
Abstract
Background
Hypertension remains a leading modifiable risk factor for cardiovascular disease, and effective anti-hypertensive prescribing is essential for optimal management. This study will evaluate the patterns of anti-hypertensive prescriptions, characteristics of specific drug class users, and significant factors influencing prescription choices within a Saudi Arabian cohort.
Methods
This retrospective, cross-sectional study at Al-Qatif Central Hospital included patients aged ≥40 years who attended outpatient cardiology and internal medicine clinics between January 2020 and December 2021. The characteristics of anti-hypertensive medication users and nonusers were compared using descriptive statistics. Logistic regression models were performed to identify factors associated with anti-hypertensive prescribing patterns adjusted for significant covariates, with results presented as adjusted odds ratios (OR) and corresponding 95% confidence interval (95% CI).
Results
About 62% of 5,852 patients were prescribed anti-hypertensive medication, with beta blockers (BBs) and calcium channel blockers (CCBs) being the most prescribed. BBs were primarily prescribed as monotherapy, constituting for 24% of prescriptions. Older patients (≥65 years) were more likely to receive combination therapy, with 17% receiving four anti-hypertensives medications. Diabetes mellitus was positively associated with the prescription of angiotensin receptor blockers (OR = 1.2, P < 0.05) and negatively associated with BBs prescribing (OR = 0.6, P < 0.05). Constipation exhibited a significant association with CCBs prescribing (OR = 1.4, P < 0.05).
Conclusion
This study demonstrates significant deviations from existing clinical guidelines, notably the overprescription of BBs in the management of hypertension. The findings highlight where doctors need to look more closely at their prescribing habits and suggest to promote the alignment of prescribing practices with emerging evidence-based recommendations.
Keywords
Introduction
Hypertension is a major public health concern, contributing substantially to global morbidity and mortality. As a primary modifiable risk factors for cardiovascular diseases (CVD), its effective management is essential for reducing the incidence of ischemic heart diseases, stroke, and other associated complications. 1 The silent and asymptomatic characteristics of hypertension complicate early diagnosis and optimal management, often leading to inadequate treatment adherence and suboptimal blood pressure control in many patients. 2
Anti-hypertensive medications have evolved over time, with several drug classes, including beta blockers (BBs), angiotensin-converting enzyme inhibitors (ACEIs), angiotensin receptor blockers (ARBs), calcium channel blockers (CCBs), and diuretics, forming the cornerstone of treatment. 3 Prescribing patterns vary significantly across regions and healthcare systems, influenced by factors including patient demographics, comorbidities, prescriber preferences, and adherence to clinical guidelines. While international guidelines recommend ACEIs, ARBs, CCBs, and thiazide diuretics as first-line treatment for uncomplicated hypertension, some regions continue to rely heavily on BBs, despite evidence indicating their limitations in certain populations.4–6
Understanding prescribing trends offers valuable insights into the possible overuse or underuse of certain drug classes. By examining factors such as age, gender, and comorbidities, one can distinguish patient subgroups that may benefit from targeted interventions designed to enhance treatment regimens. Previous research indicates that older adults frequently encounter challenges associated with polypharmacy and adverse drug reactions (ADRs), complicating anti-hypertensive therapy.7–10 Additionally, gender-specific differences in drug efficacy and ADRs have received increasing attention, with research indicating divergent prescription patterns for male and female patients. Male patients are more often prescribed ACEIs and BBs, whereas female patients tend to receive diuretics and ARBs.11,12 These patterns may be attributed to biological and clinical differences between genders that influence drug selection and response.
In Saudi Arabia, the prevalence of hypertension has been reported to range from 15.2% to 32.6%, with community-based studies indicating even broader ranges. 13 Despite considerable advancements in the healthcare system, only 59% of hypertensive patients receive anti-hypertensive treatment, reflecting the global challenge of achieving high treatment rates and effective blood pressure control.14,15 This study seeks to address the gap in regional data regarding anti-hypertensive prescribing practices in Saudi Arabia. The primary objectives are to assess the prevalence and prescribing patterns of anti-hypertensive medications, characterize users of specific anti-hypertensive classes and identify patient characteristics associated with the selection of anti-hypertensive treatments among patients visiting a cardiology and internal medicine outpatient clinic at a general hospital in the Eastern Region of Saudi Arabia. The findings from the current study may enhance clinical practice, particularly in optimizing treatment regimen for high-risk populations such as older adults and those with multiple comorbidities.
Methodology
Study Design and Study Population
This retrospective, cross-sectional descriptive study was conducted at Al-Qatif Central Hospital (QCH), Eastern Region, Saudi Arabia, from January 2020 to December 2021. The study included patients aged 40 years and older who visited outpatient cardiology and internal medicine clinics. Individuals under 40 years of age and those attending other medical care, such as endocrinology, hematology, nephrology, or in the emergency department, or admitted into hospital inpatient wards were excluded.
An age of 40 years was chosen to assess the impact of aging on the epidemiology of multiple morbidities and to examine how changes in comorbidities and coprescribed medications may influence the prescription of anti-hypertensive drugs. 16 For patients with multiple visits during the study period, only data from their first reported visit were included in the analysis.
Ethical Approval, Data Collection, Measures and Definitions
This study was a retrospective observational analysis of secondary data. Data collection was conducted with approval from the Institutional Review Board (IRB) at Mohammed Al-Mana College for Medical Sciences (SR/RP/79, 17/02/2022) and the IRB at QCH (QCH-SREC019/2022, 08/06/2022). Patient demographic information, comorbidities, and recent laboratory findings were retrieved from electronic medical records, while the prescribed medications were verified from the pharmacy electronic records.
