with persistent AF/AFL had a 45% acute pharmacological conversion rate during dofetilide loading. In this group, chemical conversion was predicted by female gender, AFL, prior catheter ablation, and shorter time in AF/AFL. 14
Acute conversion to sinus rhythm, however, does not necessarily predict long-term arrhythmia-free survival. In the real-world populations discussed above, where long-term follow-up data of 6 to 21 months were known, only approximately one-third of patients were arrhythmia-free at the end of the follow-up period. 11,13,14
Use of Dofetilide in Special Populations
Role in Ventricular Arrhythmias
Although dofetilide has only been approved for the treatment of AF in the United States, there are reports of its use in suppression of ventricular arrhythmias. A retrospective study by Baquero et al showed promising results in a small population of 30 consecutive patients with recurrent, antiarrhythmic drug refractory ventricular arrhythmias and implantable cardiac defibrillators. 15 During the initial month of therapy, dofetilide decreased the number of ventricular arrhythmia (ventricular tachycardia/ventricular fibrillation [VT/VF]) events from an average of 2.3 episodes to 0.4. Additionally, the number of defibrillator therapies was also significantly reduced. This effect was maintained over the 32-month follow-up period. It is important to note that although ventricular arrhythmias and device therapies were reduced over the early follow-up period, arrhythmia control did seem to decrease over time and the drug was eventually discontinued in 7 patients due to failure to suppress VT/VF. This may, however, more likely represent worsening of the underlying substrate rather than reduction in drug effect.
Role in Congestive Patients With Heart Failure
Maintenance of sinus rhythm can be especially critical in those with congestive heart failure or underlying ventricular dysfunction. Atrial fibrillation is common in this population of patients and, in addition to symptoms, leads to increased cardiovascular morbidity. In the DIAMOND-CHF study, 6 dofetilide was shown to be effective in restoration of sinus rhythm and at preventing further arrhythmia recurrence: at 1 year, 79% maintained sinus rhythm versus 42% in the placebo group. It was also seen to result in reduction of risk of hospitalization for worsening heart failure, likely due to better control of atrial arrhythmias. This study did not find that long-term use was associated with increased mortality, and based on these results, it does seem that the use of dofetilide is relatively safe in patients with heart failure and this is similarly reflected in the American Heart Association/American College of Cardiology/Heart Rhythm Society guidelines.
Role in Congenital Heart Disease
Atrial tachyarrhythmias (ATs) are a frequent clinical challenge within the congenital heart disease (CHD) population and can represent a major source of both morbidity and mortality. Single-center studies as well as 1 multicenter retrospective study
16,17
evaluated the role of dofetilide in this particular group of patients. One such single-center study followed 13 adults with CHD and symptomatic recurrent AT. These patients included tetralogy of Fallot (n = 4), 1 with pulmonary atresia and right-sided aortic arch, atrial septal defect (n = 2), and transposition of the great arteries (TGAs; n = 3); 1 dextro-transposition (
Although other antiarrhythmic drugs have been shown to have efficacy in this population, in those with heart failure or impaired systolic function, especially when amiodarone use represents a significant adverse side effect profile with the young age of the patient, dofetilide may offer an additional pharmacological option. One issue that may arise in this group of patients is the higher prevalence of intraventricular conduction delay with a prolonged QT interval even prior to initiation of therapy. However, routine monitoring of the corrected QT interval as a change from baseline or use of the corrected JT interval may help monitor for repolarization changes during the period of drug loading.
