
Abstract
This article considers the use of autologous stem cell-derived cardiomyocytes as a novel means to aid venous return. The approach consists of creating external cuffs of engineered heart tissue around vein segments with incompetent or poorly competent valves. The engineered heart tissue cuff prevents distention of the impaired vein segments and aids unidirectional flow by its rhythmic contractions. There appear to be no fundamental limitations to this approach as feasibility of all of the individual components has already been shown. Here, we underline the clinical need for novel ways to treat chronic deep venous insufficiency, review previous research that enabled this approach, consider potential designs of engineered heart tissue cuffs, and outline its advantages and future challenges.
Introduction
This article is submitted to the special issue of Journal of Cardiovascular Pharmacology and Therapeutics devoted to stem cell-based cardiovascular repair. It considers a novel, out-of-the-box tissue engineering approach to aid venous return and overviews experimental evidence supporting the method’s feasibility. The approach offers a new way to treat chronic deep venous insufficiency (CDVI), including venous ulcers, and it can help with other causes of limited flow, including direct muscle injury of lower limbs or their paralysis. Specifically, we consider the use of a patient’s own stem cells (induced pluripotent stem cell [iPSC] or other autologous stem cell sources) to create rhythmically beating cuffs of cardiac muscle that will surround impaired vein segments in lower extremities. 1 Such mini pumps resemble the simplest kinds of hearts observed in low invertebrates or humans, the latter as heart tubes during embryonic development. 2,3 This method is an example of using tissue engineering protocols not only to repair damaged organs but also to design entirely new ones, either outside the organ’s original anatomical location or using the functionality of specialized cells from different tissues.
Basic Physiology of Venous Return
There are several auxiliary physiological mechanisms that assist the heart in its continuous effort to propel blood through vascular beds. There is the so-called “aortic pump” or Windkessel effect of the aorta, which helps propel blood throughout diastole via the aorta’s elastic recoil. There is the “respiratory pump,” which refers to repetitive inflation/deflation cycles of the chest cavity that lead to expansion of compliant veins and increased blood flow to the heart. Finally, there is the “skeletal muscle pump” (also called calf muscle pump), which combats the effect of gravity in upright individuals. The skeletal muscle pump works by compressing nearby veins and requires competent unidirectional valves within those veins. If the skeletal muscle pump mechanism fails (due to lack of skeletal muscle activity, distention and remodeling of the veins, failure of venous valves due to aging, inflammation and thrombosis, or all of the above), it can lead to chronic venous disease.
Chronic Deep Venous Insufficiency
Chronic venous disease is one of the most widespread diseases in the Western world. The number of people who have this disorder is tremendous; an estimated 25% of the adult population have varicose veins and 6% have a more advanced chronic disease. 4 Chronic venous disease can lead to chronic skin changes, phlebitis, venous stasis, ulceration, loss of a limb, and ultimately, death. Lower extremity ulcers are particularly common in diabetic patients, with venous disease accounting for the majority of patients. 5 In the United States alone, the annual cost associated with chronic venous disease treatment is approaching US$3 billion, constituting ∼2% of the total health care budget cost. 6
Currently, there are several treatment options for chronic venous disease that are tailored to specific causes and symptoms. 6 -8 For superficial veins, nonsurgical treatment options include leg elevation, compression stockings, and venoactive medications. Surgical options include vein stripping or vein sealing, with the latter using radiofrequency or laser energy or ultrasound-guided foam sclerotherapy. These options seal the vein and, thus, force blood flow through alternative routes. However, ablation is not a good option when venous reflux occurs in the deep venous system, making correction of deep reflux a challenge. Ligation of incompetent veins, reconstruction of valves, autologous valve transplantation, and anastomosis of major segments of the femoral system are some of the approaches being explored as treatment options. 9 -12 Venous leg ulcers are particularly difficult to treat with only 40% to 70% healed after 6 months of compression therapy. 13 As a result, these leg ulcers can become infected, leading to cellulitis, gangrene, and amputation. Currently, options to treat CDVI, a subset of chronic venous disease, remain limited and several recent review articles outline the need for new approaches to treat this debilitating condition. 9,14