Patient comorbidities were identified based on documentation in the medical records and through application of the Rx-risk comorbidities index to the list of prescribed medication. 17 Comorbidities were coded as per the International Classification of Disease, 10th revision 2016 (ICD-10). 18 The Charlson Comorbidities Index (CCI) was calculated to estimate the one-year mortality risk. 19 Creatinine clearance (CrCl) was calculated using the Cockcroft-Gault Equation. 20 The Cockcroft-Gault equation was used instead of other equations, such as CKD-EPI and MDRD, due to its relevance in pharmacokinetics, as drug clearance is closely linked to muscle mass and body weight, which directly impact dosage adjustments and therapeutic outcomes. To address limitations in distinguishing specific morbidities, certain conditions were consolidated: asthma and chronic obstructive pulmonary disease (COPD) were grouped under one variable “respiratory diseases,” osteoarthritis and rheumatoid arthritis under “arthritis-related diseases,” and different types of musculoskeletal pain including pain in the lower and upper back, muscles, bones, joints, ligaments, and tendons under “musculoskeletal pain.” Additionally, peptic ulcer, gastroesophageal reflux disease (GERD), and other gastritis-related conditions were consolidated under “gastritis-related diseases” because of overlapping clinical symptoms and treatment. Lastly, atrial fibrillation, venous thromboembolism, recent myocardial infarction, and mechanical valve replacement were combined as coagulation disorders.
The medication data, including long-term regular prescriptions, short-term, as-needed medication, and supplements were collected and coded as per the Anatomical Therapeutic Chemical (ATC) classification system. 21 Anti-hypertensive drugs were identified as CCBs (ATC code C08C), BBs (C07A), ACEIs (C09A), ARBs (C09C), and diuretics (thiazide_C03A and indapamide_C03BA11). Other anti-hypertensive drugs included methyldopa (C02AB), clonidine (C02AC01), hydralazine (C02DB02), and prazosin (C02CA01), as these four medications were the only drugs reported among the cohort. These medications were grouped into a single category since their low individual prescription frequency limited the statistical power to investigate each subclass independently. The classification aimed to maintain model stability while recognizing their common function as second-line or adjunct anti-hypertensive medications. The study documented anti-hypertensive prescriptions recorded at the initial outpatient visit during the study period. Therefore, the dataset lacks information on the duration of prior anti-hypertensive therapy and if treatment was newly initiated.
For this study, patients were initially classified by age into two groups: middle-aged (<65 years) and older (≥65 years) patients. They were further categorized by gender to assess the differences in prescription pattern between these groups.
Statistical Analysis
Demographic variables, comorbidities, and medications were summarized as follows: mean ± standard deviation (SD) for parametric continuous variables, median with interquartile range (IQR) for nonparametric continuous variables, and number with frequency (%) for categorical variables. To compare continuous variables, the Student's T-test and the Mann Whitney-U-test were used for parametric and nonparametric data, respectively. The Chi-square test was used to compare the frequency of categorical variables between groups.
Binary logistic regression was performed to calculate unadjusted and adjusted odds ratios (OR) with a 95% confidence interval (95% CI), examining the association between patient characteristics and the prescription of anti-hypertensive drugs cross the entire cohort. Multinominal logistic regression was employed to identify factors associated with the prescription of mono-, dual-, triple-, or quadruple anti-hypertensive therapy. The logistic regression models were adjusted for age, sex, CCI, CrCl, and the number of prescribed medications (NPM). Covariates were included in the models if they were statistically significant (P < 0.05) in univariate analysis or being reported as clinically significant in the literature. 22 Multicollinearity was assessed using the variance inflation factor. All statistical analysis was performed using SPSS version 23 and P ≤ 0.05 was considered statistically significant.
Results
This study included 5853 patients with 62% receiving anti-hypertensive prescriptions. The median age of the cohort was 59 years (IQR: 44-80), the mean CrCl was 93 ml/min (SD: 42), the average CCI score was 4 (SD: 2), and patients were prescribed an average of 7 medications (SD: 6). Fifty percent of the cohort were male (Table 1). Anti-hypertensive drug users were older (63 vs 54, P < 0.001), had a lower CrCl (92 vs 95, P < 0.001), a higher CCI score (5 vs 2, P < 0.001), and were more likely to be male individuals (52% vs 46%, P < 0.001) compared to nonusers (Table 1). The univariate analysis revealed that anti-hypertensive drug users had a higher prevalence of diabetes mellitus (45% vs 16%, P < 0.001), gastritis-related disease (49% vs 36%, P < 0.001), constipation (13% vs 10%, P < 0.001), coagulation disorder (66% vs 20%, P < 0.001), hyperlipidemia (69% vs 21%, P < 0.001), renal disease (4% vs 2%, P < 0.001), and respiratory disorder (12% vs 7%, P < 0.001). Conversely, anti-hypertensive drug users were less likely to have anemia (31% vs 38%, P < 0.001), arthritis-related disease (68% vs 70%, p < 0.001), or osteoporosis (37% vs 43%, P < 0.001) compared to nonusers (Table 1).
Characteristics of the Entire Cohort Classified Based on Anti-Hypertensive Drug Prescription.

CrCl, creatinine clearance; CCI, Charlson comorbidity index; NPM, number of prescribed medications; M, male.
