
Abstract
Background:
Atrial fibrillation (AF) is the most common arrhythmia to appear in clinical practice. People with AF have 5 times the risk of stroke compared to the general population.
Objective:
This study aimed to determine the prevalence of AF in people over the age of 50 without known AF, who presented to a community pharmacy to check their cardiovascular risk factors, to identify risk factors associated with AF, and to assess the risk of stroke in people who screened positive for AF.
Methods:
A multicenter observational descriptive study of a screening program took place from May to December 2016. A blood pressure monitor (Microlife Watch BP Home) was used to screen for AF, and the CHA2DS2-VASc questionnaire was used to assess stroke risk.
Results:
The study included 452 adults over the age of 50. The CRIFAFARMA study detected a prevalence of AF of 9.1%. Risk factors for AF were: age of 75 years or older (P = .024), lack of physical activity (P = .043), diabetes (P < .001), dyslipidemia (P = .003), and history of cardiovascular disease (P = .003). Diabetes (OR 2.79, P = .005) and dyslipidemia (OR 2.16, P = .031) had a combined explanatory capacity in the multivariable logistic regression model adjusted for age. 85% were at high risk of stroke according to the CHA2DS2-VASc scale.
Conclusions:
AF was detected in more than 9% of the included population. Factors associated with AF were advanced age, lack of physical activity, diabetes, dyslipidemia, and history of cardiovascular disease, with diabetes and dyslipidemia standing out as the factors with independent explanatory capacity.
Introduction
Atrial fibrillation (AF) is the most frequent type of arrhythmia and one of the most prevalent cardiovascular diseases in the world, affecting 1% to 2% of the population. 1 In Spain, reported prevalence oscillates from 1.5% to 5.5%, depending on the type of study. 2 -7 The number of patients with AF is expected to rise in the coming years 8 as detection improves and the prevalence of predisposing conditions and risk factors increases. The most frequent embolic event arising from AF is stroke, which is associated with disability, dependence, and an increase in health care use and costs. 8 AF is often asymptomatic, especially in early stages, and usually evades detection until people present symptoms, cardiovascular risk factors, or sequelae like heart failure and/or stroke. 9,10 The latter is highly amenable to prevention through the use of appropriate thromboprophylaxis. 11
Esato et al 12 stated that all-cause mortality was higher in asymptomatic patients than symptomatic patients with paroxysmal AF. Early detection has been proposed as the optimal approach for increasing diagnostic rates and the use of anticoagulant therapy in people with AF, thus reducing the incidence of ischemic stroke. 1,13 Screening strategies for this disease aim primarily to identify people with AF who do not present signs or symptoms of arrhythmia, and the process is carried out in 2 stages. First, asymptomatic people with an irregular pulse are identified, and second, they undergo a 12-lead electrocardiogram (ECG) to confirm or rule out AF. 14 There is still controversy with regard to the choice of screening method, with great importance placed on the precision in the detection of an irregular pulse caused by AF. In recent years, different authors have proposed using modified blood pressure monitors (BPM) to improve the screening process. 15 -18 In 2013, the National Institute for Health and Care Excellence (NICE) 19 guidelines on the use of medical technology affirmed that using these devices could be beneficial for detecting AF in the primary health care setting, recommending the Microlife Watch BP Home device to detect AF during routine monitoring of blood pressure in primary care.
The Microlife Watch BP Home 19 is an electronic BPM that includes an algorithm to detect an irregular pulse. The algorithm calculates an irregularity index based on the interval between beats and indicates an irregular pulse when a threshold is crossed. 18 Given its high sensitivity and specificity, this device compares favorably with routine practices for manually measuring the pulse, 20 so introducing its use in clinical practice could provide a simple, objective method for monitoring and controlling blood pressure and new opportunities to detect AF. Indeed, in United Kingdom, this device is already used as a standard BP monitor (with potential for AF detection) in primary care. 15
Community pharmacies are increasingly delivering interventions for the primary and secondary prevention of heart diseases, and one aim of these services is to facilitate the early diagnosis of some pathologies, including those related to cardiovascular health. 21 Several studies 22 -24 have already demonstrated that screening services in community pharmacies are feasible and cost-effective, although more research is needed to explore the viability of combined cardiovascular screening. 25 This study aimed to determine the prevalence of AF in people over the age of 50 who presented to a community pharmacy to check and/or control their cardiovascular risk factors, to identify risk factors associated with AF, and to assess the risk of stroke in people who screened positive for AF.