Advances That Enabled the Venous Cuff Concept
The suggested approach has been enabled by recent advances in stem cell biology and tissue engineering. First, protocols have been developed to successfully produce pluripotent stem cells from a patient’s own fibroblasts. 15 Optimization of these protocols has enabled the production of large quantities of cells. 16,17 Furthermore, use of autologous iPSC has largely alleviated immunogenicity concerns although other reprogrammable cell sources can also be used to create allogeneic cardiomyocytes with minimal immunogenicity. 18,19 Second, it is now possible to selectively direct differentiation of pluripotent stem cells toward either a pacemaker or a working ventricular cell phenotype. 20 Both of these phenotypes are necessary to create self-contracting muscular cuffs as detailed subsequently. Third, development of a variety of biocompatible scaffolds has facilitated the creation of pliable and durable macroscopic constructs that are amendable to surgical manipulation. Since the first description of engineered heart tissue (EHT) constructs, 21 different ways to create these constructs have been reported. These approaches include self-assembled cardiac fibers, 22 macroscopic tube-like sheaths, 23 perforated 3-dimensional (3D) layers, 24 thermodetachable sheets, 25 biowires, 26 and other types of engineered cardiac tissue. 27 -30 Importantly, the mechanical strength and tension developed by these constructs are starting to approach those of native cardiac muscle. 24,29
Implantation and Survival of EHT Near and Around Major Blood Vessels
The pioneering work of 2 groups are credited for creating macroscopic beating layers of neonatal rat cardiac myocytes within 31 -33 and near 25,34 large blood vessel walls. The first group directly injected neonatal rat cardiac myocytes into the aortic wall of isogeneic hosts. 32,33 These studies have shown that implanted cells survive, form a functional syncytium, generate measurable pressure (up to 3.8 mm Hg), and continue to beat up to 10 months after implantation. 33 This same group also injected cardiomyocytes into the wall of the inferior vena cava 31 with similar outcomes.
A second group created EHT-like tissue, not within a vessel wall but by placing cells adjacent to the superficial caudal epigastric artery. 25,34 Their main goal was to show in vivo vascularization of thick EHT grafts. To achieve this goal, the authors used a polysurgery technique that involved sequential implantation of multiple cell sheets to create an EHT with an overall thickness of >1 mm. The grafts survived and continued to beat spontaneously and rhythmically for several months after implantation.
The above-cited studies did not create EHT cuffs around valve-containing segments of veins in the lower extremities nor did they use stem cell-derived cardiomyocytes. Yet they unequivocally showed that implanted immature cardiomyocytes can survive, form a vascularized syncytium, and generate contractile forces within or near vessel walls. These studies have showed that EHT constructs continue to beat rhythmically for extended periods of time—in the absence of both external stimulation and physical contact with the heart of a host animal.
Basic Designs of a Venous EHT Cuff
Two general types of venous EHT cuffs (VEHTCs) are envisioned (Figure 1). The first design can be implanted around vessels that have a partially competent valve, wherein the orifice of the valve has been distended. In this case, the cell content of VEHTC can be a simple mixture of pacemaker and ventricular cells. As the construct matures, these cardiac cells form gap junctions with each other to create an early form of a cardiac syncytium. As a result, the VEHTC sheath (or multiple VEHTC rings) contracts simultaneously, while the unidirectional valve within the vessel enables unidirectional flow. The intrinsic beating rate of these VEHTC can be altered by mixing different ratios of nodal (ie, pacemaker like) and ventricular cardiomyocytes. The second VEHTC design can be used around vessels without functional valves or with severely damaged valves. This type of VEHTC requires initial separation of pacemaker and ventricular-like cells, in order to create a VEHTC that will squeeze the vessel in a peristaltic fashion. This design can be achieved by creating an area with pacemaker cells upstream of the intended blood flow direction. A propagating wave of contraction will be generated as an electrical wave of activity spreads from the pacemaker cell region to the rest of the construct (Figure 2). By mixing different ratios of ventricular cardiomyocytes and fibroblasts into the VEHTC scaffold, one can modulate the propagation velocity and therefore VEHTC propulsion force.