The analysis of anti-hypertensive class prescriptions revealed that BBs were the most frequently prescribed class, accounting for 57% of prescriptions (n = 2,065), followed by CCBs at 49% (n = 1,787), ACEIs at 40% (n = 1,433), diuretics at 37% (n = 1,328), ARBs at 28% (n = 1,020) and other anti-hypertensive drugs at 4% (n = 126) (Figure 1A). Further analysis revealed that 33% (n = 1,172) of the anti-hypertensive users were prescribed as monotherapy, 30% (n = 1,083) received dual therapy, 23% (n = 832) were prescribed triple therapy, and 14% (n = 513) were prescribed four drugs (Figure 1B).

Prevalence and prescribing pattern of anti-hypertensive drugs. Panel A presents the prevalence of anti-hypertensive class prescription. Panel B presents the prescribing pattern of anti-hypertensive drugs among users. Panel C presents the prescription pattern within each specific drug class users. CCB, calcium channel blocker; BB, beta blocker; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker.
When analyzing the pattern of each anti-hypertensive class prescription, 27% of CCBs were prescribed as monotherapy, followed by BBs at 24% and ACEIs at 19%. In dual therapy, ACEIs and CCBs were most commonly prescribed, comprising 32% and 29% of prescriptions, respectively (Figure 1C). In triple therapy, diuretics, ACEIs, and ARBs were the most commonly prescribed, accounting for 37%, 29%, and 29%, respectively. In quadruple therapy, other anti-hypertensive drugs and diuretics were the most commonly prescribed, accounting for 62% and 32%, respectively (Figure 1C).
Further analysis was conducted to determine the characteristics of users within each anti-hypertensive drug class. The results revealed that users of diuretics, ARBs, and CCBs were older, whereas user of other anti-hypertensive drugs and ACEIs were younger compared to nonusers within the anti-hypertensive drug users cohort (Table 2). Additionally, user of other anti-hypertensive drugs and ACEIs exhibited higher CrCl values, while diuretics users had lower CrCl values compared to nonusers. Notably, all anti-hypertensive drug users, except those prescribed BBs, had higher CCI scores compared to nonusers (Table 2).
Characteristics of Patients Prescribed Each Class of Anti-Hypertensive Drugs.

CCB, calcium channel blocker; BB, beta blocker; ACEI, angiotensin converting enzyme inhibitor; ARB, angiotensin receptor blocker; CrCl, creatinine clearance; CCI, Charlson comorbidity index; NPM, number of prescribed medications. *P < 0.05, **P < 0.01, ***P < 0.001.
Further analysis revealed that BB and ACEI users were more likely to be male (OR = 1.4 and 1.8, retrospectively), whereas CCB, ARB, and diuretics users were predominantly female (OR = 1.25, 1.25, and 1.1, respectively) (Table 3). Diabetes mellitus was common among all anti-hypertensive drugs users, except BBs (OR = 0.8). Osteoporosis was more prevalent among CCB and other anti-hypertensive drugs users (OR = 1.6 and 2.1, respectively), but less common among BB and ACEI users (OR = 0.6 and 0.8, respectively) (Table 3). Gastritis- related diseases were more prevalent among CCB, BB, and diuretics users (OR = 1.3, 1.2, and 1.3, respectively), whereas constipation was more common observed in users of CCB, diuretics and other anti-hypertensive drugs (OR = 1.4, 1.3, and 1.7, respectively), but less prevalent among ACEI users (OR = 0.8). Coagulation disorders were less prevalent among CCB users (OR = 0.8), but more common among ACEI, ARB, diuretics, and other anti-hypertensive drugs users (OR = 1.7, 1.2, 2, and 2, respectively).
Prevalence of Gender and Comorbidities Among Each Anti-Hypertensive Class Users.
