
Abstract
Introduction
This study evaluated the efficacy and safety of a single-pill triple-combination of olmesartan/amlodipine/rosuvastatin (Olme/Amlo/Rosu) in comparison with a single-pill dual-combination of olmesartan/amlodipine (Olme/Amlo) in hypertensive patients with low-to-moderate cardiovascular risk.
Methods
This multicenter, active-control, randomized study included 106 hypertensive patients at low-to-moderate cardiovascular risk who were randomly assigned to receive either Olme/Amlo/Rosu 20/5/5 mg (Treatment 1), Olme/Amlo/Rosu 20/5/10 mg (Treatment 2), or Amlo/Olme 20/5 mg (Control) once daily for 8 weeks. The primary endpoint was the difference of the percent change in low-density lipoprotein cholesterol (LDL-C) level at 8 weeks from baseline in the 3 groups.
Results
The difference in the least square mean percent change (standard deviation) of LDL-C in the Treatment 1 and 2 groups compared with the Control group at 8 weeks was −32.6 (3.7) % and −45.9 (3.3) %, respectively (P < .001). The achievement rates of LDL-C level <100 mg/dL at 8 weeks were significantly different between the 3 groups (65.8%, 86.7%, and 6.3% for Treatment 1, 2, and Control groups, respectively, P < .001). The results of total cholesterol, triglycerides, high-density lipoprotein cholesterol, apolipoprotein B, and apolipoprotein B/apolipoprotein A1 were superior in the Treatment 1 and 2 groups compared with the Control group. Serious adverse drug reaction did not occur in the 3 groups. Medication adherence rates were excellent in the 3 groups (98.0% for Treatment 1 group, 99.7% for Treatment 2 group, and 96.3% for the Control group, P > .05).
Conclusion
Single-pill triple-combination of olmesartan/amlodipine/rosuvastatin was superior to the single-pill dual-combination of amlodipine/olmesartan in LDLC-lowering effects, with excellent safety profiles and adherence rates, in hypertensive patients at low-to-moderate cardiovascular risk.
Keywords
Introduction
Cardiovascular disease (CVD) has been the leading cause of death in the world over the past 15 years, according to World Health Organization data in 2016. 1 CVD is the second most common cause of death in Korea, with a mortality rate of 119.6 per 100,000 individuals. 2 Hypertension and dyslipidemia are the major risk factors for CVD. Recent hypertension guidelines recommend combination therapy of 2 antihypertensive drugs, with different action mechanisms, to maximize the blood pressure (BP) lowering effect and decrease adverse effects in patients with BP higher than 160/100 mmHg or more than 20/10 mmHg above the target BP.3–6 The guidelines also recommend to consider initial single-pill combination (SPC) therapy to improve medication adherence.
Hypertension and dyslipidemia often accompany one another, and management of dyslipidemia is effective to reduce the risk of CVD in hypertensive patients. According to the Dyslipidemia and Hypertension Fact Sheets in Korea, approximately 70% of hypertensive patients had dyslipidemia, although only 53.8% used anti-dyslipidemia treatment.7,8 Low-density lipoprotein cholesterol (LDL-C) lowering medications are not prescribed in approximately 20% of hypertensive patients who should take statins. According to the 2018 Korean dyslipidemia guidelines, the threshold level of LDL-C for statin use is ≥160 mg/dL in the low-risk group (with one or fewer major risk factors) and ≥130 mg/dL in the moderate-risk group (with 2 or more major risk factors). 9 The guidelines also state that individuals in the low-risk group with LDL-C of 130 to 159 mg/dL and individuals in the moderate-risk group with LDL-C of 100 to 129 mg/dL should consider statin therapy. Therefore, the management of LDL-C in patients in the vague range of LDL-C level (100-129 mg/dL in the moderate-risk group and 130-159 mg/dL in the low-risk group) may not be adequate.
In Korea, dual or triple SPC therapy is used for the treatment of hypertension. Recently, SPC drugs have also been introduced for treating hypertension and hypercholesterolemia. The present study was conducted to compare the efficacy and safety of a single-pill triple combination of olmesartan/amlodipine/rosuvastatin (Olme/Amlo/Rosu, OLOMAX®, Daewoong Pharmaceutical Co., Ltd, Korea) versus a single-pill dual combination of amlodipine/olmesartan (Amlo/Olme, SEVIKAR®, Daiichi-Sankyo, Japan) in hypertensive patients with low-to-moderate cardiovascular risk.