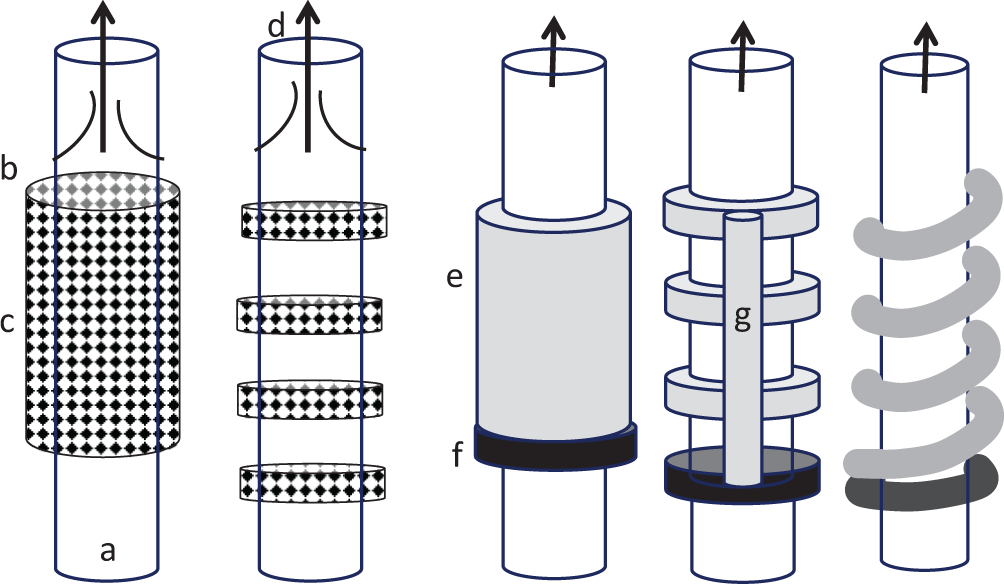
A cartoon illustrating different types of VEHTCs. (a) Blood vessel, (b) unidirectional valve, (c) VEHTC made of a mixture of pacemaker and contractile cells, (d) arrows indicate the direction of blood flow, (e) long VEHTC made of coupled contractile cells, (f) pacemaker cell-rich layer, and (g) layer of conductive tissue connecting individual VEHTC segments to create a peristaltic effect. EHT indicates engineered heart tissue; VEHTC, venous EHT cuff.
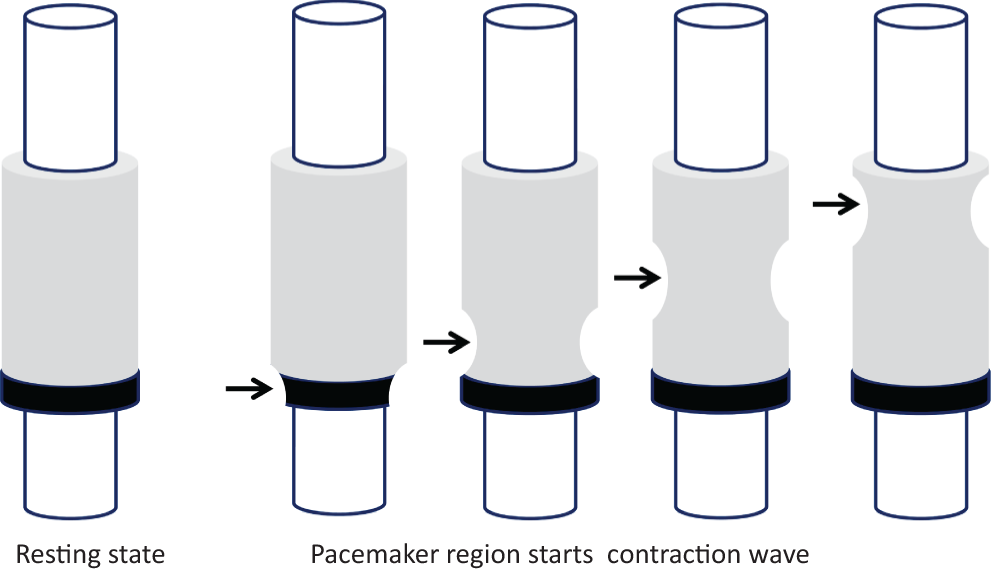
A cartoon illustrating a propagating wave of contraction in venous engineered heart tissue cuff (VEHTC) with a pacemaker ring. The velocity of the propagating wave can be modulated by cell seeding density or by mixing different ratios of cardiomyocytes and fibroblasts.