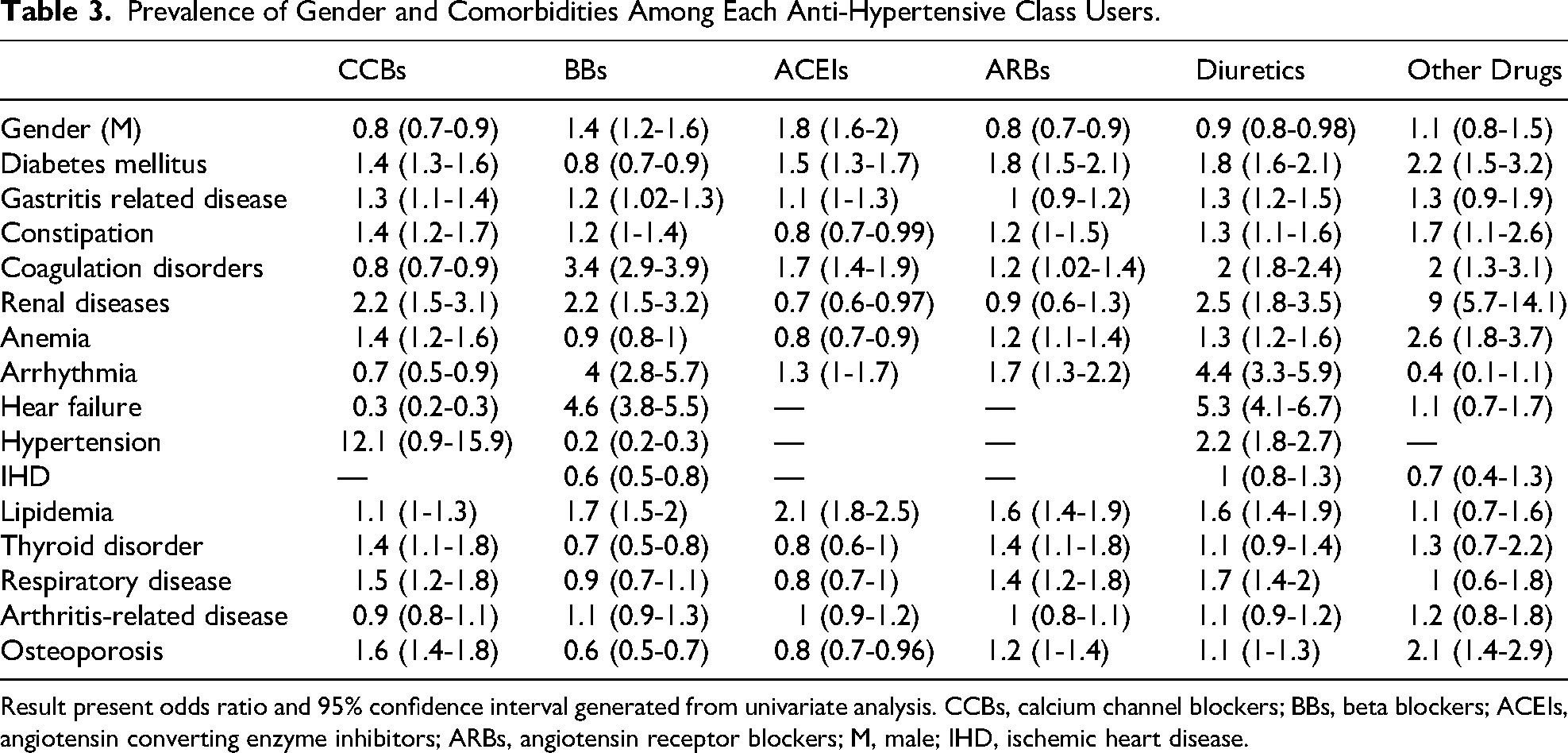
Result present odds ratio and 95% confidence interval generated from univariate analysis. CCBs, calcium channel blockers; BBs, beta blockers; ACEIs, angiotensin converting enzyme inhibitors; ARBs, angiotensin receptor blockers; M, male; IHD, ischemic heart disease.
A univariate analysis was conducted to determine the difference in the prescription pattern between older and middle-aged patients. The analysis revealed that among anti-hypertensive drug users, older patients were more likely to be female (53% vs 43%, P < 0.001), had higher CCI scores (7 vs 4, P < 0.001), but exhibited lower mean CrCl (73 vs 107, P < 0.001) and a lower NPM (6 vs 8, P < 0.001) compared to middle-aged patients (Table 4). Notably, older patients had a higher prevalence of diabetes mellitus (50% vs 41%, P < 0.001), gastritis-related disease (56% vs 43%, P < 0.001), constipation (18% vs 8%, P < 0.001), coagulation disorders (75% vs 59%, P < 0.001), and osteoporosis (40% vs 34%, P = 0.001) compared to middle-aged patients (Table 4). In terms of cardiovascular diseases, older patients were more likely to have heart failure (83% vs 80%, P = 0.007), hypertension (86% vs 82%, P = 0.001), and hyperlipidemia (74% vs 65%, P < 0.001) compared to middle-aged patients (Table 4).
Characteristics of Anti-Hypertensive Drug Users Classified Into Older Versus Middle-Aged Patients.

CrCl, creatinine clearance; CCI, Charlson comorbidity index; NPM, number of prescribed medications.
When comparing the prescription patterns of anti-hypertensive drugs between older and middle-aged patients, the analysis revealed that middle-aged patients were more likely to be prescribed a single anti-hypertensive drug (37% vs 27%, P < 0.001), less likely to receive triple therapy (20% vs 26%, P < 0.001) or four medications (13% vs 17%, P < 0.001) compared to older patients (Figure 2). Remarkably, older patients were more likely to be prescribed diuretics (46% vs 30%, P < 0.001), CCBs (52% vs 48%, P = 0.02), and ARBs (31% vs 26%, P < 0.001) compared to middle-aged patients (Figure 3).

Difference between middle-aged versus older patients in terms of the pattern of prescribing anti-hypertensive drug.

Prevalence of specific anti-hypertensive class prescription among older versus middle aged patients. Some patients were prescribed more than one drug. CCBs, calcium channel blockers; BB, beta blockers; ACEIs, angiotensin converting enzyme inhibitors; ARBs, angiotensin receptor blocker. *P < 0.05, **P < 0.001.
Further analysis to illustrate gender-specific differences in anti-hypertensive prescribing patterns was conducted (Figure 4). Female patients were more likely to receive CCBs (52% vs 47%, P < 0.01) and ARBs (31% vs 26%, P < 0.01), whereas male patients more frequently received BBs (61% vs 54%, P < 0.001) and ACEIs (46% vs 33%, P < 0.001) (Figure 4B). Additionally, the intensity of anti-hypertensive therapy differed between gender, with female patients more commonly receiving monotherapy (35% vs 30%) and male patients more frequently prescribed combination regimens (Figure 4A, P = 0.002). Importantly, the mean number of anti-hypertension drugs differ significantly between male and female patients (2.3 (SD: 1.1) vs 2.2 (SD: 1.1), P = 0.002).

Prevalence of specific anti-hypertensive class prescription among older versus middle aged patients. Some patients were prescribed more than one drug. CCBs = Calcium channel blockers; BB, beta blockers; ACEIs, angiotensin converting enzyme inhibitors; ARBs, angiotensin receptor blocker. *P < 0.05, **P < 0.01, ***P < 0.001.