Material and Methods
Study Population
Individuals that met the following inclusion criteria were included in this study: (1) Men and women 19 years and older; (2) sitting systolic BP (sitSBP) ≥160 mmHg or sitting diastolic BP (sitDBP) ≥100 mmHg in antihypertensive-naive patients or sitSBP ≥140 mmHg or sitDBP ≥90 mmHg in patients administered angiotensin receptor blocker (ARB) or calcium channel blocker (CCB); and (3) LDL-C ≥130 mg/dL in the low-risk group or LDL-C ≥100 mg/dL in the moderate-risk group based on the risk category of the fourth Korean dyslipidemia guidelines (Table S1). 9
Exclusion criteria were as follows: (1) Secondary hypertension or suspected secondary hypertension; (2) symptomatic orthostatic hypotension; (3) concomitant diseases with atherosclerotic CVDs, any myopathy including rhabdomyolysis, biliary stenosis, or severe hepatic dysfunction within the previous 24 weeks; drug or alcohol abuse within the past 1 year; major psychiatric disorders; or malignant tumor within the previous 5 years; (4) laboratory abnormalities with creatine phosphokinase ≥2 times the upper normal limit, triglycerides (TGs) ≥500 mg/dL, active hepatic disorder including aspartate or alanine aminotransferase ≥3 times the upper normal limit, renal dysfunction with dialysis, creatinine clearance <30 ml/min, potassium >5.5 mEq/L, sodium <135 mEq/L, or uric acid >10 mg/dL; (5) a history of statin or nonstatin lipid-modifying drugs within 8 weeks prior to screening; (6) expected to take other antihypertensive and lipid-modifying drugs, cyclosporine, or other drugs that may affect blood lipids; (7) genetic conditions such as galactose intolerance, Lapp lactase deficiency, or glucose–galactose malabsorption; and (8) pregnant or breastfeeding women, women of childbearing potential, and men who were unwilling to use appropriate contraception.
The trial protocol was approved by the institutional review board at each participating center (IRB No: B-1907/550-004 in the Seoul National University Bundang Hospital and IRB No: KBSMC 2019-06-015 in the Kangbuk Samsung Hospital), and informed consent was obtained from all subjects.
Study Design
This multicenter, randomized, open-label, active-control, phase IV clinical trial (OPTIMIST trial) was performed at 15 institutions in Korea from August 2019 to July 2021. Eligible participants at the screening visit (visit 1) provided informed content and were given Amlo/Olme 5/20 mg with recommended therapeutic lifestyle changes (TLC) during a 6-week run-in period. The following criteria at the randomization visit (visit 2) were required to be met for participation in the study: (1) Drug compliance of 70% or more of Amlo/Olme 5/20 mg during the screening period and good TLC performance and (2) measured LDL-C (mLDL-C) ≥130 mg/dL for the low-risk group or mLDL-C ≥100 mg/dL for the moderate-risk group. Participants were randomly assigned to 3 groups, Treatment 1 (olmesartan/amlodipine/rosuvastatin 20/5/5 mg, Olme/Amlo/Rosu 20/5/5), Treatment 2 (olmesartan/amlodipine/rosuvastatin 20/5/10 mg, Olme/Amlo/Rosu 20/5/10), and Control (amlodipine/olmesartan 5/20 mg, Amlo/Olme 5/20) groups, with 1:1:1 ratio by a block randomization method for each participating center using the SAS system (Version 9.4 64 bit, SAS Institute Inc., Cary, NC, USA) (Figure 1). Among 158 subjects screened, 52 were excluded because of screening failure; the remaining 106 were randomized to Treatment 1 (n = 40), Treatment 2 (n = 32), or Control (n = 34) groups. Three subjects dropped out, and 103 subjects completed the study (Figure 2).