Potential methods to create VEHTCs are shown in Figure 3 and include surrounding the vessel with a 3D construct, wrapping a vessel in multiple sheets or thin threads of cardiomyocytes, or using a mesh of cardiac fibers (see also Supplemental Movie 1). These designs can be achieved by implanting custom-designed scaffolds and then injecting cardiomyocyte precursors or by culturing scaffolds together with cardiomyocytes and then implanting them.

Drawings of different types of possible venous engineered heart tissue (EHT) cuff (VEHTC) designs, including (A) thick tissue constructs, (B) vessels wrapped with cell sheets, and (C) mesh-like arrangement of cell fibers. See also Supplemental Movie 1.
Main Components of VEHTC
The 2 main components of VEHTCs are cells that can serve as cardiomyocyte precursors and scaffolds in which to seed the cells. Currently, the most obvious choice of cells to seed VEHTCs is patient’s own cells. Indeed, a number of sources have been shown to give rise to functional cardiomyocytes, including induced pluropotent stem cells, hematopoietic cells, adipose derived stromal cells, parthenogenetic stem cells, and others. 35 -37 Since this list continues to grow, the ultimate source of cardiomyocyte precursors to seed future VEHTC will depend on ethical, medical, and cost factors during the time of the actual procedure. Scaffolds into which cardiomyocyte precursors are seeded can be either biological or chemical in origin. Biological scaffolds include decellularized tissue slices, thrombin–fibrinogen-based glues, or sheets made of other bioderived extracellular matrix proteins. Chemical scaffolds include a rapidly growing variety of linkable polymers that can create highly controllable scaffolds with different degrees of architectural complexity. The list of materials and methods to produce scaffolds for tissue engineering purposes continues to increase. 38 -43
Culturing and Implanting of VEHTC
When cardiomyocyte precursors are combined with a scaffold of choice and then cultured using standard cell culture conditions—as either cell sheets, fiber networks, or small pieces of tissue, they form spontaneously contracting cardiac-like tissue. Furthermore, cell alignment and cardiomyocyte maturation improve significantly when EHT constructs are electrically and mechanically stimulated, which results in improved mechanical performance. 44 Therefore, additional ex vivo procedures, such as stretching and electrical stimulation, can be used to improve force development and quality of VEHTC before their implantation near the valve area (Figure 4 and Supplemental Movie 2). The VEHTC can also be cultured with a small piece of excised vein (Figure 5 and Supplemental Movie 3). In the latter case, the vein can act as a stretchable balloon upon connection to a pulsatile pressure source. The final step of the process is implantation of VEHTC around a vein of interest for which several scenarios can be envisioned. The acellular scaffold can be implanted first, followed by cell injection. Alternatively, cell-seeded scaffolds can be cultured ex vivo and then implanted around the vein of interest. The VEHTCs can also be created around segments of autologous excised vein, prosthetic, or decellularized allogeneic vessels. After creating VEHTC around it, the newly formed “self-pumping” vessel can be used to replace or bypass poorly functioning vein segment.