Methods and Material
Study Design and Participants
CRIFAFARMA is a multicenter, observational descriptive study of a screening program for AF in community pharmacies, performed from 2016 to 2017 in 19 community pharmacies in Alicante (Spain). Participating pharmacies offered routine services for monitoring and/or controlling cardiovascular risk factors (hypertension, diabetes mellitus, dyslipidemia) and took part in the study as part of their regular practice. Participation was free, voluntary, and independent. The study complied with the principles of the Declaration of Helsinki and was approved by the institutional ethics committee of Miguel Hernandez University of Elche, 11 DE FEBRERO 2016: DCM.CCM.01.16.
This paper follows the STROBE reporting guidelines for observational studies.
Participants were people who used the pharmacy service to check and/or monitor any cardiovascular risk factor from 1 May to 31 December 2016 and who were not referred to the medication dispensing service. Inclusion criteria were: age of 50 years or older and signed informed consent. Exclusion criteria were: incapacitating and/or terminal illness, and history of using a pacemaker or defibrillator.
To calculate the sample size, we estimated a prevalence of AF of 5% in the population with some cardiovascular risk factor, 7,8,11 a confidence level of 95% (Z2α = 0.05), and a precision of 2%. A sample size of 456 patients was obtained; after factoring in a loss of 10% of the sample, the total number of participants needed was 500. We used a consecutive, non-probability sampling strategy.
AF Screening Procedure
A standardized screening procedure was designed, specifying the responsibilities of collaborating pharmacists, necessary materials, and a protocol for performing the study. The pharmacists took part in a clinical training session prior to beginning the study. Pharmacists participating in the study shared a face-to-face clinical session taught by an expert for AF training, where training and information about the importance of early detection of AF and the available treatment options was provided. A workshop was held to train participating pharmacists on how to correctly measure blood pressure, explain how the monitor detects AF, and how it should be interpreted. The standard work procedure and data collection procedure were explained and doubts were resolved. Throughout the study period, contact was maintained with the participating pharmacists in order to verify and maintain homogeneity in the data collection criteria. Fidelity to the study protocol and data collection criteria were monitored throughout the study period.
Collaborating pharmacists recruited participants who met selection criteria and went to their community pharmacy to check for or monitor some cardiovascular risk factor. AF screening was performed by means of the Microlife WatchBP Home device. 19 This electronic sphygmomanometer measures blood pressure in compliance with the guidelines of the European Society of Hypertension, the American Heart Association, and the British Hypertension Society, and it includes an algorithm to detect irregularities in the pulse. To use the device, a cuff is placed on the person’s right or left arm, and it inflates and deflates automatically after being turned on. The screen shows the mean values of 3 blood pressure measurements. If irregularities in the pulse were detected on at least 2 measurements, an icon with the description “Afib” appears and starts to blink. If the BPM showed the Afib icon on the first reading, the measurement was repeated after at least 1 hour had passed. If the Afib icon appeared on the second use, the result was considered positive for AF; otherwise, the result was considered negative, as specified in the manufacturer’s instructions.
Once the screening test was completed, the pharmacist explained the result to the participant and provided a written report detailing the blood pressure measurement and the results of the AF screening test. The time needed to screen each person was about 20 min; both the measurements and the clinical interviews took place in the personal service areas of participating pharmacies, thus guaranteeing people’s confidentiality during the performance of the study.
All participants with a positive result for AF were referred to their primary health care physician with the pharmacy report in order to assess the need for a 12-lead ECG to precisely determine the abnormality in the cardiac rhythm, as laid out in the NICE 26 and European Society of Cardiology 8 guidelines (Figure 1). The prevalence of AF was not confirmed by 12-lead ECG.

Standard operating procedure.