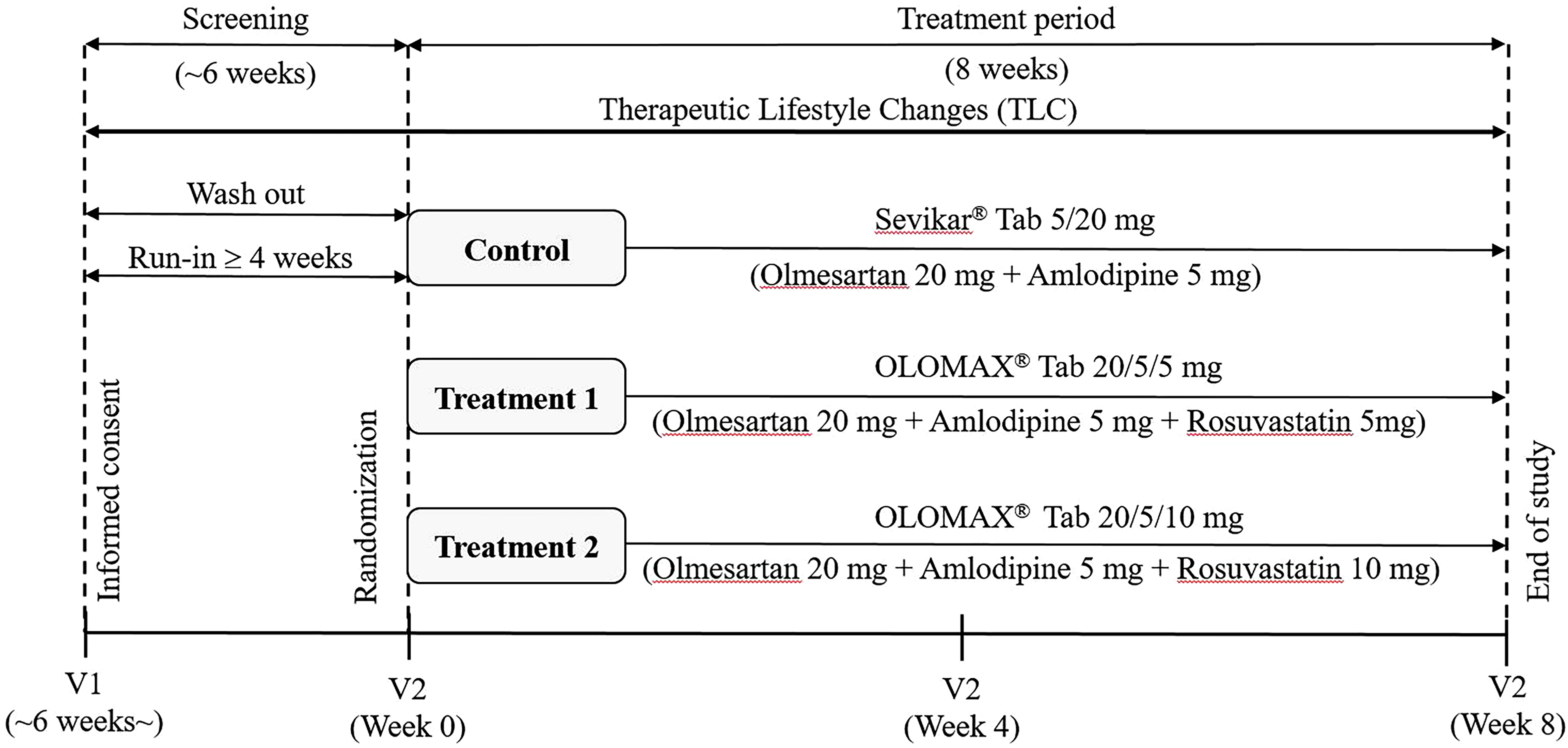
Schematic diagram of the study design.

Flow chart of patient selection. Amlo/Olme, amlodipine/olmesartan; Olme/Amlo/Rosu, olmesartan/amlodipine/rosuvastatin.
BP was measured 3 times at least 2 min apart in a sitting position using the same sphygmomanometer in each center. The average of the 3 measurements was calculated as the sitBP. Biochemical measurements including lipid profile were performed after 12 h of fasting in each participating center that was certified by the Korean Society of Laboratory Medicine.
Efficacy and Safety Assessment
The primary efficacy endpoint was the mean percentage change of mLDL-C at 8 weeks after treatment compared with baseline between Treatment 1 and Control groups and between Treatment 2 and Control groups. The secondary efficacy endpoints were (1) the mean percentage changes of measured LDL-C at 4 weeks after treatment; total cholesterol (TC), TG, high-density lipoprotein cholesterol (HDL-C), mLDL-C/HDL-C, high-sensitivity C reactive protein (hsCRP), apolipoprotein A1 (apoA1), apolipoprotein B (apoB), apoB/apoA1 at 4 weeks and 8 weeks of treatment; sitSBP and sitDBP at 4 weeks and 8 weeks after treatment; fasting plasma glucose, fructosamine, and hemoglobinA1C at 4 weeks and 8 weeks after treatment; (2) percentage of subjects with mLDL-C less than 70 mg/dL and 100 mg/dL at 4 weeks and 8 weeks of treatment; and (3) percentage of subjects with sitSBP <140 mmHg and sitDBP <90 mmHg compared with baseline between Treatment 1 and Control groups and between Treatment 2 and Control groups. The safety endpoints were (1) adverse events, (2) laboratory tests, (3) rate of serum aspartate or alanine aminotransferase concentration ≥3 times of the upper limit of normal, and (4) rate of creatine kinase ≥10 times the upper limit of normal. Adverse events included treatment-emergent adverse event (TEAE), adverse drug reaction (ADR), serious adverse event (SAE), and serious adverse drug reaction (SADR). Adherence to medication was assessed using medication dispensing records and pill counts.