The binary regression analysis indicated that anti-hypertensive drug prescriptions were positively associated with increasing age but negatively associated with higher CCI scores (Table 5). Being female increases the likelihood of BBs (OR = 1.7) and ACEIs (OR = 2.1) prescriptions. Diabetes mellitus increased the likelihood of ARBs prescriptions (OR = 1.2) but was negatively associated with BB prescriptions (OR = 0.6) (Table 5).
Factors Associated With Anti-Hypertensive Drug Prescribing.

CCBs, calcium channel blockers; BBs, beta blockers; ACEIs, angiotensin converting enzyme inhibitors; ARBs, angiotensin receptor blockers; CrCl, creatinine clearance; CCI, Charlson Comorbidity Index; NPM, number of prescribed medications. *P < 0.05.
Interestingly, the multinominal regression analysis revealed that increasing age was negatively associated with the total number of anti-hypertensive drug prescriptions (Table 6). In contrast, higher CCI scores and male gender were positively associated with an increased number of prescribed anti-hypertensive drugs.
Factors Associated With Total Number of Anti-Hypertensive Drug Prescriptions.
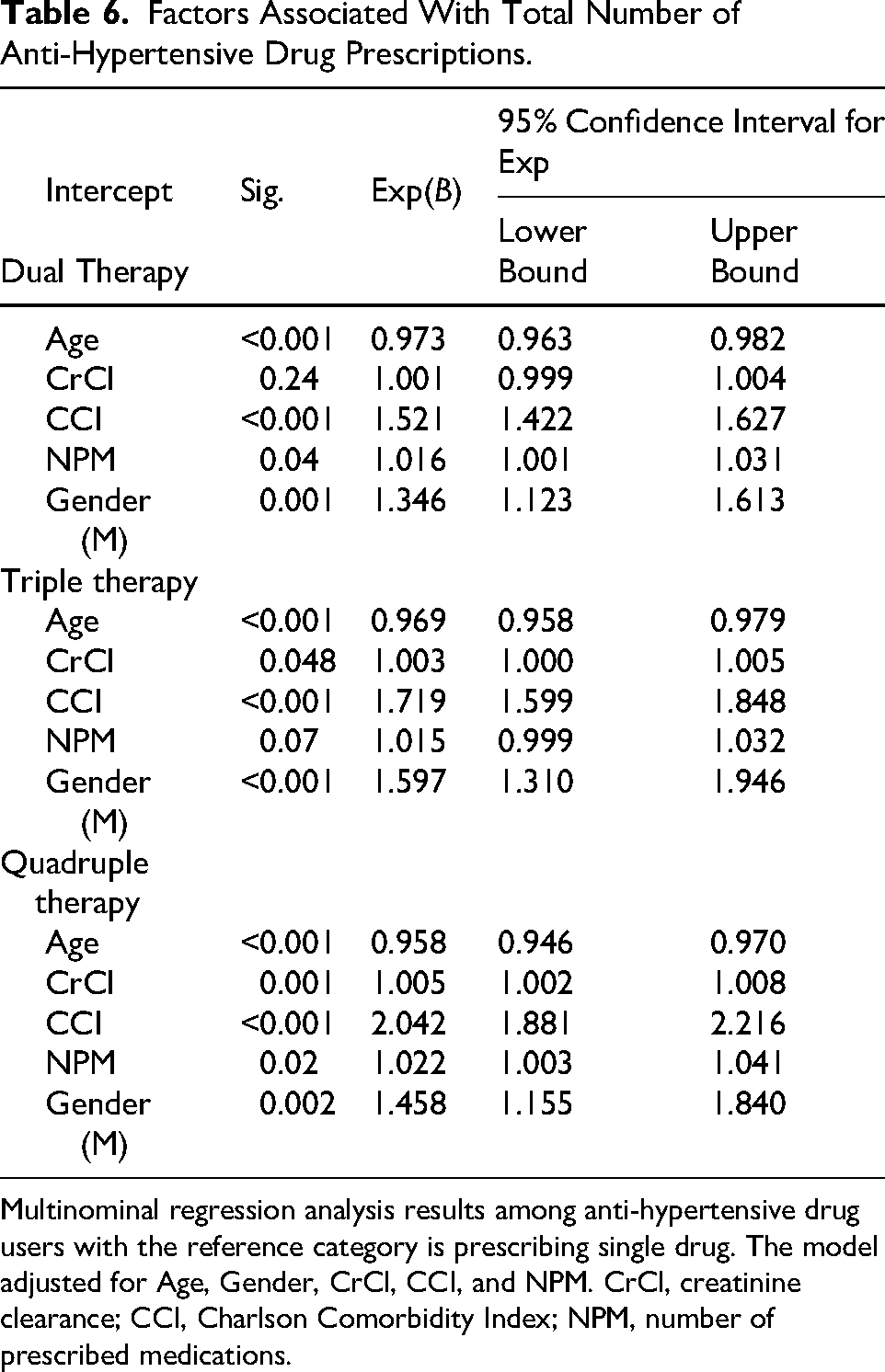
Multinominal regression analysis results among anti-hypertensive drug users with the reference category is prescribing single drug. The model adjusted for Age, Gender, CrCl, CCI, and NPM. CrCl, creatinine clearance; CCI, Charlson Comorbidity Index; NPM, number of prescribed medications.
