
Abstract
Introduction
Atrial fibrillation (AF) is the most common type of arrhythmia, affecting approximately 3% of the population aged >20 years and 9% of the population aged >80 years old. 1 The incidence of AF is increasing in the ageing population. Restoration of the sinus rhythm remains integral to treating this type of arrhythmia. Electrical cardioversion (ECV) is more effective than pharmacological cardioversion (PCV) in restoring sinus rhythm. 1 Although ECV is widely used and generally safe, complications can occur. Complications secondary to ECV can be divided into thromboembolic events (0.7%), arrhythmias (primarily bradyarrhythmias, 0.9%), and hemodynamic decompensation.2–4 Frailty and multimorbidity in older adults are likely associated with a higher risk for this procedure. ECV is a painful procedure that requires anesthesia or at least deep sedation. Deep sedation is a controlled state of depressed consciousness or unconsciousness. Various short-acting drugs (eg, propofol, midazolam, and etomidate) are used for this purpose, each of which has advantages and disadvantages. 5 Furthermore, the safety of these drugs, when used without the assistance of anesthesiology teams, is debated among cardiologists. Anesthesiologist participation may introduce logistical challenges, increase waiting times, and additional costs.
This single-center retrospective study aimed to assess the safety of ECV without assistance from anesthetists. We also evaluated the efficacy and safety of this procedure in older adults (≥80 years) compared to the younger population.
Methods and Materials
We retrospectively enrolled 218 patients hospitalized for electric cardioversion of AF at the Department of Heart Disease Medical Center of Postgraduate Education between January 2018 and December 2021. The patients were admitted to our emergency department for ECV, both for planned elective cardioversion and after ineffective PCV of paroxysmal AF. We collected data on variables such as comorbidities and risk factors; clinical, echocardiographic findings and laboratory findings; chronic pharmacological treatment before admission; and antiarrhythmic drugs used in the emergency department to PCV (if applicable). CHA2DS2VASc score and HAS-BLED score were calculated for each patient. The database contains information about the drugs used for sedation, the amount of energy used, the number of outages, complications after cardioversion (bradyarrhythmias, thromboembolic events, cardiogenic shock, and death), the effectiveness of ECV, and AF recurrence during hospitalization.
All patients with an AF duration >48 h who underwent ECV were anticoagulated for at least 3 weeks. If there was an uncertain duration of AF or any doubts regarding anticoagulation status, a transesophageal echocardiogram was performed before the procedure to exclude a left atrial thrombus.
Before ECV, each patient underwent a physical examination with blood pressure measurement. Blood samples were collected to measure erythrocyte and serum creatinine levels. All patients provided written informed consent prior to ECV. The procedure was performed in the intensive care cardiac unit (ICCU). The team performing the procedure comprised a cardiologist and 2 nurses trained in resuscitation. The standard ECV procedure involves the use of defibrillator pads on the right side of the sternum and over the left scapula. The synchronized delivery of energy shock began at 150 J and was increased to 200 and 300 J, as needed. Observation of patients after shock takes approximately 2 h and is longer in cases of bradyarrhythmia or hypotonia. Propofol is a general anesthetic used for deep sedation. The starting dose of propofol was a bolus of 0.8 mg per kg body mass, which was fractionally increased every minute to the desired sedation level or to a maximum dose of 1.5 mg/kg. A cardiologist continuously assessed the sedation level. Transdermal oxygen saturation and electrocardiographic findings were monitored continuously during the procedure. The blood pressure was measured before and after the procedure. Each patient received oxygen supplementation with a 100% oxygen mixture.
To achieve our aims, we divided the study population into 2 groups: those aged <80 years and those aged ≥80 years. We compared clinical characteristics, risk factors, as well as clinical, laboratory, and echocardiographic findings between the study cohorts. We assessed the effectiveness and safety of ECV in younger and older patients.
Finally, follow-up clinical data were collected for up to 2 years (median: 962 days). Using telephone contact, we obtained information (from 90% patients) about the late recurrence of AF.
This study was approved by the Institutional Bioethical Committee. The ethics committee waived the requirement for informed consent due to the retrospective nature of the study.