Study Variables
The following information was collected from participants: age; sex; nationality; country of origin; location of residence; employment status (employed/unemployed or student/ retired); educational attainment (from no schooling to primary school/from secondary schooling to university); height; weight; waist circumference; routine physical activity (yes/no, and if yes, moderate/intense); alcohol intake (yes/no); tobacco use (never smoker/current smoker/ex-smoker); comorbidities such as hypertension, diabetes, and dyslipidemia (yes/no, and if yes, years of evolution); and personal and family history of cardiovascular disease (yes/no).
The primary outcome was AF (yes/no), measured by pharmacists during the screening test. The CHA2DS2VASc comorbidity questionnaire was also completed in people with positive screening tests in order to assess the risk of stroke in people with AF. 27
Statistical Analysis
A descriptive analysis was performed for all variables, calculating absolute and relative frequencies for categorical variables and, medians and interquartile ranges (IQR) and ranges for quantitative variables. These descriptive statistics were used to express the prevalence of AF and the 95% confidence intervals (CIs) using bootstrapping methods. The prevalence of early detection AF was compared according to explanatory variables, using 2×2 tables and the chi-square test for categorical variables, and the Mann-Whitney U test to compare mean values of quantitative variables.
To assess the magnitude of associations between explanatory variables and AF, we fitted logistic regression models to each variable, estimating the odds ratio (OR) and 95% CI. We then constructed a multivariable model using a backward stepwise selection process based on the Akaike information criterion. Goodness-of-fit indicators were calculated, as was the honest area under the receiver operating curve (AUC) by means of 10-fold cross-validation with 30 repetitions. Analyses were performed with SPSS statistical software (v.18) and the R program (v3.4.2).
Results