An older multicenter study drew from the experience of 4 centers in the United States and Canada. In this retrospective analysis, a total of 20 patients with CHD who were admitted for recurrent AT were identified and reviewed. The median age of initiation of therapy was 30 years, and all but one had had prior cardiac surgery. Arrhythmias on presentation included AF (n = 4), AFl (n = 3), and intra-atrial reentrant tachycardia (n = 13). Seventy percent had undergone prior catheter ablation which had either been unsuccessful or initially successful, with subsequent recurrence. During hospitalization, adverse events were uncommon: 2 patients did have torsades de pointes (TdP) and another had excessive prolongation of QT interval requiring discontinuation of medication. Acute conversion to and maintenance of sinus rhythm with no adverse events during hospital stay were observed in 85% of patients. At a median of 1-year follow-up, 55% of these patients remained on dofetilide. 17 These are encouraging data, when compared to a substudy of DIAMOND, showing that 45% of patients without CHD were maintained in sinus rhythm on dofetilide after 1 year of follow-up. 18
Role in Hypertrophic Cardiomyopathy
Recently, a small retrospective study of 25 patients with hypertrophic cardiomyopathy and AF was reported. Persistent AF was present in 75% of the patients. Three patients had their dofetilide discontinued during hospital dose titration due to prolongation of the QT interval; however, no TdP was reported. Of the 21 patients discharged on dofetilide, 11 remained on treatment for a median follow-up of 396 days. Further studies are needed to assess the safety and efficacy of dofetilide in this patient population since currently the guidelines do not recommend dofetilide as an alternative drug in this patient population. 19
Role in Catheter Ablation Patients
Dofetilide also seems to have a role in patients considered candidates for catheter ablation. A single-center Canadian study retrospectively collected data on the use of dofetilide in patients undergoing catheter ablation. In this cohort of almost 130 patients, the drug was started in preparation for ablation, immediately following ablation to prevent recurrences within the early postablation period, or after the 3-month blanking period to treat recurrent AF. On average, most patients had failed 2 prior antiarrhythmic drugs. The majority of these patients had paroxysmal AF (58%) versus persistent AF (27%). Thirty-one percent had underlying structural heart disease. After an average follow-up of 15 months, only 2 adverse drug events were noted requiring discontinuation: an allergic reaction to the drug and symptomatic ventricular bigeminy presumed to be related to dofetilide. In general, the drug was well tolerated and was effective in over half of these patients who had previously failed or were intolerant of flecainide, propafenone, or sotalol, or in whom amiodarone was either discontinued due to intolerances or side effects, or in preparation of ablation. 20
Predictors of Dofetilide Efficacy
The efficacy of dofetilide for acute cardioversion and maintenance of sinus rhythm is most consistently dose related, with a significantly improved response to the 500 μg dose. 4,5,12 The only clinical trials presented to the FDA showing dofetilide efficacy were of patients with persistent AF, resulting in the approval of dofetilide for AF/AFl of over 1-week duration. 1 The premarketing studies of patients with paroxysmal AF on dofetilide did not show significant efficacy and were never published. 1,3 Many of the postmarketing studies have included only persistent AF, or a minority of patients with paroxysmal AF, resulting in limited data for the paroxysmal AF group. However, in a cohort of 287 patients with AF, of which 71% were paroxysmal, no difference in dofetilide efficacy was found between the persistent and paroxysmal AF groups. In this study, the only variable found to predict dofetilide efficacy was coronary artery disease. The success rate of dofetilide therapy in patients with coronary artery disease was 41.1%, compared to the 23.5% in those without coronary artery disease. 21
Comparative Effectiveness With Other Antiarrhythmic Drugs
Studies have compared dofetilide directly to other antiarrhythmic agents, mostly in a retrospective manner. In reviewing 1 single-center study which compared dofetilide with dronedarone, amiodarone, sotalol, and class IC antiarrhythmic agents, although not as effective as amiodarone at preventing recurrences of AF, dofetilide was as effective as dronedarone. In addition, it significantly reduced hospital admissions associated with arrhythmia. This was a large group of over 5000 patients, followed for an average of 2 years, the majority of whom had paroxysmal AF. Limitations of the study may have included an inability to take into account underlying differences in the patient populations within the different antiarrhythmic groups, although the authors did attempt to adjust for major baseline characteristics in a multivariate analysis. 22
