
Abstract
Background:
Ticagrelor is a recommended P2Y12 receptor inhibitor after acute coronary syndrome (ACS). Its superiority has been suggested to rely on pleiotropic effects beyond platelet inhibition. Experimental studies indicate that ticagrelor may protect from ischemia-reperfusion injury but no data are available from such studies on patients. This study aimed to determine if chronic ticagrelor treatment protects against endothelial ischemia-reperfusion injury in patients with a previous ACS.
Methods:
Patients with a previous ACS were studied with flow mediated dilatation of the left brachial artery to determine the degree of endothelial ischemia-reperfusion injury before and after discontinuation of ticagrelor treatment, which had been continuous since 1 year. Each patient underwent 3 identical examinations. The first examination (Visit A) was at the end of ticagrelor treatment and the following 2 (Visit B and C) were after cessation of this treatment with an interval of 2 to 4 weeks.
Results:
Ischemia and reperfusion induced significant impairment of endothelial function at all 3 occasions (absolute decline in flow mediated dilatation 3.0% ± 0.7 at Visit A (P < 0.001), 1.9% ± 0.9 at Visit B (P < 0.05) and 1.9% ± 0.4 at Visit C (P < 0.0001)). However, there was no difference in the degree of endothelial ischemia-reperfusion injury or baseline endothelial function between the visits.
Conclusion:
Chronic ticagrelor treatment in patients 1 year after an ACS does not protect against endothelial ischaemia-reperfusion injury. Nor is it associated with better basal endothelial function compared to after discontinuation of treatment.
Keywords
Introduction
Ticagrelor is a recommended P2Y12 receptor inhibitor to achieve dual antiplatelet therapy (DAPT) after an acute ST-elevation myocardial infarction (STEMI). 1,2 The PLATO (Platelet Inhibition and Patient Outcomes) trial showed a decrease in mortality, myocardial infarction and stroke in patients with acute coronary syndrome (ACS) treated with ticagrelor as compared to clopidogrel. 3 Current guidelines suggest prolonging this treatment beyond 12 months for patients with high ischemic and low bleeding risk, but the level of evidence is low. 4 Furthermore, the underlying mechanism(s) responsible for this prolonged protection are not clear. 5,6 While ticagrelor achieves greater and less variable P2Y12 inhibition than clopidogrel, 7 it also has a unique pleiotropic effect to inhibit adenosine cell reuptake through inhibition of the equilibrative nucleoside transporter 1 (ENT1), 8 with the potential to increase extracellular adenosine levels in patients with ACS. 9 This is of potential clinical interest in the STEMI-setting as it has been demonstrated that adenosine protects against ischemia-reperfusion injury. 10,11 Accordingly, ticagrelor has been shown to attenuate myocardial ischemia-reperfusion injury in an adenosine-dependent manner in rat 12,13 and pig models 14,15 of coronary artery occlusion and reperfusion. In healthy humans, ticagrelor increases coronary blood flow 16 and attenuates endothelial dysfunction induced by ischemia-reperfusion compared to clopidogrel, 17 but there is conflicting evidence concerning its effect on endothelial function in patients with established coronary artery disease. 6 Furthermore, any protective effect of ticagrelor against ischemia-reperfusion injury has not been evaluated in patients with established coronary artery disease.
Collectively, available data indicate that ticagrelor may interfere with ischemia-reperfusion injury. However, any specific effect of ticagrelor on ischemia-reperfusion injury in patients with established coronary artery disease has not previously been studied. In the present study, we aimed to investigate if ticagrelor protects against endothelial ischemia-reperfusion injury in patients with a previous ACS.