Statistical Analysis
Data are presented as mean (standard deviation, SD) and median [minimum, maximum] for continuous variables and frequency (percentage) for categorical variables. The comparison of the mean percentage changes of LDL-C and other continuous variables to assess primary and secondary endpoints was analyzed by analysis of covariance (ANCOVA) using PROC MIXED procedure in SAS. The comparison for the change of categorical variables was evaluated with Pearson's chi-square test or Fisher's exact test. Pre-specified subgroup analysis was performed according to cardiovascular risk (low and moderate).
To calculate sample size, the average LDLC change rate was assumed to be 18% for the Treatment groups, 0% for the Control group, and 21.87% for the standard deviation. Based on the above setting basis, the allocation ratio between the administration groups was set at 1:1 and the significance level of both sides was 5%. The minimum number of study subjects to secure 80% statistical power was 25 per group. Considering a dropout rate of 15%, 30 patients per group were calculated. Therefore, a total of 90 study subjects was recruited from the 3 groups.
The efficacy analysis was conducted with a full-analysis set (FAS) as the main analysis and a per-protocol set (PPS) as the sensitivity analysis. The safety analysis used a safety set (SS). The FAS included subjects who were administered clinical trial drugs at least once and who underwent mLDL-C measurement as the primary efficacy variable at least once after randomization. The PPS refers to subjects who completed the study without violating the critical study protocol, and the SS included all subjects who received the study drugs at least once. Pre-specified subgroup analyses were performed according to risk category. Two-tailed p value < 0.05 was considered statistically significant and was calculated using SAS software version 9.3 (SAS Institute, Cary, NC, USA).
Results
In the overall population, subjects under the age of 65 accounted for 72.6% of the total group, and the mean age was 59.5 (10.7) years; the proportion of male subjects was approximately two-thirds. The proportion of individuals who had been diagnosed with hypertension was 91.5%; among them, 83.0% were taking ARB or CCB at the time of participation in the study. The proportion of total subjects represented by the moderate-risk group was higher than that of the low-risk group (84.9% vs 15.1%). Baseline LDL-C, HDL-C, TG, and TC levels were 147.3 (25.4) mg/dL, 51.0 (12.3) mg/dL, 167.0 (85.4) mg/dL, and 219.5 (32.3) mg/dL, respectively, and baseline apoB and apoA1 were 123.1 (21.4) mg/dL and 140.5 (23.1) mg/dL, respectively. Baseline sitSBP and sitDBP were 131.3 (14.2) mmHg and 82.4 (10.4) mmHg, respectively. Baseline LDL-C level in the low- and moderate-risk groups was 157.9 (17.8) mg/dL and 145.2 (26.3) mg/dL, respectively.
The baseline characteristics were similar among the 3 groups (Table 1).
Baseline Characteristics of the 3 Groups Enrolled in This Study.

Low-risk group was defined as individuals with no major risk factor; intermediate-risk group was defined as individuals with one or more major risk factors. High HDL-cholesterol (≥60 mg/dL) is considered a protective factor, so one risk factor is deducted. Abbreviations: Amlo/Olme, amlodipine/olmesartan; ASCVD, atherosclerotic cardiovascular disease; HDL, high-density lipoprotein; NA, not applicable; Olme/Amlo/Rosu, olmesartan/amlodipine/rosuvastatin.
Primary Efficacy Endpoint
The mean (SD) change in LDL-C from baseline at 8 weeks was −3.3 (14.8) mg/dL, −34.1 (17.4) mg/dL, and −48.4 (10.6) mg/dL in the Amlo/Olme 5/20, Olme/Amlo/Rosu 20/5/5, and Olme/Amlo/Rosu 20/5/10 groups, respectively. The differences in the least squares mean (LSM) (standard error, SE) of LDL-C change at 8 weeks in the Olme/Amlo/Rosu 20/5/5 and Olme/Amlo/Rosu 20/5/10 groups compared with the Amlo/Olme 5/20 group were −32.6 (3.7)% and −45.9 (3.3)%, respectively (p < 0.001) (Table 2 and Figure 3).