Statistical Analysis
Normally distributed data are presented as mean ± standard deviation, and were compared between groups with Student's t test. Non-normally distributed continuous variables are reported as percentiles (median, 25th, and 75th percentiles) and compared across 2 groups by Mann–Whitney test. Categorical data are reported as counts and percentage. The significance of differences in proportions was verified by Pearson's chi-squared test or Fisher's exact test. A multivariable logistic regression model with backward elimination was used to identify independent predictors of atrial fibrillation during hospitalization. Variables that were associated with this endpoint in univariate analysis with a significance level of P < .2 were entered into the initial model. The goodness of discrimination was assessed with the C-statistic AUC [95% CI]. All the tests performed were 2-sided where P-value of < .05 was considered statistically significant. Statistical software of SAS (version 9.4, SAS Institute Inc, Cary, North Carolina, USA) was used for data analysis.
Results
We enrolled a total of 218 patients: 73 were ≥80 years and 145 were <80 years old (Table 1). The mean age in the older group was 84.8 years, and that in the younger group 66.7 years (P < .001), with females being the majority of the population. The older group had a significantly higher incidence of hypertension, heart failure, renal failure, and coronary artery disease as well as a lower body mass index and proportion of former and current smokers than the younger group. The younger group had significantly lower CHA2DS2VASc and HAS-BLED scores than the older group. In terms of chronic oral anticoagulation, the older group was more often treated with rivaroxaban and less often with vitamin K antagonists (VKAs). The younger group required a higher mean dose of propofol to achieve deep sedation (Table 2). The total success rate of ECV was high and comparable between the groups (97.3% vs 96.5%, P = 1.00). There were no statistically significant differences in the incidence of pauses >5 s or AF recurrence during hospitalization.
Patients Characteristics.

Data are presented as the number (percentage) of patients unless otherwise indicated. Bolded entries indicate a statistically significant difference between groups (P-value < 0.05).
Abbreviations: AF, atrial fibrillation; CAD, coronary artery disease; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CRT, cardiac resynchronization therapy; ECV, electric cardioversion; ICD, implantable cardioverter defibrillator; LAA, left atrial appendage; LVEF, left ventricular ejection fraction; TIA, transient ischemic attack; VKA, vitamin K antagonist; ECV, electrical cardioversion.
Electrical Cardioversion Data.

Data are presented as number (percentage) of patients unless otherwise indicated. Bolded entries indicate a statistically significant difference between groups (P-value < 0.05).
Abbreviations: AF, atrial fibrillation; ECV, electrical cardioversion.
Among the study groups, 47 (64.4%) and 142 patients (74.5%) in the older and younger groups, respectively, underwent unsuccessful PCV before ECV (Table 3). The success rate of ECV was comparable between the study groups. There were no differences in the incidence of pauses >5 s between groups. The multivariate analysis demonstrated that a high frequency of AF recurrence before admission (>1 per month) and increased systolic blood pressure were independent predictors of arrhythmia recurrence during hospitalization (Table 4). Chronic treatment with ACEi is associated with the maintenance of sinus rhythm before discharge.
Subgroup of Patients After Unsuccessful Pharmacological Cardioversion Before Electric Cardioversion.
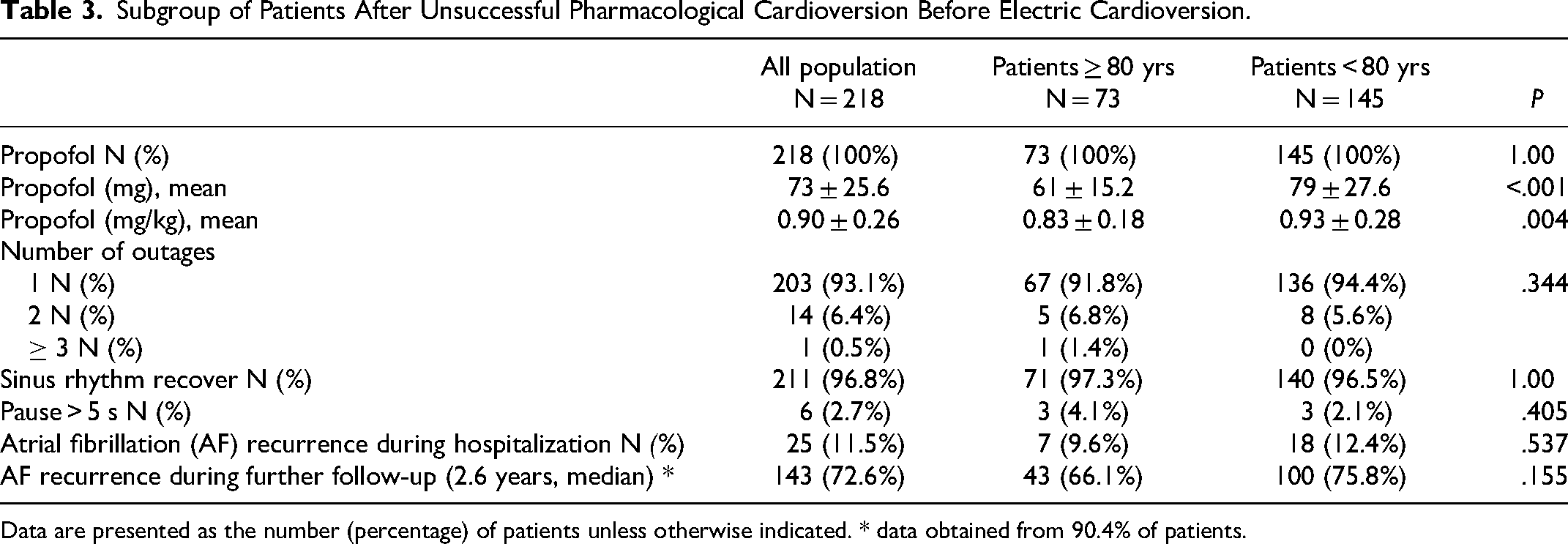
Data are presented as the number (percentage) of patients unless otherwise indicated. * data obtained from 90.4% of patients.