An excised segment of a rabbit posterior tibial vein containing a valve. The latter can be located by “milking” the vein, which empties the vein (A), followed by its refill (B). Bulging valvular sinus and valve cusps can then be clearly seen (C). See also Supplemental Movie 2.

Top row: excised dog saphenous veins (A), rings of collagen-based EHT in polydimethylsiloxane (PMDS) molds (B), and tubular fibrin-based EHT constructs (C). Bottom row: (D) beating VEHTC made from an excised segment of a rat posterior tibial vein. Right side: motion traces acquired from a region of interest shown by the gray rectangle. VEHTC contract spontaneously and can also be placed at desired frequencies. See also Supplemental Movie 3. EHT indicates engineered heart tissue; VEHTC, venous EHT cuff.
Advantages and Challenges of the Approach
The idea of using iPSC-derived cardiomyocyte tissue constructs as a tool to treat CDVI is novel and open to debate and experimentation. This approach applies recent discoveries in the cardiac regeneration field toward a very different clinical application. Remarkably, most of the concerns regarding the use of EHT for heart repair do not apply when the same constructs are used as VEHTC. Subsequently, we discuss these concerns and contrast them with the conventional goal of using EHTs for myocardial repair.
Contractile Force
One of the major hurdles of the cardiac tissue engineering field is the need to create a muscle that is strong and thick enough to create >200 mm Hg pressures within a large diameter container. This is not a trivial task, leading many to doubt whether bioengineered heart tissue is achievable any time soon. In contrast, VEHTCs do not need to be very powerful in order to work. First, pressures on the venous side are an order of magnitude lower than on the arterial side. Second, since the diameter of a medium-sized vein is much smaller than the ventricular cavity, the Law of LaPlace predicts that proportionally less wall tension is needed to create the same transmural pressure. Indeed, the mouse left ventricle with its 2 to 3 mm diameter and 1 to 1.5 mm wall thickness creates pressure exceeding 100 mm Hg. Contractile wall tension values that can be generated from recently developed cardiac tissue constructs are starting to reach physiological levels. For example, neonatal rat cardiomyocyte-based constructs have attained tensile force 29 as high as 30 mN/mm2 while hESC-derived cardiac tissue patches have recently been reported 24 to generate 11 mN/mm2. Notably, when first reported 21 in 2002 that number was of the order of 1 to 2 mN/mm2 so remarkable improvements in composition, fabrication, and conditioning of cardiac tissue constructs have occurred throughout the last decade. The average radius of a human saphenous vein 45 is about 2 mm; the LaPlace law suggests that the required thickness of a VEHTC to create 10 mN/mm2 (75 mm Hg) pressure will be about 10 mN/mm2 × 2 mm/30 mN/mm2 = 0.7 mm. This means that a VEHTC with a thickness of less than 1 mm can potentially make a difference in venous flow outcomes. As previously mentioned, the feasibility and long-term in vivo survival of multiple cardiomyocyte sheets with an overall thickness of up to 1 mm has already been shown. 34 Admittedly, the above-mentioned, back-of-the-envelope calculations do not take into account the internal stiffness of the vein, length of VEHTC, or the fact that blood vessels are open-ended structures. They are just a feasibility estimate and need experimental confirmation both in vitro and in vivo. Yet, these calculations support the general feasibility of the VEHTC approach.
Need for Vascularization
As described previously, VEHTCs do not need to be very thick. This eliminates the need to prevascularize EHTs before implantation, which is the second major obstacle in the cardiac engineering field. Being relatively thin and in close proximity to the main blood vessel, a VEHTC should survive initial grafting without major problems. As noted earlier, when multiple layers of cardiac myocytes are placed in the vicinity of a blood vessel, capillaries readily grow into the newly formed tissue. 25
Macroarchitecture
The third obstacle in the field of cardiac tissue engineering is how to recreate an anatomically and functionally complex heart on both macroscopic (multiple chambers, sinoatrial and atrioventricular nodes, valves, and nerves) and microscopic levels (orientation of myocytes, fibroblasts, capillaries, extracellular matrix, etc). These concerns are not applicable to VEHTCs, since they are designed to function as a primitive tube-like heart. As such, they can be created from a simple mixture of immature cardiomyocytes of any origin and full maturation of these cells is not required.