Percent changes in LDL-C at week 8 in the 3 groups in the full-analysis set. (A) Amlo/Olme 5/20 mg versus Olme/Amlo/Rosu 20/5/5 mg, (B) Amlo/Olme 5/20 mg versus Olme/Amlo/Rosu 20/5/10 mg. Data are expressed as mean (standard error). Abbreviations: Amlo/Olme, amlodipine/olmesartan; Olme/Amlo/Rosu, olmesartan/amlodipine/rosuvastatin; LDL-C, low-density lipoprotein cholesterol; SE, standard error.
Changes in LDL-C at 4- and 8-Week Follow-up in the 3 Groups in the Full-Analysis set.
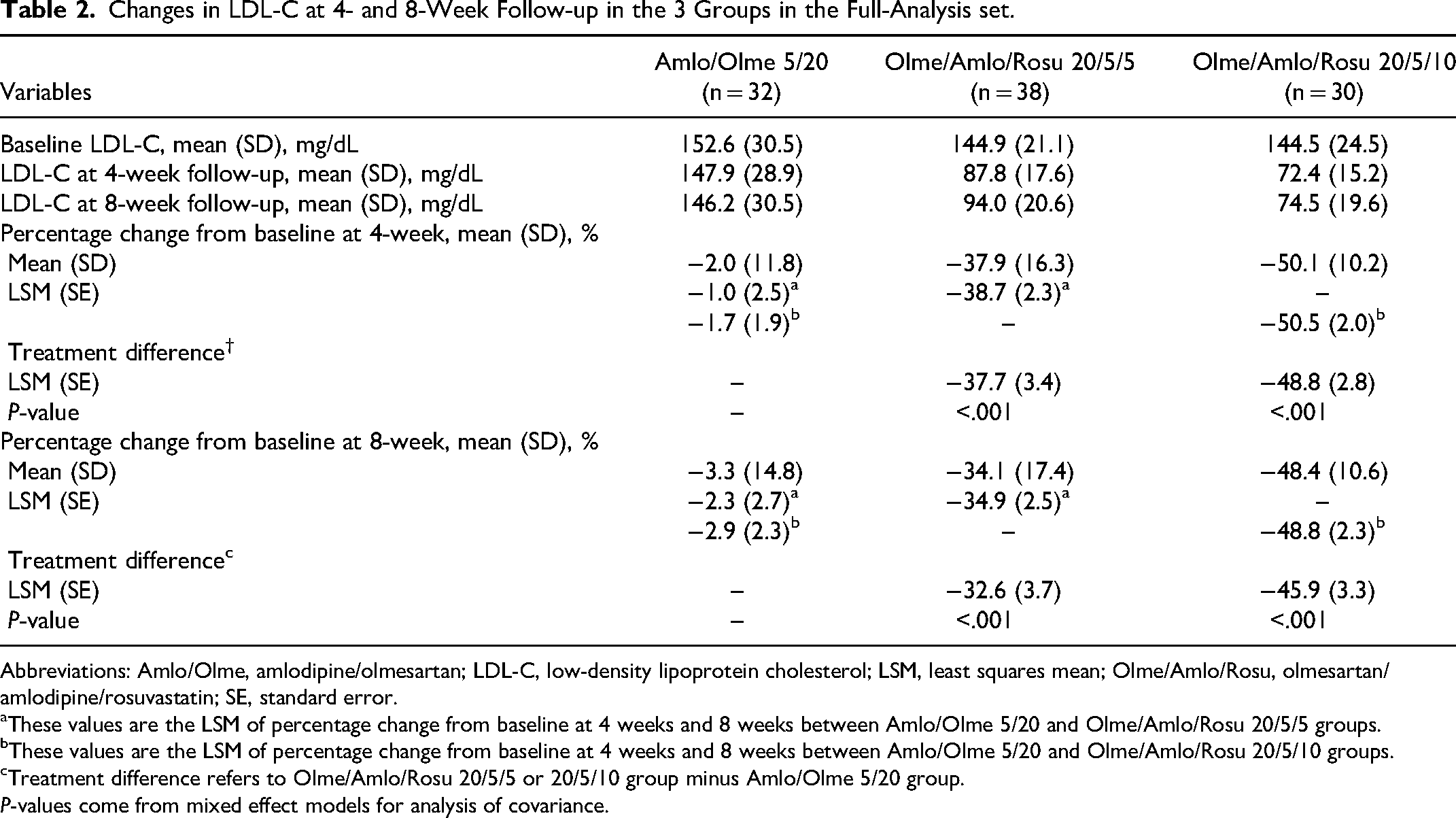
Abbreviations: Amlo/Olme, amlodipine/olmesartan; LDL-C, low-density lipoprotein cholesterol; LSM, least squares mean; Olme/Amlo/Rosu, olmesartan/amlodipine/rosuvastatin; SE, standard error.