Discussion
This study aimed to examine the current prescribing pattern of anti-hypertensive medications among patients aged 40 years and older and to identify factors influencing these patterns. The prevalence of anti-hypertensive prescriptions was 62%, with BBs and CCBs being the most prescribed classes. A key observation was the high prevalence of BB prescriptions compared to other anti-hypertensive classes. This pattern contrasts with the global trend, where the prescription rates of ACEIs, ARBs, and CCBs have increased over the past two decades.6,23 While, International guidelines (such as the Eighth Joint National Committee and the European Society of Hypertension) encourage ACEIs, ARBs, and thiazide diuretics as an initial treatment of uncomplicated hypertension, the reported prescribing patterns may also reflect physician-level preferences, institutional practices, and the high burden of cardiovascular comorbidities in this cohort.3,4 In addition, CCBs are currently recommended as first-line hypertension treatment in many international guidelines, particularly for elderly patients and certain ethnic population.24,25 The significant prevalence of CCB prescriptions observed in this cohort aligns with current guideline recommendations, particularly considering the demographic characteristics of the study cohort.
Furthermore, BBs constituted the most commonly prescribed class for monotherapy within this cohort. Previous research has shown that ACEIs are the most commonly prescribed monotherapy drugs. 5 However, similar patterns of high BBs prescribing have been seen in some countries.4–6,26,27 The significance of the incidence of ischemic heart disease (57%) and heart failure in our cohort certainly played a major role in this prescription pattern. BBs have been identified as treatments for lowering cardiovascular morbidity and mortality in patients with heart failure and previous myocardial infarction,28,29 and their use in these populations is strongly supported by clinical guidelines. 29 However, in patients without definitive cardiac indications, recent hypertension guidelines generally recommend renin–angiotensin system inhibitors, CCBs, or thiazide-type diuretics as first-line treatments for uncomplicated hypertension. 3 Consequently, the identified prescribing pattern may reflect a combination of comorbidity-influenced decision-making and existing prescribing traditions. These findings highlight the complexity of selecting anti-hypertensive medications in patients with multiple cardiovascular conditions and illustrate the need for personalized therapeutic strategies that adhere to advancing evidence-based guidelines.
Another notable finding is the significant gender-based differences in the pattern of anti-hypertensive medication prescriptions. Male patients were more likely to be prescribed ACEIs and BBs, whereas female patients were more often prescribed diuretics and ARBs. These variations may be attributed to differences in drug efficacy, side effect profiles, and comorbidities between genders, as highlighted in previous studies.8,30,31 For instance, ACEIs are often prescribed to male patients because of their proven efficacy in reducing cardiovascular mortality. 11 In contrast, diuretics may be preferred in female for their effectiveness in lowering blood pressure and their protective role in preventing heart failure, especially among older women. 12 Female patients, particularly post-menopausal, have a higher risk of osteoporosis, making diuretic-induced calcium retention a potential therapeutic benefit. 32 However, this advantage must be considered against an elevated risk of electrolyte imbalances and metabolic disturbances, which are more common in women. Understanding these gender-based differences is essential for customizing treatments for individual patients. By acknowledging these factors, healthcare providers can enhance the efficacy of anti-hypertensive therapy and improve patient adherence.
The higher prevalence of ARB prescriptions in female patients relative to ACEIs may be attributed to differences in tolerance among these drug subclasses. ACEIs are known for inducing a chronic dry cough, which has been recorded with greater frequency in women. 33 This ADR frequently results in stopping ACEIs and switching to ARBs, which offer similar renin-angiotensin system inhibition without the bradykinin-induced cough. Moreover, concerns about angioedema linked to ACEIs may affect physician preferences in vulnerable patients. 34 Consequently, differing tolerability profiles, rather than safety considerations connected to pregnancy, may partially explain the observed sex-based differences in prescribing practices.
Another significant finding from this study is that diabetes mellitus was associated with lower odds of BB prescriptions by 70%, while increasing the odds of prescribing ARBs by 20%. BBs and diuretics are known to have adverse metabolic effects that may increase the risk of diabetes mellitus incidence, 35 and BBs can also mask the symptoms of hypoglycaemia. 36 In contrast, CCBs have neutral effects on glucose tolerance, whereas ACEIs and ARBs may delay the onset of diabetes mellitus and provide kidney protection. 37 Previous studies reported that 15%–20% of hypertensive patients may develop glucose intolerance, with diabetic female individuals at higher risk for worse cardiovascular outcome compared to male counterparts. 38 Since diabetes mellitus is a major risk factor for cardiovascular morbidity and mortality, the appropriate selection of anti-hypertensive medications is critical. ACEIs and ARBs have been shown to delay the progression of diabetic nephropathy and reduce albuminuria, providing dual benefits in this patient cohort. 38 The observed negative association between BBs and the preference for ARBs in diabetic patients in our study reflects adherence to current clinical guidelines and should be encouraged to minimize ADRs.
Renal function is an important factor in the selection of anti-hypertensive medications, owing to safety concerns and the reno-protective properties of some classes, such as ACEIs and ARBs, in chronic kidney disease (CKD). 39 Despite the inclusion of CrCl in multivariable models, the total group exhibited reasonably intact renal function, with a low prevalence of recorded renal disease (4%). Such an outcome may have constrained the capacity to identify differential prescribing patterns according to CKD severity. The cross-sectional design restricted the assessment of dose adjustments or longitudinal fluctuations in renal function that could affect therapeutic modifications. Future research targeting CKD populations might improve understanding of renal function–guided prescribing strategies.