Independent Predictors of Atrial Fibrillation Recurrences During Hospitalization. Results of Multivariable Logistic Regression Analysis.

AUC [95% CI]: 0.779 [0.679-0.880]. Abbreviations: AUC, area under curve; Cl, confidence interval; SBP, systolic blood pressure; ACEi, angiotensin-converting enzyme inhibitor.
Discussion
The main finding of this study was that ECV performed in unselected patients by experienced cardiologists and nurses in the ICCU was safe and effective. The lower number of professionals involved in this procedure was associated with reduced delay, improved patient satisfaction, decreased costs, and minimized logistical challenges associated with the coordination between cardiologists and anesthesiologists. It is important to be careful and precise in each period: Preparation for the procedure, sedation and shock delivery, and postsedation observation. In our study, patients were qualified for ECV after checking for adequate anticoagulation, assessment of baseline ECG, and determination of the potassium level in the blood on the day of ECV. Blood pressure, transdermal oxygen saturation, and cardiac rhythm were monitored directly in each patient before the procedure. The subsequent step was sedation and the selection of appropriate drugs. To the best of our knowledge, there are no recommendations for the most appropriate sedative therapy for ECV. Several drugs have been investigated and described in the literature for sedation during ECV, including midazolam,6–8 diazepam,9–11 propofol,7,12–14 methohexitone,12,13 and thiopentone,6,11,15,16 Propofol is one of the frequently used agents for deep sedation during ECV, which is also used in our department. In terms of advantages, propofol offers rapid (<60 s) and short anesthetic action (3-8 min), allowing for fast recovery. 17 However, propofol may be associated with serious side effects, including the cardiovascular risk of hypotension and bradycardia, and respiratory effects, such as hypoventilation, hypoxemia, and apnea. 18 Previous studies and meta-analyses have reported sporadic occurrences of critical side effects of propofol (eg, laryngospasm, need for intubation, and aspiration) comparable to those of other sedatives.19–21 Furthermore, when adverse effects occurred, the patients recovered smoothly and rapidly. These results conform to the observations in our study population. We did not observe any episodes of apnea or hypotension, and intubation was not required. It must be noted that deep sedation should be performed by emergency physicians who are qualified to supervise all levels of sedation and are skilled in ventilation, airway management, and resuscitation, which are necessary for complications. In our study, all ECV procedures were performed in an ICCU equipped with monitoring, medical gas supply system, and resuscitation equipment.
Several tests have been used to evaluate recovery from deep sedation or anesthesia.22–25 In our study population, we did not perform dedicated tests to evaluate the recovery period. In this phase, we monitored the patients closely (ECG recording, pulsimeter oxygen, blood pressure check, and rhythm monitoring) with appropriate maneuvers to maintain the patency of the airways, such as jaw lift and hyperextension of the neck. In all cases, total consciousness was restored after a few minutes. Subsequently, patients were instructed to remain in bed for 2–4 h in the ICCU until complete recovery of their ambulatory capacity.