Arrhythmogenicity
Another major concern of the cardiac regeneration field is increasing the likelihood of cardiac arrhythmias. 46 The latter can be caused by endogenous ectopic activity of the grafts or mismatch in graft–host conduction velocities leading to reentry formation. Since VEHTC do not have any functional connection to the host heart, cardiac arrhythmias should not be a concern. One may also think of VEHTC causing unwanted twitches of the surrounding skeletal muscle. Yet, all previous attempts to electrically couple cardiac to adult skeletal muscle have proven unsuccessful, with only immature myotubes showing some degree of coupling under very defined conditions. 47 However, if problems of this nature arise, a layer of collagen or any other protective material can be placed around the VEHTC to prevent cardiomyocyte to skeletal muscle coupling.
Overgrowth
The VEHTC will be made from terminally differentiated cells; therefore, their ability to cause tumors should not be much different from other cells in the body. Stem cell-derived cardiomyocyte proliferation tapers off quickly, 48,49 which minimizes the concern that VEHTC will expand and impinge on the vessel lumen.
Thrombogenesis
Venous EHT cuffs will be positioned outside the vessel; therefore, the endothelial lining of the veins will not be impacted, minimizing any concerns of thrombus formation, fibroblast proliferation, and/or wound repair-related valve changes or closures.
Number of VEHTCs
Studies with valvular reconstruction or transplantation of excised autologous valves have shown that replacement of even a single valve can lead to significant improvements in the affected limb. 8,12,14,50 These studies suggest that a finite number of VEHTCs can make a difference in a patient’s outcome.
Possible additional advantages of the VEHTC approach include:
Stenting: In addition to its pumping mechanism, VEHTC should provide structural support to the distended vein, thus acting as an external stent that can help to bring valve cusps together. Today, both external (transcommissural) and internal valvuloplasty surgery are used to improve the competency of distended valves with mixed degree of success. 14,51,52 Another approach is external banding valvuloplasty that works by extraluminal wrapping of affected vein segments. 53 This method can be accomplished using a commercially available kit (Venocuff II, Imthage, Australia) and it has been shown to work fairly well in specific clinical cases. 8,54 Therefore, VEHTC can be designed to serve as both a stent and an actively contracting pump.
Self-adjustable pump:Venous EHT cuffswill be intrinsically myogenic, that is, upon more stretch, its contraction will be stronger according to the Frank-Starling mechanism. The latter is based on a stretch-dependent increase in myofilament calcium sensitivity and an increase in the number of cross-bridges. This mechanism has been shown to be fully operational in engineered cardiac tissue constructs. 55 As a result, VEHTC is expected to act as a self-adjustable pump. In a standing position, which increases hydrostatic pressure, VEHTC will be stretched leading to increased force of contraction. Once pressure is relieved and/or the patient lies down, the strength of the VEHTC pumping action will automatically decrease.
Pulsatile flow: Even if VEHTC will not be strong enough to fully combat hydrostatic pressure upon standing, its rhythmic contraction will lead to pressure pulsations within the vein. It is well established that pulsatile shear stress enhances secretion of cytokines by venous endothelial cells and, consequently, counteracts a predisposition to platelet aggregation, hypercoagulability, and white cell adhesion, diminishing thrombosis and promoting healing of leg ulcers. 56 -58 This was underlined in a clinical study 58 that compared the outcomes of pulsatile high-pressure venous insufficiency (due to severe tricuspid valve regurgitation) to chronic nonpulsatile venous insufficiency. Patients with pulsatile venous insufficiency had significantly increased flow in the distal calf veins, diminished leukocyte trapping, and a benign clinical course as compared to these with nonpulsatile disease.