Methods
Study Subjects
The Swedish Web-system for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recommended Therapy (SWEDEHEART) registry 18 was used to identify male patients with a previous ACS awaiting their scheduled clinical 1-year follow-up visit at one of the 3 recruiting hospitals in the Stockholm area (Karolinska University Hospital Solna, Karolinska University Hospital Huddinge and Danderyd Hospital). At the present time, all patients with age ≤75 years treated for an ACS in Sweden were included in the follow-up part for secondary prevention of the SWEDEHEART registry. Twenty eligible patients (non-diabetics with ongoing ticagrelor treatment 90 mg twice daily) were recruited by telephone calls and written informed consent was acquired from all patients. The study was approved by the regional ethics committee in Stockholm and was conducted according to the Declaration of Helsinki. 19
Study Protocol
The endothelial function of enrolled patients was evaluated by flow mediated dilatation (FMD) on 3 occasions as according to the protocol illustrated in Figure 1. The first examination (Visit A) was performed at the end of the planned 12-month period of ticagrelor treatment after which the drug was discontinued. Examination 2 (Visit B) took place 2 to 4 weeks later. A third examination (Visit C) was performed after an additional 2 to 4 weeks to evaluate change in FMD over time. All study participants were overnight fasting before the examinations and they refrained from tobacco products and caffeine-containing drinks on the study days. The patients were asked to remain with their regular activities during the study period and instructed to take their morning medication on the study days 1 to 2 hours before the examinations (including ticagrelor at Visit A). All examinations were performed in the morning in a quiet dimly lit temperature-controlled (21-24°C) room. A venous catheter was introduced in a superficial vein in the right antecubital fossa for collection of blood samples. The left arm was used for determination of endothelium-dependent vasodilatation using FMD. After determination of basal FMD the left arm was subjected to 20 min of ischemia by inflating a blood pressure cuff placed around the upper arm to 200 mm Hg for 20 min. After 20 min of reperfusion a second FMD was performed. The change in FMD between baseline and after ischemia-reperfusion illustrates the degree of endothelial impairment. 20 Endothelium-independent vasodilatation was determined by sublingual administration of 0.4 mg of nitroglycerine at the end of the examination. Nitroglycerine was not administered before ischemia due to its long-acting vasodilatation which may influence baseline radial artery diameter following ischemia. The effect of exogenously administered NO donors is not affected by ischemia-reperfusion. 21

Study protocol. First visit was at the end of the planned 12-month period of ticagrelor treatment, after which the drug was discontinued. Second and third visits were performed with 2 to 4 week intervals to the previous one. EID = endothelium independent dilatation; FMD = flow mediated dilatation.
Flow-Mediated Dilatation
Endothelial function was assessed by determination of FMD of the brachial artery of the left arm as previously described elsewhere. 22 Briefly, an 11 MHz (output 12 MHz) linear-array transducer, mounted on a flexible tripod (to prevent movement of the probe) and connected to a Vivid E9® (GE, Waukesha, Wisconsin, USA) was used to record ECG-gated images of baseline artery diameter at end-diastole. A blood pressure cuff was inflated to 200 mmHg for 5 min around the upper part of the left forearm and then deflated. Maximum dilatation of the brachial artery during the following hyperaemia was determined. The Brachial Analyzer software (Medical Imaging Applications, Iowa, IA, USA) was used for image analysis. FMD was calculated as percentage increase from baseline diameter [(diameter following cuff deflation-baseline diameter)/baseline diameter x 100]. Evaluations were performed by a blinded technician. Intra-observer variability for FMD was 0.1 ± 3.9 (bias and SD). 23
Analysis of Platelet Inhibition
At the beginning of each visit, 3 mL of venous blood was collected in a Hirudin-containing tube and immediately delivered to the hospital laboratory to be tested within 2 hours of sampling. The degree of platelet inhibition was evaluated with impedance aggregometry (Multiplate, Roche Diagnostics). 24 ADP-test (platelet function after stimulation of platelet adenosine diphosphate receptors) was used to test the effect of ticagrelor and ASPI-test (platelet function stimulated by arachidonic acid) was used to test the effect of aspirin. Simultaneous analysis of platelet count (using EDTA containing tubes) was performed to confirm platelet counts above 50 x 109/L.