ECV is associated with complications unrelated to sedation, such as bradyarrhythmias, thromboembolic events, and hemodynamic decompensation. Bradycardia after ECV might be caused by the unmasking of latent tachy-brady syndromes or atrioventricular conduction disturbances as well as possible damage to cardiac conduction induced by electric shock. However, this complication is rare and often transient. Gronberg et al reported that bradycardic complications occurred in 0.9% of electrical cardioversions, with 0.7% occurring in asystole lasting more than 5 s. 26 Advanced age and female sex are predictors of these events. Interestingly, more than 40% of patients with bradycardic complications after ECV require permanent pacemaker placement. Another study indicated that bradyarrhythmic events are highly dependent on age. 27 In contrast, in our study, we did not observe differences in the incidence of asystole lasting more than 5 s between the older population (with a mean age of 84.8 years) and the younger population (with a mean age of 66.7 years). The incidence rates were 4.1% and 2.1% in the older and younger populations, respectively, (P = .405). Interestingly, we did not observe differences between the study groups in terms of the incidence of bradyarrhythmia in patients who underwent ECV after prior administration of antiarrhythmic drugs as PCV.
Cardioversion is associated with thromboembolic risk, which can be reduced by adequate anticoagulation with both non-VKA oral anticoagulants and VKA. In patients with an AF duration >48 h who have not been anticoagulated, transesophageal echocardiography (TOE) is recommended to rule out the presence of any embolic material from the heart cavity. 1 In the present study, neither group experienced thromboembolic complications during the postshock observation. In patients scheduled for ECV who were not or were nonoptimally anticoagulated, we preferred performing TOE on the same day to avoid rescheduling patients for another treatment after a minimum of 3 weeks of oral anticoagulation. This practice is common in most European centers. 28
We have recorded a remarkably high effectiveness rate of 96.8% for ECV in restoring the sinus rhythm. Furthermore, the success rate was comparable between the older and younger population (96.5 vs 97.3%, respectively). Our results align closely with those reported by Morani et al, who reported effective ECV in 98.9% of the cases. 29 Marginally worse results have been reported by Gronberg et al, with a success rate of 94.2% with acute ECV (<48 h) for AF. 30 A multinational rhythm-AF study showed that sinus rhythm could be restored in 89.7% of patients by performing ECV. 31
Unfortunately, despite the high efficacy of ECV, only 30%–35% of patients can maintain sinus rhythm after 1 year.32,33 Among our study population, during the follow-up of 2.6 years we observed high AF relapse among 72.6% patients, without difference between younger and older patients. Tieleman et al 34 showed that AF recurrence is most frequent in the first few days after the procedure. The authors reported that 57% of the patients had a relapse of AF during the first month after cardioversion, with a high proportion (63%) occurring during the first 5 days. A lower incidence of early ECV recurrence (<30 days) was reported in another study (17.3%), with a median time to AF recurrence of 11 days. 30 Consistent with the above findings, we reported AF relapse in 11.5% of patients during hospitalization, without a significant difference between the older and younger study group (9.6 vs 12.4%, respectively). In our study, higher systolic blood pressure and higher frequency of arrhythmia relapse were associated with a recurrence during hospitalization. These states likely promote electrical and structural remodeling; therefore, patients have a higher risk of not maintaining sinus rhythm during short-term observation. In contrast, chronic ACE treatment prevents AF recurrence before discharge. These drugs inhibit the renin-angiotensin system, which is upregulated in the atria of patients with chronic AF. The increased expression of angiotensin-converting enzymes is associated with the activation of downstream signaling pathways involved in fibrogenesis. 35 They also increase the likelihood of long-term sinus rhythm after ECV. 36
Limitations
This was a retrospective observational study posing limitations related to the study design. Data on blood pressure, heartbeat after shock, or blood oxygen saturation before and after the procedure were unavailable in the collected data. Furthermore, there was no information regarding the time required for sedation. Another limitation was the relatively small sample size, which may have been insufficient to include a relatively rare serious event that could have occurred.
Conclusions
Electric cardioversion is an effective and safe procedure regardless of patient age. Sedation with propofol administered by cardiologists was found to be safe. Adverse events were not considered serious or reversible. Considering the possible serious complications, sedation should be performed by emergency physicians with appropriate proficiency in ventilation, airway management, and resuscitation. ECV should be performed in a unit equipped with continuous monitoring capabilities, a medical gas supply system, and resuscitation equipment. These resources are essential for ensuring the safety and well-being of the patient during the procedure.
Footnotes
Acknowledgements
The authors thank all the physicians and nurses who participated in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Postgraduate Medical School of Warsaw, Poland.