A total of 452 people were included, 56.9% (n = 257) of whom were women. The mean age of the sample was 66.9 years (SD 10.3, range 50 to 91). About two-thirds (64.2%) of the participants had hypertension, with a mean evolution of 10.5 years (SD 8.3) and a maximum of 40 years, while 19.0% had diabetes, with a mean evolution of 10.4 years (SD 7.9) and a maximum of 41 years. Table 1 shows the baseline participant characteristics.
Participant Characteristics.a

Abbreviation: CVD, cardiovascular disease.
a N = 452.
During the first reading, 53 possible cases of AF were detected, of which 41 (77.4%) were confirmed on a second reading. The prevalence in the sample was 9.1% (95% CI 6.6%-11.7%). Among the detected cases, 85% (n = 35) scored 2 or above on the CHA2DS2-VASc questionnaire, indicating an elevated risk of stroke.
Table 2 shows the prevalence of AF according to the explanatory variables. AF was more common in older people (14.5% in people aged 75 or older), those who did not do physical activity (12.5%), and people with diabetes (20.9%), dyslipidemia (13.6%), or a history of cardiovascular disease (18.6%).
Prevalence of AF According to Explanatory Variables.a
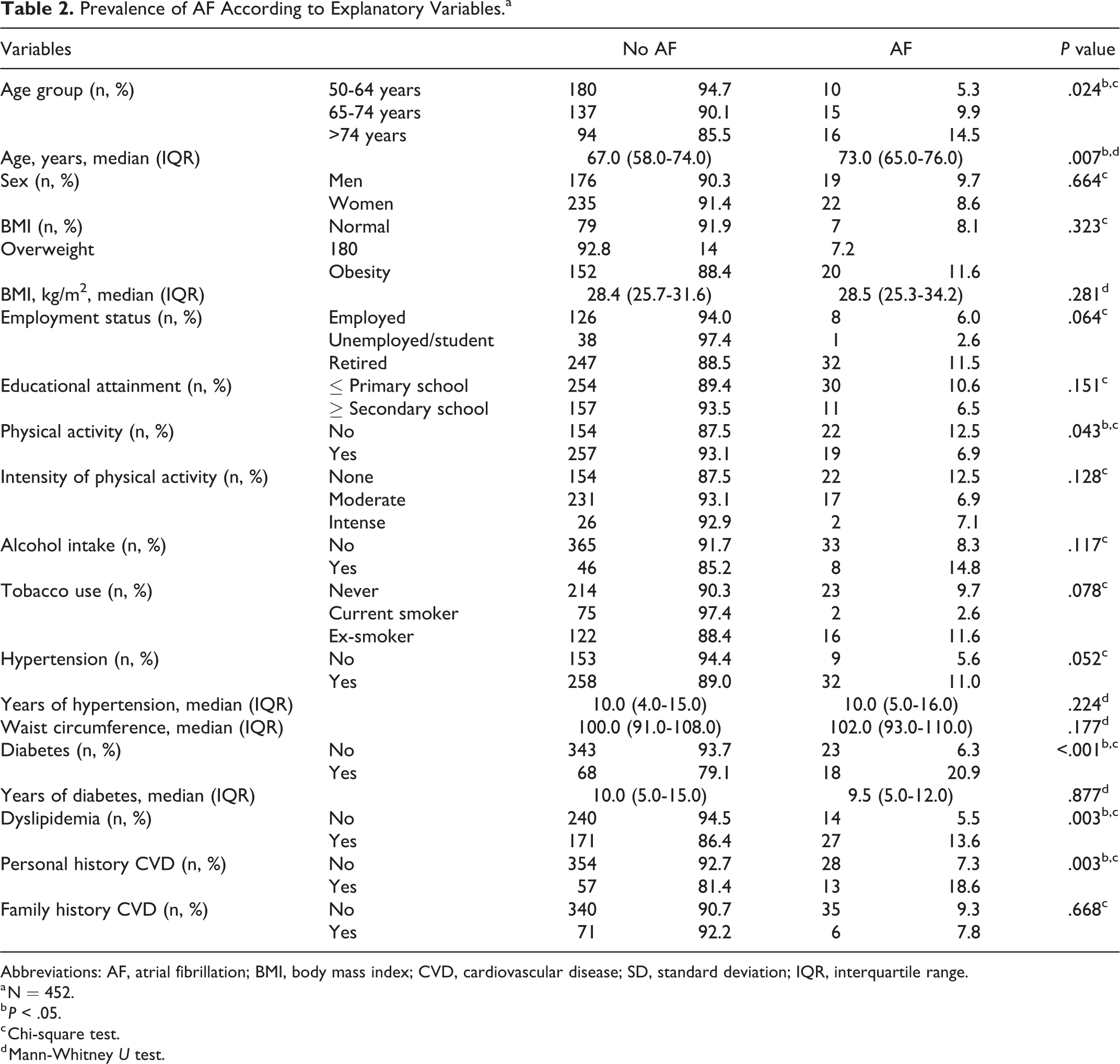
Abbreviations: AF, atrial fibrillation; BMI, body mass index; CVD, cardiovascular disease; SD, standard deviation; IQR, interquartile range.
a N = 452.
b P < .05.
c Chi-square test.
d Mann-Whitney U test.
Multivariable logistic regression showed that diabetes (OR 2.79) and dyslipidemia (OR 2.16) were significantly associated with AF, after adjusting for age (Table 3). The model showed a good fit with the data, with an honest AUC of 0.6384 (95% CI 0.4696-0.8072).
Multivariable Logistic Regression for Prevalence of AF.a

Abbreviations: CI, confidence interval; OR, odds ratio.
a Likelihood ratio test: 22.8 (P value < .001). Honest area under the ROC curve cross-validation: 0.6384 (95% CI: 0.4696-0.8072).
Discussion
The prevalence of AF detected during the screening program for cardiovascular risk was 9.1%, and 85% of these people were at high risk for stroke. The factors associated with AF were advanced age, lack of physical activity, diabetes mellitus, dyslipidemia and history of cardiovascular disease with diabetes and dyslipidemia standing out as the factors with independent explanatory capacity.