Statistical Analysis
The primary endpoint of the study was change in FMD after ischemia-reperfusion from baseline. The magnitude of any possible protective effect of ticagrelor against endothelial ischemia-reperfusion injury was unknown to us. However, based on the assumption of a degree of protection comparable to that achieved in our previous studies of protection against endothelial ischemia-reperfusion injury, 23,25 we estimated an absolute improvement in FMD of 1.3%. Based on a standard deviation of 1.8%, 15 patients were needed to achieve 80% power at a significance level of 5%. To compensate for possible dropouts and examinations with poor image quality, 20 volunteers were recruited. Normality of data was tested using D’Agostino and Pearson normality test. Change in FMD at each visit (induced by ischemia-reperfusion) was analyzed with paired t-test. Comparison of platelet inhibition, baseline endothelial function and endothelial ischemia-reperfusion injury between visits was made with 1-way ANOVA and Tukey’s multiple comparisons post-hoc test was used where appropriate. Statistical analyses were made with GraphPad Prism version 6.05 for Windows (GraphPad software, La Jolla California USA, www.graphpad.com). Values of P < 0.05 were considered to be statistically significant.
Results
Study Subjects
All patients arrived to all visits, completing a total of 60 examinations. Baseline characteristics of the patients are described in Table 1.
Baseline Characteristics.

Medians and interquartile ranges or numbers and percentages. N = 20. BMI = body mass index; CRP = C-reactive protein; DBP = diastolic blood pressure; fP = fasting plasma; GFR = glomerular filtration rate; HDL = high-density lipoprotein; LDL = low-density lipoprotein; SBP = systolic blood pressure; ACE-I = angiotensin converting enzyme-inhibitor; ARB = angiotensin II receptor blocker; TG = triglycerides.
Flow-Mediated Dilatation
After exclusion of examinations due to poor image quality or motion artifacts, 17 patients remained in the final analysis. There was no significant difference in baseline brachial artery diameter or maximal flow velocity during hyperaemia (Table 2).
Brachial Artery Diameter and Peak Flow Velocity From Visits A-C.

Means and SEM. P > 0.05 for comparisons within each variable. n = 17. IR = ischemia-reperfusion.
Baseline FMD did not differ significantly between the 3 visits (Figure 2; P = 0.07). Ischemia-reperfusion significantly attenuated endothelium-dependent vasodilatation at all 3 examinations. The absolute change in FMD from baseline to 20 min of reperfusion was -3.0% ± 0.7 at Visit A, -1.9% ± 0.9 at Visit B and -1.9% ± 0.4 at Visit C (Figure 3). There was no significant difference in the degree of endothelial impairment induced by ischemia-reperfusion between the examinations (P = 0.39).

FMD before and after ischemia-reperfusion at each visit. bars mark mean and whiskers mark SEM (n = 17). Data were analyzed with 1-way ANOVA. FMD = flow mediated dilatation; IR = ischemia-reperfusion; SEM = standard error of the mean. Significant differences between baseline and IR visits are depicted; *P < 0,05, ***P < 0.001.

Absolute change in FMD from baseline induced by ischemia-reperfusion illustrating the degree of endothelial ischemia-reperfusion injury at each visit. Bars mark mean and whiskers mark SEM (n = 17). There are no significant differences between visits. Data were analyzed with 1-way ANOVA. FMD = flow mediated dilatation; SEM = standard error of the mean.
Nitroglycerine-Induced Dilatation
There was no significant difference in endothelium-independent dilatation of the brachial artery induced by sublingual nitroglycerine between the examinations (Visit A: 14.3 ± 1.5%; Visit B: 13.3 ± 1.7%, Visit C: 12.1 ± 1.4%; P = NS).
Platelet Inhibition
There was a marked impairment of platelet function as measured by Trc-ADP during treatment with ticagrelor at visit A compared to after the discontinuation of treatment at Visits B and C (Table 3). Trc-ASPI was slightly but significantly lower at Visit A than at the other occasions.
Platelet Inhibition. Means and SEM.