These values are the LSM of percentage change from baseline at 4 weeks and 8 weeks between Amlo/Olme 5/20 and Olme/Amlo/Rosu 20/5/5 groups.
These values are the LSM of percentage change from baseline at 4 weeks and 8 weeks between Amlo/Olme 5/20 and Olme/Amlo/Rosu 20/5/10 groups.
Treatment difference refers to Olme/Amlo/Rosu 20/5/5 or 20/5/10 group minus Amlo/Olme 5/20 group.
P-values come from mixed effect models for analysis of covariance.
Other Efficacy Endpoints
The achievement rates of LDL-C < 100 mg/dL at 8 weeks were 6.3%, 65.8%, and 86.7% in the Amlo/Olme 5/20, Olme/Amlo/Rosu 20/5/5, and Olme/Amlo/Rosu 20/5/10 groups (p < 0.001) and those of LDL-C < 130 mg/dL at 8 weeks were 28.2%, 92.1%, and 100% in the 3 groups, respectively (p < 0.001) (Table S2 and Figure S1). The achievement rates of the LDL-C target goal (LDL-C < 130 mg/dL) in the moderate risk subgroups according to fourth Korean dyslipidemia guidelines were 27.6%, 90.9%, and 100% in the 3 groups (p < 0.001), and the percentage of subjects that achieved the LDL-C target goal (LDL-C < 160 mg/dL) in the low risk subgroup was 100% in both the Olme/Amlo/Rosu 20/5/5 and Olme/Amlo/Rosu 20/5/10 groups (Table S3 and Figure S2).
There were significant treatment differences in LSM (SE) change in TC, TGs, HDL-C, apoB, and apoA1 between the Amlo/Olme 5/20 and Olme/Amlo/Rosu 20/5/5 groups and between the Amlo/Olme 5/20 and Olme/Amlo/Rosu 20/5/10 groups (Table S4). The treatment differences in LSM (SE) change of apoB were −32.0 (4.1) %and −43.5 (4.4) % between the 2 groups, respectively. There were no significant differences in hsCRP, fasting glucose, hemoglobinA1C, and fructosamine levels among the 3 groups (Table S5).
The treatment differences in the mean change of sitSBP and sitDBP from baseline at 8 weeks in the 3 groups were not significant, and the achievement rates of the sitBP target goal at 8 weeks, defined as SBP <140 and DBP <90 mmHg, between the 3 groups were not significantly different (65.6%, 71.1%, and 66.7% in the Amlo/Olme 5/20, Olme/Amlo/Rosu 20/5/5, and Olme/Amlo/Rosu 20/5/10 groups, respectively, Table S6 and Figure S3).
Safety Endpoints
The frequency of TEAEs in the overall population was 10.4%; no significant difference was observed among the 3 groups. Only 1 ADR case was reported (constipation) in Olme/Amlo/Rosu 20/5/5 group; no cases of serious ADR were reported (Table 3). Medication adherence rates in the FAS were excellent in the 3 groups (98.0% and 99.7% in the Olme/Amlo/Rosu 20/5/5 and Olme/Amlo/Rosu 20/5/10 groups, respectively, and 96.3% in the Amlo/Olme 5/20 group, p > 0.05); the rates in the PPS were similar (Table S7 and Figure S4).
Summary of Treatment-Related Adverse Effects Including Laboratory Tests in the Safety set.

Abbreviations: ADR, adverse drug reaction; Amlo/Olme, amlodipine/olmesartan; Olme/Amlo/Rosu, olmesartan/amlodipine/rosuvastatin; SADR, serious adverse drug reaction; SAE, serious adverse event; TEAE, treatment-emergent adverse event; ULN, upper limit of normal.
Seven TEAEs occurred in 5 patients, which were hematuria (n = 1), deafness (n = 1), food poisoning (n = 1), upper limb fracture (n = 1), headache (n = 1), anxiety (n = 1), and removal of foreign body from throat (n = 1). All cases were mild and had an “unlikely” relationship with the drug.