Another paper did, however, show dofetilide to be superior to dronedarone, with a lower rate of arrhythmia recurrence, with only 45% experiencing recurrence of AF as compared to 71% on dronedarone over the first year of treatment. This was a higher morbidity group, with 43% having had a history of congestive heart failure. About half of these patients had paroxysmal AF. 23
Combination of Dofetilide With Other Antiarrhythmic Drugs
In general, there are little data regarding combination of dofetilide with other antiarrhythmic drugs. In a study by Liu et al, it was demonstrated that in rabbits, combined use of dofetilide and mexiletine synergistically increases the atrial effective refractory period and effectively suppresses the inducibility of AF and also markedly reduces QT prolongation and TdP risk posed by dofetilide. There are no studies in humans to date. 24
Safety
Dofetilide is a well-tolerated drug without significant noncardiac adverse side effects. However, in-hospital initiation of the drug is mandated for the risk of TdP. Additionally, the dofetilide dose for each patient is determined by their CrCl using the Cockcroft and Gault formula. These recommendations from the FDA were a result of findings from clinical trials. Before 1994, a significant incidence of TdP cases occurred in dofetilide trials. Patients were assigned dosages without regard to CrCl, and even 750 μg doses were used. In 1994, the protocol was changed midway through the studies. Once the 750 μg dose was discontinued and the drug dose was adjusted for CrCl, the result was a significantly lower incidence of TdP. 1,3 In the DIAMOND-CHF trial, the incidence of TdP was 2.9% after the protocol change, compared to 4.8% prior to the changes made. 3
The DIAMOND trials were studies of patients with structural heart disease and heart failure, which showed dofetilide had a neutral effect on mortality. Study protocol called for patients to be monitored on telemetry in the hospital for 3 days to initiate dofetilide. Patients with a QTc greater than 460 milliseconds or with a history of polymorphic VT were excluded from the study. In the DIAMOND-CHF trial, 3.3% of patients had TdP, but the majority of cases occurred in the first 3 days of initiation of the drug. Only 0.9% of patients in the DIAMOND-MI study experienced TdP, and approximately half of the episodes occurred outside the in-hospital monitoring window. In both these studies, the dofetilide dose was decreased for a QT >550 milliseconds or >20% increase in QT over baseline. This occurred in 5% of DIAMOND-CHF patients and 7% of DIAMOND-MI patients on dofetilide. The drug was discontinued due to prolonged QT or QTc in 1.8% and 2.5% of DIAMOND-CHF and DIAMOND-MI patients, respectively. Risk factors for TdP in the clinical trials were a dose of 500 μg, a history of sustained VT, a baseline QT >450 milliseconds, a significant QT prolongation during drug loading, or female gender. Although the incidence of TdP was greater in the dofetilide-treated group when compared to placebo, dofetilide did not increase mortality in this population at high risk for sudden cardiac death, when monitored the first 3 days and dosed according to CrCl. 6,7
The efficacy trials of EMERALD and SAFIRE-D were not powered for safety, and data regarding adverse events are not complete. In the EMERALD trial, there was 1% incidence of TdP and 1 death in the dofetilide group. Similarly, 1.2% of patients in the SAFIRE-D trial developed TdP. In both trials, there was no significant difference in all-cause mortality between the dofetilide and placebo groups. 25
To provide some postmarket safety data on patients with AF treated with dofetilide, the electrophysiologists at Cleveland Clinic looked at over 1000 patients with dofetilide initiated between 2008 and 2012 at their institution. During in-hospital loading, 1.2% of patients experienced TdP. Dofetilide was stopped in 7.5% of patients during loading due to QTc prolongation or TdP. The Cleveland group also found the 1-year all-cause mortality of patients still taking dofetilide after 1 year to be over 2 times higher than for patients whose drug had been discontinued (hazard ratio: 2.48). However, patients who were no longer taking dofetilide due to an incident of TdP still had a higher mortality in the first year than the other patients off dofetilide without having had TdP (17.6% vs 3%). The Cleveland group speculated that TdP with dofetilide could predict high risk of proarrhythmia with other QT-prolonging drugs. For patients surviving the first year of dofetilide therapy, their mortality risk was lower than patients no longer taking the drug. These data suggest close monitoring is warranted in the first year of dofetilide use. Additionally, the Cleveland group found the risk factors for TdP to be female gender, a lower ejection fraction, greater QTc prolongation, and the 500 μg dose of dofetilide. These findings were similar to those in the dofetilide efficacy trials. Left ventricular hypertrophy was not found to be a risk factor for TdP in the Cleveland group, suggesting dofetilide could be used safely in this population. 25 Prior to the most recent AF guidelines, dofetilide was not recommended for use in patients with significant left ventricular hypertrophy.