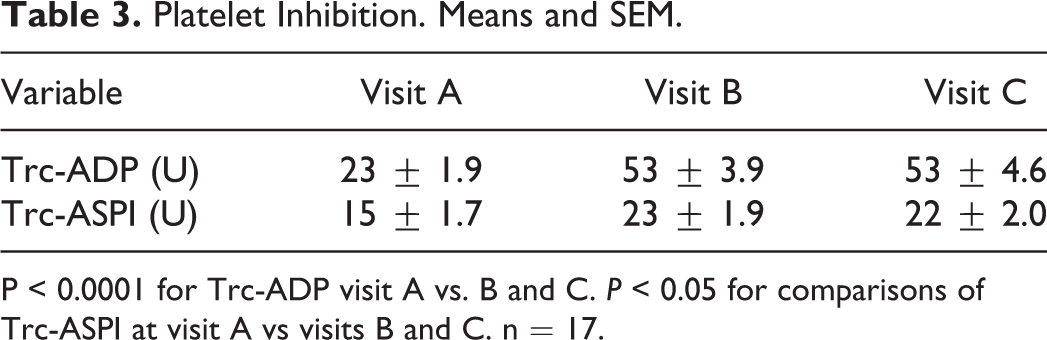
P < 0.0001 for Trc-ADP visit A vs. B and C. P < 0.05 for comparisons of Trc-ASPI at visit A vs visits B and C. n = 17.
Discussion
Pleiotropic effects of ticagrelor possibly contributing to cardioprotection have been receiving increasing interest. 26 The present study is to the best of our knowledge, the first to investigate the effect of ticagrelor on ischemia-reperfusion injury in patients with established coronary artery disease. The results show that treatment with ticagrelor did not confer protection against ischemia-reperfusion injury or improve endothelial function in patients with previous ACS.
Comparing the 2 P2Y12-blockers clopidogrel and ticagrelor, the PLATO-trial found superior cardiovascular outcomes and survival for the latter. 3 Animal studies have shown that treatment with ticagrelor is superior to clopidogrel in reducing myocardial infarct size after ischemia-reperfusion, despite similar degree of platelet inhibition, indicating a pleiotropic cardioprotective effect of ticagrelor. 12 -14,27 Cardioprotective effects of ticagrelor were observed both following a loading dose in connection with the ischemia-reperfusion and following chronic treatment. Beyond being a P2Y12 receptor antagonist, ticagrelor also inhibits adenosine uptake by erythrocytes through inhibition of ENT1, thereby increasing extracellular adenosine concentrations. 8 Interestingly, ENT1-null mice are protected against myocardial ischemia-reperfusion injury in an adenosine-dependent manner compared to wild-type animals. 28 Additionally, adenosine has cardioprotective properties in the STEMI-setting. 10,11 These observations indicate that the inhibition of adenosine uptake by ticagrelor may be of potential therapeutic value. Furthermore, there is increasing awareness that co-medication might have an impact on the outcomes of current trials evaluating new cardioprotective strategies. 29 As ticagrelor is established as a P2Y12-inhibitor of choice in STEMI it is important to fully understand the clinical implications of its pleiotropic effects beyond platelet inhibition.
We therefore investigated the effect of ticagrelor on an established model of ischemia-reperfusion injury in humans. The forearm model has previously been used for investigations of interventions targeting ischemia-reperfusion injury in healthy subjects and patients with coronary artery disease. 22,30 In agreement with previous results forearm endothelium-dependent vasodilatation was markedly attenuated by ischemia-reperfusion. However, ticagrelor treatment did not protect against the development of endothelial dysfunction despite therapeutic efficacy by ticagrelor treatment as demonstrated by adequate degree of platelet inhibition. These results suggesting that ticagrelor does not confer protection against ischemia-reperfusion injury in patients 1 year after ACS are in contrast to those of Weisshaar et al showing a protective effect of ticagrelor against endothelial ischemia-reperfusion injury in healthy humans, 17 and to previous animal studies demonstrating cardioprotective effects of ticagrelor both when given as an acute loading dose and as chronic treatment. 12 -14,27 The specific reasons for the discrepancies in results are presently unclear. Important contributing factors include species differences, age of subjects, co-medication, co-morbidities and the use of the surrogate endpoint endothelial functions, which highlight the well-known translational challenges associated with research in cardioprotection. 29,31
Previous studies have indicated that ticagrelor may have beneficial effects on baseline endothelial function. Torngren et al found that patients with a previous ACS and ongoing ticagrelor treatment since 3 to 12 months had better endothelial function than patients treated with clopidogrel or prasugrel. 32 Fromonot et al showed that endothelial function was improved in patients with a recent ACS after 30 days of ticagrelor treatment compared to clopidogrel treatment and this effect correlated to a significant increase in plasma adenosine levels. 33 We found no significant beneficial effect of treatment with ticagrelor on baseline endothelial function in the present study. This observation gives support to and extends the results of the study of Xanthopoulou et al that demonstrated no deterioration in endothelial function within 5 days after discontinuation of ticagrelor treatment. 34 Additionally, Ariotti et al studied patients with a previous ACS to compare the effect of 4 weeks of treatment with ticagrelor, clopidogrel and prasugrel respectively and detected no improvement in endothelial function in response to treatment with ticagrelor. 35 Furthermore, Lim et al showed that 30 days of ticagrelor treatment did improve baseline endothelial function in patients with a recent ACS. 36 Thus, any beneficial effect of ticagrelor on baseline endothelial function in patients with cardiovascular disease remains to be established.