Four TEAEs occurred in 3 patients, which were positional vertigo (n = 1), constipation (n = 1), urticaria (n = 1), and neck pain (n = 1). The first 3 cases were mild and neck pain was moderate.
Five TEAEs occurred in 3 patients, which were increased blood urea nitrogen (n = 1) and creatinine (n = 1), decreased creatinine clearance (n = 1), food fracture (n = 1), and dizziness (n = 1). All cases had an “unlikely” relationship with the drug.
One patient reported mild constipation. This ADR was classified as a “possible” relationship with the drug.
One patient reported neck pain.
Discussion
This study have shown that triple SPC therapy with statins can be a feasible treatment option to easily control LDL-C levels without additional adverse effects in hypertensive patients at low-to-moderate cardiovascular risk, who are susceptible to oversight of statin therapy.
ARB and CCB are widely used as first-line drugs for BP lowering in hypertensive patients, and the combination of the 2 drugs can be expected to improve cardiovascular outcomes. 10 Recent guidelines recommend initial SPC therapy to reduce adverse effects and improve drug compliance in hypertensive patients with stage 2 or those requiring lowering of SBP/DBP to 20/10 mmHg or more.3–6 The single pill of olmesartan and amlodipine was commercialized in Korea in 2008 and is one of the most used antihypertensive combination drugs. Previous studies showed that the single-pill fixed-dose combination therapy of olmesartan and amlodipine was more effective in lowering BP and achieving BP target goal than either drug alone.11,12
A recent Mendelian randomization study reported that genetic exposure to both lower LDL-C and BP levels is associated with reducing cardiovascular events. 13 Co-management of dyslipidemia with hypertension is fundamental to the prevention of CVD. In Korea, the prevalence of dyslipidemia in hypertensive patients is approximately 70%, but approximately 2 to 10 hypertensive patients do not receive statin medication.8,9 One of the reasons for this discrepancy between the guidelines and clinical practice is as follows. The Korean dyslipidemia treatment guidelines classify high- and very high-risk groups according to disease entity and the low-to-moderate risk group according to the number of major cardiovascular risk factors (Table S1). Therefore, in clinical practice, doctors may be prone to forgetting LDL-C-lowering therapy in the low-to-moderate risk group due to the complexity of application of risk category.
The Korean dyslipidemia guidelines recommend the use of statins when LDL-C level is ≥160 mg/dL in the low-risk group and ≥130 mg/dL in the moderate-risk group, and the respective LDL-C treatment target of <160 and <130 mg/dL. 9 Moreover, the guidelines indicate that treatment for the low-risk group with 130 to 159 mg/dL LDL-C and the moderate-risk group with 100 to 129 mg/dL LDL-C might involve statins, of which the level is a range that may not be active in statin use in clinical practice. Very recently, a nationwide cohort study from the Korean National Health Insurance Service database was performed to validate the treatment target of LDL-C according to the risk category in the guidelines. The study reported an increased risk of CVD including myocardial infarction and stroke from ≥ 130 mg/dL of LDL-C level in the low-CV risk group and an increased risk of myocardial infarction from ≥ 100 mg/dL of LDL-C level in the moderate-risk group. 14 These findings provide a rationale for the inclusion criteria of the potential effect of statin treatment in the low-risk group with ≥ 130 mg/dL LDL-C level and the moderate-risk group with ≥ 100 mg/dL LDL-C level in our study.
Rosuvastatin, which was used in this study, is one of the most used LDL-C lowering drugs in Korea and worldwide, and its use is supported by strong scientific evidence, especially for primary prevention of CVD, through previous large-scale randomized control trials.15–17 In particular, the HOPE-3 trial that included patients at intermediate risk with 128 mg/dL LDL-C level showed that rosuvastatin at 10 mg per day significantly reduced the risk of cardiovascular events and lowered LDL-C by 39.6 mg/dL compared with placebo. The effects of LDL-C reduction of the 2 groups of Olme/Amlo/Rosu in our study were consistent with that of the HOPE-3 trial, 32.6 mg/dL and 45.9 mg/dL in the Olme/Amlo/Rosu 20/5/5 and 20/5/10 groups, respectively, compared with the Amlo/Olme group. The achievement rate of the LDL-C target goal mentioned in the Korean dyslipidemia guidelines was excellent in the 2 Olme/Amlo/Rosu groups, at greater than 90%. In the subgroup analysis of the highest third of SBP (>143.5 mmHg) of the HOPE-3 trial, the group that used both antihypertensive drug and statin (HR[95% CI], 0.60[0.43-0.84]) showed a reduced risk of future cardiovascular events more than the group only with antihypertensive drug (0.76[0.60, 0.96]) compared with the placebo group.16,17 These results suggest that co-management for BP and LDL-C reduction in hypertensive patients at intermediate risk, even if LDL-C level is not very high, may provide additional benefits to future cardiovascular event risk reduction.