Another retrospective study was completed consisting of 114 patients with AF starting dofetilide at the Minneapolis VA between 2011 and 2014. Their results showed 17% of patients had dofetilide stopped during loading due to QT prolongation and 2% due to VT. In this population, 28% of patients starting dofetilide were also taking other QT-prolonging drugs. Of the patients having to stop dofetilide during loading, 45% were taking other QT-prolonging drugs. This is a higher incidence of QT prolongation and TdP during drug loading than was reported in the clinical trials, where concomitant use of QT prolonging drugs was not allowed. 26
Safety in Women
It is known that women have a longer baseline QTc interval than men. Also, female sex is a risk factor for proarrhythmia with potassium channel–blocking agent. Dofetilide and sotalol carry a higher risk of TdP than does amiodarone and dronedarone. However, even with the lower risk drugs, the reports of TdP occur at least twice as often in women as in men. In the DIAMOND trials, the odds ratio for women on dofetilide developing TdP was 3.2. 27
Recently, a retrospective study from Duke University compared 220 matched men and women (CrCl >60 mL/min) in which the 500 μg dose of dofetilide twice daily was initiated. In this cohort, there was no significant gender difference in the baseline median QTc interval. Dofetilide had to be discontinued or the dose decreased in 55% of women compared to 32% of men (P < .001). Unacceptable QTc prolongation was responsible for the majority of the dose reductions or drug discontinuations. There were no cases of TdP in either men or women. The rates of drug discontinuation and dose reductions were much higher in this study than in the DIAMOND trials. However, this population only included patients started on 500 μg, with a CrCl >60 mL/min. Additionally, women comprised only 28% of the population of the DIAMOND trials. 28
Even though the risk of QT prolongation and TdP is higher in women, the algorithm for dosing dofetilide is the same regardless of sex. Extra vigilance in monitoring women on dofetilide can go a long way to prevent proarrhythmia. Uncontrolled heart failure, hypokalemia, and polypharmacy with drugs that can prolong the QT interval are all known risk factors for TdP that should be avoided in female patients on dofetilide. 27
Dofetilide Reloading
The FDA recommends reinitiation of dofetilide during in-hospital monitoring for 3 days. The data behind this decision are in the drug’s package insert. The mean change in the QTc from baseline during initial dofetilide loading is higher than 3 weeks later with the drug at steady state concentration. 1 For a long while, there were no data on the proarrhythmia risk of reinitiation of the drug. A study published in 2016 assessed practice variation among cardiologists in the reinitiation of dofetilide. A questionnaire was sent worldwide, but the majority of responders practiced in North America. Wide variation in practice was seen with 21% of cardiologists always admitting patients for reinitiation of dofetilide, while 37% of physicians admitted pateints in <10% of cases. 29
In 2017, a retrospective study from Cleveland Clinic analyzed 138 patients admitted for reinitiation of dofetilide from 2008 to 2012. No TdP occurred in patients reloaded at their previous dofetilide dose, but 6.7% of patients reloaded at a higher than previous dose did experience TdP. In both groups, a significant number of patients required a dosage decrease for increased QTc. There was not a baseline QTc or JTc below which no TdP or significant QTc prolongation occurred. Their findings reinforce the need to monitor patients’ in-hospital for reinitiation of dofetilide. The Cleveland Clinic group recommends patients missing >2 doses should be readmitted. However, the package insert does not state how many missed doses necessitate monitored reloading. Dofetilide is usually held 3 days prior to AF ablations, so based on the Cleveland data, these patients should be reloaded in the hospital postablation. The risk of TdP without hospital reinitiation raises the concern for safety in the noncompliant patient who takes the drug erratically. Other patients may run out of the drug due to cost or insurance issues. 30
Dosing
The package insert has a black box warning stating dofetilide must be initiated or reinitiated in the hospital with the patient on continuous ECG monitoring for 3 days. Several criteria need to be verified prior to the decision to admit and start the drug (Table 2). Dofetilide is now available in generic form which makes it more affordable. However, prior to admission, the patients need to know whether the drug will be affordable to them. Any QT prolonging drugs or drugs contraindicated with dofetilide need to be discontinued (Table 1). Also, the creatinine level should be checked since the dofetilide dose is determined according to CrCl. Additionally, the potassium level needs to be within normal limits to help reduce the risk of TdP. A 12-lead ECG should be performed to measure the QTc prior to drug initiation. The QTc must not be >440 milliseconds, or >500 milliseconds with a bundle branch block. The uncorrected QT interval should be used if the heart rate is <60 beats/min. If these variables are acceptable, the admission can then be arranged. If the CrCl is >60 mL/min, 500 μg of dofetilide can be given twice daily. If the CrCl is 40 to 60 mL/min, a dose of 250 μg twice daily is initiated. For a CrCl 20 to <40 mL/min, 125 mL/min twice daily is the starting dose. Dofetilide is contraindicated in patients with CrCl <20 mL/min. An ECG will be repeated 2 to 3 hours after each dofetilide dose to measure the QTc at peak drug effect. If after the first dose, the QTc has increased >15% over the baseline, or if the QTc is >500 milliseconds (>550 milliseconds with bundle branch block), the dose of dofetilide should be decreased by half (Table 3). If the QTc becomes prolonged after the second or subsequent doses, dofetilide should be discontinued. In-hospital ECG monitoring is maintained for 3 days, or longer if needed, to monitor at least 12 hours after conversion to sinus rhythm. 1
Criteria to Verify Prior to Dofetilide Admission.