Our results for the prevalence of AF in people aged 50 years or older were consistent with other epidemiological studies of AF
28
in primary care settings in Spain. The
Compared to other studies in a pharmacy setting, the results of the CRIFAFARMA study are generally concordant but still sensibly higher. The SEARCH-AF study, 22 in Australian pharmacies, estimated a prevalence of 6.7%, which was higher than that reported by Twigg et al 23 in UK pharmacies, where the rate of positive screens did not exceed 1.5%. The differences in AF prevalence may be attributable to the heterogeneity of the populations studied (age range, ethnicity, presence of risk factors among included participants), the strategy for recruiting people to the screening program, and/or the detection methods used. CRIFAFARMA made use of a non-electrocardiographic device, the Microlife WatchBP Home. This device, one of the best BPMs studied, is capable of identifying possible cases of AF when at least two out of 3 readings indicate an irregular pulse. It has a sensitivity of approximately 80% to 100% and a specificity of about 89% to 99%, and it is less susceptible to observer bias than manual pulse measurement to detect asymptomatic AF in primary care. 15 In contrast, the Australian pharmacy study 22 used manual pulse measurement and a mobile ECG app with the AliveCor cardiac monitor, and the British pharmacy study 23 used the Microlife WatchBP Office Afib device for initial screening, with follow-up of positive results made with the AliveCor ECG app and interpreted by a cardiologist. The most recent study 24 on early detection of AF, using the same device as the CRIFAFARMA study, BPmonitorig Microlifite, found a prevalence of AF of 3.2%, lower than the rate reported in the present study. Similarly, other previous studies 33,34 also found a lower prevalence of AF than that found in this study. The reason for this may be due to the different inclusion criteria of patients used in these studies exploring the general population, while CRIFAFARMA selected the patients who attended their community pharmacy for the control and follow-up of any cardiovascular vascular risk factor. This likely explains the higher prevalence of AF among the CRIFAFARMA study patients.
Cost-effectiveness was not calculated in the present study. A similar study carried out in Canada showed that interventions aimed at the early detection of AF and subsequent treatment in community pharmacies were a cost-effective strategy by reducing the costs generated by stroke due to untreated AF. 35 Previous work carried out in community pharmacies has shown that screening and early detection of AF are effective and cost-effective strategies that can play a key role in stroke prevention, playing a prominent role in more underserved rural settings where there is a greater risk in relation to urban areas. 36 -40
Other studies of AF screening in Spanish primary care have used manual pulse measurement, a specific but low-sensitivity technique, reporting prevalence estimates of up to 6.8% in people with signs and symptoms of AF 41 and 1.1% in opportunistic screening. 14
The results of other studies, 7,15 reporting an increase in AF with age, were confirmed in ours, with the group of people aged 75 years or older showing the highest prevalence of AF (14.5%), compared to 9.9% in those aged 65 to 74 years and 5.3% in those under 65.
Currently, there is no blanket recommendation to screen for silent AF in people under the age of 65 years; however, the Microlife WatchBP Home can be considered appropriate for evaluating people aged 50 or older who have associated risk factors. Indeed, compared to the general population, those with conditions like diabetes and hypertension are at higher risk of developing this arrhythmia. 16 Moreover, the presence of AF could explain the 1.5% prevalence of stroke in people aged 50 to 59 years. 42 As suggested by a Cochrane systematic review, 43 this risk factor for stroke is important enough to justify further studies into AF screening, both in healthcare settings (including community pharmacies) and in younger population groups. In our study, the prevalence of AF in the youngest group studied (50 to 64 years) was 5.3%. In addition, 11% of participants with hypertension had a positive screen for AF, and although this result was slightly above the cutoff for statistical significance (P = .052), it is enough to establish an association 44,45 between AF and hypertension.
To identify factors associated with AF, we fitted a multivariable logistic regression model, which showed that the factors related to the appearance of AF were diabetes, dyslipidemia, and advancing age. This finding has important implications considering that these factors are already included in cardiovascular risk monitoring offered in pharmacies, suggesting a unique opportunity to establish strategies for the early detection of AF. In addition, the European Society of Cardiology mentions in its guidelines for the diagnosis and management of AF that pharmacies can play an important role in the early detection of this problem. 46
Limitations
Limitations of the study include those inherent to the opportunistic screening method used, such as increased morbidity for cases whose prognosis is not altered, overtreatment, resource expenditure, false sense of security in false negative results, anxiety, and sometimes morbidity, in false positive results, risk of the screening test. 47 However, we considered that screening was capable of detecting medical conditions at an early stage, before the onset of symptoms, and this could help to save lives or avoid some complications like stroke. Despite the lack of access to data from clinical records, the necessary data for the study were collected through the clinical interviews.