The intriguing finding of our study is that even a 5 mg dose of rosuvastatin showed a significant reduction in LDL-C levels and achieved the target goal in almost all patients in our study population. Previous literature has reported that statin dose escalation may increase the risk of adverse events, particularly the risk of new-onset diabetes.18,19 Taking these considerations into account, our results suggest that rosuvastatin 5 mg, when used as an initial LDL-C lowering therapy in hypertensive patients at low-to-moderate risk, is effective enough to achieve LDL-C target goal attainment rates compared to rosuvastatin 10 mg, without additional adverse effects.
The importance of medication adherence has been highlighted for optimal management, especially for patients with chronic disorders including hypertension and dyslipidemia. SPC therapy is helpful in improving medication adherence and may lead to better clinical outcomes.20,21 The size and shape of the drug may also affect medication adherence. 22 The single-pill triple combination formulation of Olme/Amlo/Rosu, used in this study, is a round, flat tablet with a diameter of 7.5 to 8 mm, which is one of the smallest among single-pill formulations of 2 antihypertensive drugs and one statin in Korea; this medication has the advantage of being convenient to take. As a result, medication adherence rates in our study were quite excellent, at greater than 98%.
This study has several limitations. First, the present study included a relatively small population and a short follow-up period. Second, the recruitment rate in the study was low, mainly due to strict government quarantine regulations and other safety protocols with the outbreak of coronavirus disease 2019 (COVID-19) shortly after the start of the study. Third, our study design was not significantly different from previous studies, as previous studies have shown that the addition of statins to antihypertensive drugs has an unquestionable LDL-C-lowering effect. However, the results of our study may provide additional evidence of the potential benefit of single-pill triple combination therapy in hypertensive patients at low-to-moderate risk, who tend to be overlooked for statin therapy and have been under-represented in clinical trials.
Conclusions
The single-pill triple-combination of olmesartan/amlodipine/rosuvastatin was superior to the single-pill dual-combination of olmesartan/amlodipine in LDL-C lowering effects, with similar BP reduction effects and excellent safety profile and adherence rates in hypertensive patients at low to moderate cardiovascular risk. This finding suggests that guideline-based treatment with triple combination therapy can be easily performed without additional adverse effects in 20% of hypertensive patients who need to receive statin based on guidelines but are not receiving statin.
Supplemental Material
sj-docx-1-cpt-10.1177_10742484231205204 - Supplemental material for Efficacy and Safety of a Single-Pill Triple Combination of Olmesartan, Amlodipine, and Rosuvastatin in Hypertensive Patients with Low-to-Moderate Cardiovascular Risk: A Multicenter, Randomized, Open-Label, Active-Control, Phase IV Clinical Trial
Supplemental material, sj-docx-1-cpt-10.1177_10742484231205204 for Efficacy and Safety of a Single-Pill Triple Combination of Olmesartan, Amlodipine, and Rosuvastatin in Hypertensive Patients with Low-to-Moderate Cardiovascular Risk: A Multicenter, Randomized, Open-Label, Active-Control, Phase IV Clinical Trial by Byung Jin Kim, Kwang Soo Cha, Wook Hyun Cho, Eung Ju Kim, Seung-Hyuk Choi, Moo Hyun Kim, Sang-Hyun Kim, Jun-Bean Park, Seong-Mi Park, Il Suk Sohn, Kyu Hyung Ryu and In-Ho Chae in Journal of Cardiovascular Pharmacology and Therapeutics
Footnotes
Data Availability
The data analyzed for the present study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The trial protocol was approved by the institutional review board at each participating center (IRB No: B-1907/550-004 in the Seoul National University Bundang Hospital and IRB No: KBSMC 2019-06-015 in the Kangbuk Samsung Hospital), and informed consent was obtained from all subjects. The study was performed under the standards specified in the International Council for Harmonization Guidelines for Good Clinical Practice and the principles of the Declaration of Helsinki. This trial was registered at ClinicalTrials.gov on October 08, 2019, with ClinicalTrials.gov Identifier: NCT04120753.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; participated in drafting, revising, or critically reviewing the article; gave final approval of the version for publication; have agreed on the journal to which the article has been submitted; and agree to take responsibility and be accountable for the contents of the work.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.