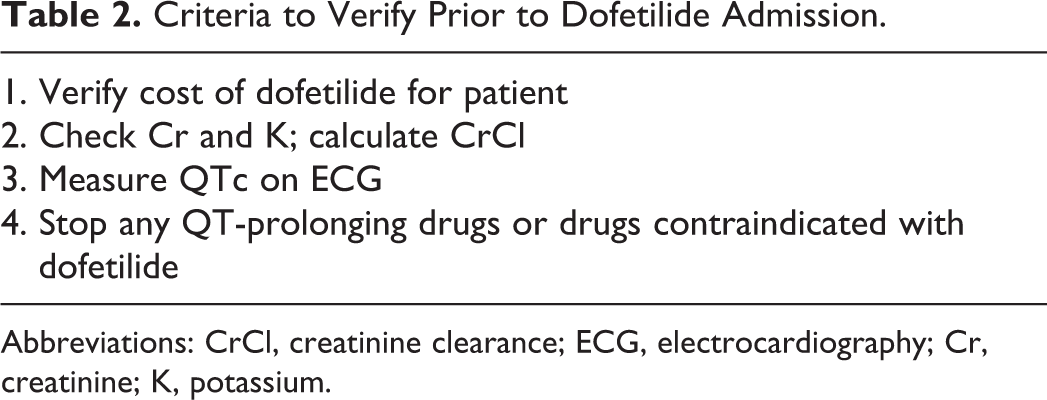
Abbreviations: CrCl, creatinine clearance; ECG, electrocardiography; Cr, creatinine; K, potassium.
Dofetilide Dosing Regimen.

Comparison With Amiodarone
Amiodarone therapy is frequently initiated in patients with structural heart disease without considering other possible antiarrhythmic options. Dofetilide compares favorably with amiodarone and may be a better option for some patients (Table 4). It has greater efficacy for acute termination of AF than does amiodarone. Although in-hospital initiation of dofetilide is required, many patients do not need electrical cardioversion. Due to in-hospital monitoring and dosing, according to CrCl, the risk of TdP is low. Dofetilide’s safety in patients with CHF and post-MI patients is similar to that of amiodarone. Unlike amiodarone, dofetilide has little sinus, atrioventricular nodal, and His-Purkinje system effects. They both have multiple drug interactions, but this is more of a problem with amiodarone. Dofetilide is renally cleared, whereas amiodarone is metabolized via the liver. The half-life of dofetilide is 10 hours, as opposed to 58 days for amiodarone. This results in a delay when switching from amiodarone to sotalol or dofetilide, due to the risk of QT prolongation and TdP. Dofetilide has no end-organ toxicity, which makes its use more appealing over amiodarone, especially in the younger patient.
Comparison of Dofetilide Versus Amiodarone.a

Abbreviations: AF, atrial fibrillation; AVN, atrioventricular nodal; CHF, congestive heart failure; HPS, His Purkinje System; MI, myocardial infarction; SR, sinus rhythm; TdP, torsades de pointes.
a± indicates minimal or none, + low, ++ moderate, and +++ high.
Conclusion
Dofetilide was approved for the treatment of persistent AF/AFl in symptomatic patients and has a higher chemical conversion rate than most other antiarrhythmic drugs. Its efficacy in maintaining sinus rhythm has been found to be comparable to the other oral potassium channel–blocking agents, with the exception of amiodarone. Dofetilide is also used off-label for paroxysmal AF/AFl, atrial tachycardia, and ventricular arrhythmias with encouraging results. It has a neutral mortality effect in populations with structural heart disease.
Dofetilide is a good choice for patients with acceptable renal function and normal QTc. As the only potassium blocking agent that does not affect heart rate, it is the best choice for patients with baseline bradycardia. Dofetilide is affordable to more patients now that the generic form is available. It is well tolerated without noncardiac adverse side effects. However, patients must be admitted for 3 days to initiate or reinitiate the drug due to the risk of TdP. Routine outpatient monitoring is required to follow renal function, potassium level, and QTc and avoid drug interactions.
Footnotes
Author Contributions
Deborah L. Wolbrette and Gerald V. Naccarelli contributed to conception and design, contributed to acquisition, analysis, and interpretation, drafted the manuscript, and critically revised manuscript. Sarah Hussain and Ilir Maraj contributed to conception and design, contributed to acquisition, analysis, and interpretation, and drafted the manuscript. All authors gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Naccarelli is a consultant to Janssen, Glaxo Smith Kline, Sanofi, Novartis, Aceion, and Omeicos.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Naccarelli has a research grant from Janssen.