Our study has certain important limitations. First, we did not investigate the effect of a bolus dose of ticagrelor to ticagrelor-naïve patients and any extrapolation of the results to the acute setting should be done with great caution. Second, we did not measure plasma adenosine and thereby no conclusions can be made on the specific ability of chronic ticagrelor treatment to affect these levels. Third, we did not measure plasma levels of ticagrelor. However, the therapeutic efficacy of ticagrelor treatment, patient compliance and treatment discontinuation were established by determination of significant platelet inhibition. Fourth, the possible impact of co-medication was not explored. However, the study was designed to evaluate the effect of ticagrelor in a clinically significant setting, as reflected by the fact that all patients were on aspirin and statins, and a majority were taking betablockers and ACE-I or ARB. As patients acted as their own controls and medication other than ticagrelor was unchanged, it is unlikely that a possible effect of co-medication altered the outcome of the study. Fifth, the possible influence of strenuous physical exercise was not taken into account, as such data was not gathered for the study period. However, study subjects were instructed to adhere to their regular living habits, to reflect a real life setting. Sixth, this trial was of limited size. However, sample size was according to power calculation. Finally, it is important to keep in mind that endothelial ischemia-reperfusion injury of a conduit vessel in a limb, as investigated in the present trial, might not fully reflect the complex entity of myocardial ischemia-reperfusion injury.
Conclusion
Chronic ticagrelor treatment did not confer protection against endothelial ischemia-reperfusion injury in patients with a previous ACS, nor was it associated with better endothelial function compared to after termination of treatment. Further studies are needed to clarify underlying mechanisms accounting for improved clinical outcomes with prolonged ticagrelor treatment in certain groups of patients.
Footnotes
Abbreviations
ACE-I: angiotensin converting enzyme-inhibitor; ACS: acute coronary syndrome; ARB: angiotensin II receptor blocker; BMI: body mass index; CRP: C-reactive protein; DAPT: dual antiplatelet therapy; DBP: diastolic blood pressure; EID: endothelium independent dilatation; ENT1: equilibrative nucleoside transporter 1; FMD: flow mediated dilatation; GFR: glomerular filtration rate; HDL: high-density lipoprotein; IR: ischemia-reperfusion; LDL: low-density lipoprotein; SBP: systolic blood pressure; SEM: standard error of the mean; STEMI: ST-elevation myocardial infarction; TG: triglycerides.
Authors’ Note
The trial was performed at the Division of Cardiology, Department of Medicine, Karolinska Institutet, Stockholm, Sweden.
Acknowledgments
The authors are grateful to David Ersgård for skilled patient management and FMD examinations.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Swedish Research Council (2016-01284); the Swedish Heart and Lung Foundation (20170354, 20180507, 20190266); the Stockholm County Council (20190031); the Diabetes Research and Wellness Foundation (363-PG) and the EU-CARDIOPROTECTION CA16225 Cooperation in Science and Technology (COST) Action (CA16225).