Long-term effects on cardiovascular system: By placing cardiac cells outside the heart to assist venous return from lower extremities, one can prevent edema and ultimately aid flow throughout the entire circulatory system, including the heart muscle itself. Interestingly, placement of a left ventricular assist device (LVAD) that unloads the failing heart leads to a long-lasting improvement in systolic and diastolic function—even after the LVAD is disabled. 59 Therefore, one may imagine an intriguing long-term possibility of treating patients with failing hearts with their small, strategically placed EHT counterparts—not only around veins of lower extremities with impaired valves but also around other essential blood vessels.
Other vessels or cell types: In addition to treating CDVI, one can envision wrapping EHT constructs around lymphatic vessels to treat lymphedema. 60 -62 Alternatively, scaffolds around a vein can be seeded not with cardiac myocytes but with smooth muscle cells aided by interstitial cells of Cajal to provide rhythmic activation. Current tissue engineering protocols can create complex multilayered structures that include sheets of single-unit smooth muscle and the possibility of combining them with different cell types will only increase. 30,63 -65
Conclusions
Rapid advances in the fields of tissue engineering and stem cell biology open up the development of fascinating new treatment strategies for many patient groups. One of these strategies can be creating a rhythmically contracting layer of autologous cardiomyocytes around a vessel of interest to help increase venous or lymph flow, by essentially creating a heart outside the heart. These autologous mini EHT pumps will aid blood flow without the necessity of recreating the structural complexity of the adult heart.
The biological feasibility of this approach can also be demonstrated by lymph propulsion that uses a very similar physiological mechanism. Specifically, lymph propulsion is achieved by the spontaneous, rhythmic contractions of surrounding smooth muscle layer that serves as an essential pump mechanism to propel lymph uphill against a hydrostatic pressure gradient from peripheral lymphatics through lymph nodes into the thoracic duct. 66,67 The terms that are used to characterize the lymphatic pump are very similar to cardiac physiology and include stroke volume, preload, and afterload. One can see no fundamental contradictions to bioengineer a similar strategy using recent advances in stem cell biology as a means to aid return of venous flow. Another example are waves of wall muscle contraction that are responsible for transporting esophageal, ureteral, and gut contents.
With all the advantages of the outlined approach one wonders why nature itself did not equip us with a similar mechanism? The answer lies in the fact that venous insufficiency is a disease of old age; therefore, having venous pumps would not have imparted us with a significant evolutionary advantage. However, humans are living longer and the number of patients facing health problems due to limited venous flow will only increase. There is no reason why we cannot harness the advantages of using a patient’s own cardiomyocytes to perform a similar task—just outside their original anatomical location. Such mini pumps will resemble the embryonic tube heart observed during human development or the simplest primitive hearts seen in lower invertebrates. Notably, annelid worms have multiple (>7) tube-like hearts while sea squirts have tubular hearts that change direction of flow every 3 to 4 minutes by turning on and off an alternative pacemaker source. 3,68 Interestingly, some mammals, like bats, use venomotion for active venular pumping of the blood. 69 The novel approach presented here aims to use the insights from these biological mini pumps together with recent advantages in stem cell biology and tissue engineering to aid venous return in millions of patients having this debilitating disease.
Footnotes
Acknowledgments
The author thanks Drs Arthur Petrosian, Michael Laflamme, Ara Arutunyan, Anton Sidawy, Bao-Ngoc Nguyen, and Gordana Vunjak Novakovic for helpful discussions and Dr Nikki Gillum Posnack for editorial assistance. Technical help of Dr Luther Swift and Hao Ding is gratefully acknowledged.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: US Provisional Patent Application No. 61/905,491 on VEHTC concept was filed by the University on November 18, 2013.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported, in part, by the National Science Foundation (EAGER award CBET1231549) and intramural institutional funds.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.