Another important finding is the significant differences in prescribing patterns according to age. Older patients (aged ≥ 65 years) were more likely to be prescribed multiple anti-hypertensive medications, including triple and quadruple therapy. A similar recent study conducted in Aseer Region of Saudi Arabia reported that the majority of the hypertension patients were aged 55 years and older. 40 While combination therapy is often required to achieve optimal blood pressure control in this population, polypharmacy raises concerns regarding ADRs and drug-drug interactions.7,8,10,41 A recent study reported that polypharmacy poses a significant concern for hypertension patients, increasing risk of ADRs and drug-drug interactions. 42 This finding indicates the need for continuous monitoring and re-evaluation of anti-hypertensive therapy in older patients to enhance care. Multidisciplinary collaboration, involving cardiologists, endocrinologists, nephrologists, and clinical pharmacists can improve treatment precision and patient outcomes.
Interestingly, this study may reflect cautious prescribing approaches in older adults as increasing age was associated with a higher likelihood of being prescribed monotherapy, and a lower likelihood of combination therapy. This may reflect a good clinical practice, as prescribers might avoid combination therapy in older patients to mitigate the risk of orthostatic hypotension and falls, which are well-known complications of anti-hypertensive therapy. 43 Furthermore, this relationship may explain the observed negative association between higher CCI scores and the overall anti-hypertensive use. However, the finding that a higher CCI score was associated with greater use of combination therapy, rather than monotherapy, raise concern, as it may increase the risk of ADRs and drug-drug interactions in patients with multiple comorbidities. 44
Another key finding is the high prevalence of constipation in patients receiving CCBs, with a 40% increase likelihood of experiencing constipation. CCBs, particularly dihydropyridines like amlodipine, are known for their ability to induce smooth muscle relaxation, potentially resulting in delayed colonic transit and subsequent constipation. 39 Despite their efficacy in lowering blood pressure, the gastrointestinal adverse effects of CCBs are frequently lead to treatment discontinuation or nonadherence. This association emphasizes the importance of monitoring and managing ADRs to maintain long-term adherence. Strategies to mitigate CCBs-induced constipation include increasing dietary fiber intake, using stool softeners, or switching to alternative anti-hypertensive medication when appropriate. 45 Physicians should proactively address gastrointestinal symptoms and provide timely interventions to improve patient comfort and compliance. However, due to the cross-sectional design, it is hard to ascertain whether the administration of CCBs preceded the diagnosis of constipation or the reverse.
This study reported a relatively low proportion of confirmed hypertension diagnoses (51%) compared to the higher rate of anti-hypertensive use (62%). BBs, ACEIs and ARBs are frequently prescribed for patients with heart failure and ischemic heart diseases because of their well-established mortality benefits, even in the absence of primary hypertension.46,47 This therapeutic overlap is particularly relevant in older patients, who often exhibit several comorbidities and overlapping cardiovascular risk factors. 10 Understanding these complex prescribing patterns is critical for accurately interpreting real-world treatment patterns and recognizing opportunities for guideline optimization, particularly in populations with elevated cardiovascular risk.
A principal strength of this study is its large sample size, which enhances the generalizability of the findings within the Saudi Arabian context. The inclusion of diverse patient population, stratified by age, gender, and comorbidities, facilitates a comprehensive examination of anti-hypertensive prescription patterns and their associated factors. A significant strength of this study is the application of robust statistical methods, such as logistic regression and stratified analyses, which effectively adjust for confounding factors, hence improving the reliability and validity of the results.
However, some limitations must be acknowledged. The observational cross-sectional study design limits causal inference. The current study identifies associations between patient characteristics and prescribing patterns, but it cannot determine if specific comorbidities directly influenced prescribing decisions. Therefore, prospective studies are required to clarify temporal and causal relationships. In addition, the retrospective design introduces potential biases due to incomplete or missing data. Although efforts were made to verify prescriptions and patient characteristics, reliance on electronic medical records may lead to underreporting or misclassification. Furthermore, this research did not include prescriber-level factors. Variability in medical training, subspecialty expertise, personal clinical experience, and adherence to revised guideline recommendations may have influenced prescribing practices. The absence of prescriber identifiers and indicators of guideline adherence in the dataset implies that potential prescribing bias cannot be excluded. Further studies employing physician-level data and institutional prescribing guidelines could provide more understanding of diversity in decision-making.
Some potentially significant confounding variables were missing in the dataset. Lifestyle factors such as smoking status, dietary habits, physical activity levels, and body mass index were not recorded. Socioeconomic factors, like educational status and income level, were likewise inaccessible. In addition, the evaluation of drug adherence was not performed, which may influence decision on treatment escalation or modification. The absence of these variables raises the risk for residual confounding; thus, the observed associations should be evaluated with caution. The current study lacked longitudinal data regarding blood pressure management and clinical outcomes, such as cardiovascular events, hospitalization, or mortality rates. As a result, the clinical efficacy and prognostic significance of the identified prescribing patterns could not be evaluated. The study focused exclusively on identifying associations between patient characteristics and the selection of anti-hypertensive medications. Future longitudinal studies incorporating blood pressure trajectories and cardiovascular outcomes are required to evaluate the practical effectiveness of these prescribing approaches.
The study was conducted at a single tertiary care hospital in the Eastern Region of Saudi Arabia, where prescribing preferences may reflect regional healthcare strategies, institutional guidelines, and formulary accessibility. Therefore, the results may not be readily applicable to other healthcare systems or populations exhibiting distinct demographic and clinical characteristics. The large sample size and the inclusion of a diverse cardiovascular outpatient demographic may enhance applicability to analogous tertiary-care settings. In addition, the relatively low prevalence of advanced renal impairment in the study cohort may limit generalizability to patients with moderate-to-severe CKD.The inclusion of diverse patient demographic, stratified by age, gender, and comorbidities, facilitates an exhaustive analysis of anti-hypertensive prescribing patterns and their associated clinical factors.