To avoid measurement bias, the instrument used for detecting AF was calibrated and validated, and the investigators in charge of taking measurements were always the same. These professionals had received prior training to minimize variations in the blood pressure measurements and AF screening. Moreover, all of the field investigators followed a strict and systematized study protocol. Another possible limitation could be due to not reach sufficient statiscal power in the secondary objective of identifying the factors associated with AF. Future studies focused on this objective should take into account a sufficient sample size to detect the proposed effects.
On the other hand, the patients, at the end of the opportunistic screening, received a report of the results of the blood pressure measurement and the result of the presence or absence of AF. However it was not collected whether there was subsequent confirmation by 12-lead ECG. Furthermore, since the measurement was repeated at least 1 hour after the first one if irregularities in the pulse were detected (following the device instructions), it was possible that the patient returned to normal sinus rhythm in that time period. If the first measurement is positive could be a warning sign. Thus, in clinical practice, it would be more operative if the patients are referred to their physician after a first positive test. Further research is needed to assess the patient perception or satisfaction since it was not measured in the present study.
Implications for Clinical Practice
To address the upward trend in AF prevalence over the next decades, it is important to focus on all components of the care spectrum, from early detection and diagnosis to treatment. 48 Experts and professional societies recommend screening for AF in high-risk populations, as people with undiagnosed and asymptomatic AF carry an elevated risk of stroke.
The key to reducing the risk of stroke associated with AF is its early detection. These patients should undergo an evaluation of stroke risk using instruments like the CHA2DS2VASc questionnaire in order to initiate oral anticoagulant therapy and reduce this risk. Similarly, people receiving this treatment should be assessed for their risk of major bleeding through tools like the HAS-BLED score, in order to optimize pharmacotherapy and limit the risk of bleeding. Early diagnosis of AF is a challenge, and many patients are not diagnosed until the onset of significant symptoms or the incidence of a stroke 49 ; however, stroke risk is just as high in people with asymptomatic as in symptomatic AF. 50 Thus, screening programs like the one described here represent an improvement in planning strategies to optimize early detection of AF in pharmacies.
The pharmacies that participated in this study continue to perform AF screening tests, although they do not receive any reimbursement for providing this service, being especially accessible to the population. The future is an opportunity for community pharmacy to play a broader role and for pharmacists to transform from drug dispensers to healthcare providers, critical to ensuring a future in which the profession can develop and prosper as a fundamental part in the search for efficiency and access to the health system. From the community pharmacy, a very important health work could be carried out both in the prevention, screening and control of diseases, as well as in the early detection of AF during the routine measurement of blood pressure. Top barriers that may appear in community pharmacy screening programs may be predisposition on the part of pharmacists, lack of integration within the health system, lack of specific training in AF and no remuneration.
At the same time, a model capable of predicting risk could contribute to a specific framework that could be applied to the population and to the development of intervention strategies to minimize the impact of AF. 51 Such a risk model could reduce the need to wait for arrhythmias to manifest and decrease the incidence of stroke. Risk stratification would also help to predict the risk of future problems and proactively implement preventive interventions. 52 Considering that some predictive risk factors are already included in monitoring and control programs for cardiovascular risk factors, our results open the door to establishing strategies for the early detection of AF in people who use community pharmacies to monitor their cardiovascular risk. Specific interventions can then be implemented in this population to reduce the prevalence of modifiable risk factors, support them in making healthy behavioral changes, 53 and take advantage of the collateral benefits of this screening service, like the identification of patients with hypertension and those at high risk of stroke.
Conclusions
In a screening program for AF in people aged 50 years or older presenting to community pharmacies for monitoring and control of cardiovascular risk factors, the estimated prevalence of AF was 9.1%, and 85% of these people presented an elevated risk of stroke. Factors associated with AF were advanced age, lack of physical activity, diabetes mellitus, and dyslipidemia.
Footnotes
Authors’ Note
All the authors have participated and agree with the content of this article.
Author Contributions
All authors have contributed equally to drafting and revising this manuscript and agree the content is ready for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.