The inclusion and exclusion criteria resulted in a study population primarily composed of older patients with significant cardiovascular comorbidities, notably elevated rates of heart failure and relatively low rates of renal impairment. This selection bias must be considered when interpreting the results, since it may restrict their applicability to broader hypertensive populations. It is important to indicate that the study did not assess patient adherence to anti-hypertensive medications, which may influence interoperation of the outcomes. Moreover, although patients with a confirmed diagnosis of hypertension were included, the primary analysis was concentrated on those receiving anti-hypertensive therapy. The reported prescribing prevalence may underrepresent untreated hypertensive people and should not be regarded as an accurate indicator of actual hypertension prevalence in the general population. Comorbidities were obtained from review of medical records; however, the Rx-Risk Comorbidities Index was applied to help mitigate omissions in medical records. This application led to the exclusion of mineralocorticoid receptor antagonists and loop diuretics from anti-hypertensive list, as their primary indication was determined to be the management of heart failure and fluid retention associated with heart failure based on Rx-risk tool application.46–49 Furthermore, while medication burden was quantified using the number of prescribed drugs, the study did not assess the appropriateness of therapy, potential drug–drug interactions, or medication-related adverse events. These factors are important components of medication safety and warrant further investigation. Specific subclasses of anti-hypertensives were grouped into broader groups to ensure statistical stability due to low individual frequencies. The approach may have diminished heterogeneity among particular agents within those groups of agents. Finally, the analysis provides a cross-sectional overview of anti-hypertensive prescriptions during the initial documented outpatient visit over the study period. It was difficult to differentiate between newly commenced anti-hypertensive therapy and established chronic treatment. Consequently, prescribing patterns may indicate both historical prescribing choices and recent treatment modifications.
Lastly, the current study provides several actionable insights for improving hypertension management. The overuse of BBs highlights the need to reinforce adherence to international guidelines, particularly in patients without specific indications for their use. The observed gender-based differences in prescribing patterns emphasize the importance of personalized treatment strategies that account for gender-specific pharmacodynamic responses and comorbidities profiles. In older patients, it is crucial to conduct regular medication review to manage polypharmacy and reduce the risks of ADRs and drug-drug interactions. Additionally, addressing common ADRs can improve patient adherence and clinical outcomes. A multidisciplinary approach that includes primary care physicians, specialists, and pharmacists is essential to optimizing anti-hypertensive therapy, reducing complications, and promoting sustained health outcomes. Furthermore, continuous professional development programs and audit-based interventions can further refine prescribing patterns to align with current evidence-based guidelines.
Conclusion
This study provides valuable insights into anti-hypertensive prescribing patterns within a Saudi Arabian cohort, highlighting key trends, potential disparities, and areas for enhancement. The overuse of BBs, gender-based differences in medication selection, and the appropriate management of anti-hypertensive therapy in diabetic and older patients emphasize the need for personalized treatment strategies. The findings emphasize the importance of addressing polypharmacy and controlling common side effects, such as CCB-induced constipation, to enhance adherence and improve therapeutic outcomes. Deviations from guideline-recommended therapies, such as the overuse of BBs and gender-specific prescribing trends, highlight the need for more personalized, context-specific treatment strategies to enhance therapeutic effectiveness and reduce cardiovascular risk. Continuous professional development programs and audit-based feedback mechanisms could promote the alignment of prescribing practices with emerging evidence-based recommendations.
Footnotes
Acknowledgments
The authors extend their gratitude to the medical records and information technology staff at QCH for their invaluable support in reviewing and collecting patient data.
Ethical Approval and Informed Consent
This study was a retrospective, cross-sectional descriptive analysis of secondary data. Data collection was approved by the Institutional Review Board (IRB) at Mohammed Al-Mana College for Medical Sciences (SR/RP/79, Approval Date 17 February 2022) and by the Qatif Central Hospital’s IRB (QCH-SRECO 19-2022, Approval Date 8 June 2022). Data was collected between 1st of August 2022 and 20th of February 2023 from the hospital’s information technology department. All participants were deidentified and a waiver of consent collection was approved by IRB as data was collected retrospectively.
Authors’ Contributions
Dr Aymen A. AlQurain: Conception, Data collection, data analysis, writing first draft, evaluating and modifying and approving final manuscript. Mr Arif Aldihani, Miss. Hadeel Almousa, Miss. Gofran Alkhalaf, Miss. Fatimah Alqurayn: Data collection and coding and preparing data for analysis, data analysis, writing first draft and approving final version. Mrs Luma Ameer, Mrs. Sherihan Ghosn, Mrs. Marwa Algoraini, Miss Samaher Al-Shaibi, Mrs. Ghadeer Alowaywi, Mr Hassan Althabet, Dr Reem Ashoor, Dr Afnan Alshnbari, Dr Salah Abohelaika, Dr Shahad Alghamdi, Dr Abdulkhaliq Alsalman, Dr Bander Alanzi, Dr Fadhel Alomar: Support in writing the first draft of the introduction, methods, results, and discussion, interpreted the data, and edited and approved the final manuscript.
Data Availability
The datasets analyzed during the current study are available upon reasonable request. Data will be shared for scientific purposes with researchers whose proposed use has been approved by the research team.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors sincerely thank the Research Development and Innovation Authority (RDIA) for their ongoing support, as this work received partial funding from RDIA, grant (ID: 12990-iau-2023-iau-R-3-1-HW).