
Abstract
Background:
There is an incomplete understanding of the prevalence and predictors of attainment of low-density lipoprotein cholesterol (LDL-C) goal after myocardial infarction (MI).
Aim:
To evaluate the prevalence of achievement of LDL-C goal of 70 mg/dL, to identify the baseline features associated with suboptimal lipid control, and to assess the use of LDL-C-lowering drug therapies (LLT) beyond the first year after MI.
Methods:
The EYESHOT Post-MI was a prospective, cross-sectional, Italian registry, which enrolled patients presenting to cardiologist 1 to 3 years after MI. In this retrospective post-hoc analysis, patients were categorized in 2 groups according to the achievement or not of the LDL-C goal of 70 mg/dL. Univariable and multivariable logistic regression analyses were performed to identify the baseline features associate with LDL-C≥70 mg/dL.
Results:
The study population included 903 patients (mean age 65.5 ± 11.5 years). Among them, LDL-C was ≥70 mg/dL in 474 (52.5%). Male sex (P = 0.031), hypertension (P = 0.024), prior percutaneous coronary intervention (P = 0.016) and high education level (P = 0.008) were higher in the LDL-C <70 group. At multivariable analysis, low education level was an independent predictor of LDL-C≥70 mg/dL (OR:1.582; 95%CI, 1.156-2.165; P = 0.004). Conversely, hypertension increased the probability to achieve the LDL-C goal (OR:0.650; 95%CI, 0.443-0.954; P = 0.028). Among off-target patients, LLT was not modified in the majority of cases (67.3%), intensified in 85 (18.6%), and actually reduced in 63 patients (13.8%).
Conclusions:
In patients presenting to cardiologists 1 to 3 years from the last MI event, LDL-C is not under control in a large proportion of patients, particularly in those with a low education level or without hypertension. LLT is underused in this very-high-risk setting.
Introduction
There is a continuous, positive, association between low-density lipoprotein cholesterol (LDL-C) and the risk of major cardiovascular events. 1 -3 Data from randomized controlled trials (RCTs) showed that lowering LDL-C by intensifying statin therapy or adding non-statin agents safely reduces cardiovascular adverse events. 4 -7
Although RCTs have not been designed to assess clinical outcome as a function of specific LDL-C levels, the use of lipid goals can alert clinicians on patient’s residual risk and guide the optimization of LDL-C-lowering drug therapies (LLT). 8 The previous edition of European Society of Cardiology (ESC) guidelines on management of dyslipidemia recommended a low-density lipoprotein cholesterol (LDL-C) serum level of 70 mg/dL in patients with very high total cardiovascular risk. 9 The same LDL-C goal is recommended by the current guidelines of the American College of Cardiology/American Heart Association (ACC/AHA) in this clinical setting. 10
Consistent evidence from meta-analyses support the achievement of the largest LDL-C reduction to prevent atherosclerotic cardiovascular disease (ASCVD) and no lower LDL-C limit to this benefit has been detected. 11,12 Therefore, the 2019 up-to-date ESC guidelines pursues this objective by recommending a further lower absolute LDL-C treatment goal of <55 mg/dL in very-high-risk patients such as those who experienced acute coronary syndrome. 13
The achievement of the LDL-C goal and the adoption of appropriate pharmacological therapy in patients with suboptimal lipid control is a matter of concern in daily practice. To date, few studies have investigated the adherence to guidelines recommendations and patterns in contemporary cardiology practices to reduce LDL-C level in very-high-risk patients such as those who experienced previous MI.
Aim of our study is to evaluate the attainment of LDL-C target level of 70 mg/dL, to identify baseline features associated with a suboptimal LDL-C control, and to assess the use of LLT beyond the first year after MI in the real world.
The EYESHOT registry (EmploYEd antithrombotic therapies in patients with acute coronary Syndromes HOspitalized in iTaly), with nationwide prospective enrolment of patients presenting to cardiologist 1 to 3 years after MI, provides a unique opportunity to evaluate LDL-C level and to describe the secondary prevention strategies adopted in these subjects at very high cardiovascular risk.
Methods
Study Population
The design and primary results of the EYESHOT Post-MI registry have been described in detail elsewhere. 14 In brief, this prospective, cross-sectional, nationwide, Italian registry, enrolled 1633 consecutive patients with a documented history of prior MI occurred between 1 and 3 years before the time of enrolment. The primary objective was to evaluate the clinical characteristics, management and treatment of these very high-risk patients admitted to Italian cardiology centers, using a recruitment broad enough to provide data generalizable to the entire country. Therefore, patients were recruited in cardiology units and/or ambulatory clinics of 165 cardiology centers located in 177 Italian hospitals during a period of 3 months. Enrollment was made at the beginning of outpatient visit or at hospital admission. The patient baseline characteristics, including data on home pharmacological therapy, were collected at the time of recruitment. At the end of visit or hospital discharge, changes in pharmacological therapy, if any, were systematically collected.
In this retrospective post-hoc analysis, we included all the patients for whom LDL-C value was available at the time of enrollment. Patients were categorized in 2 groups according to the achievement or not of the LDL-C goal of 70 mg/dL recommended for subjects at very high risk by both the ESC and ACC/AHA guidelines at the time of enrollment. 10,15
All patients were informed of the nature and aims of the study and asked to sign an informed consent for the anonymous management of their individual data. Local Institutional Review Boards (IRB) approved the study protocol according to the current Italian rules.
Measures
Baseline demographic, clinical, echocardiographic and laboratory data were prospectively collected and recorded on an electronic case report form. Beyond age and gender, the following demographic features were reported: level of education (none, elementary school, secondary school, high school, university), occupation (unemployed, housewife/houseman, pension, employed), number of books in the house (<10, 11-25, >25) and number of persons in household. Education level was defined low for patients with none, elementary- or secondary-school degree. Patients with high education level included those graduated from high school or university.
Pharmacological therapy was collected both at baseline and at the end of visit or hospital discharge. The following LLT agents were systematically reported: statins, ezetimibe, proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors, fibrates and omega-3 fatty acids. Statins were also grouped according to their intensity as follows
10,16
high intensity: atorvastatin 80 mg, atorvastatin 40 mg, rosuvastatin 40 mg and rosuvastatin 20 mg; moderate intensity: atorvastatin 20 mg, atorvastatin 10 mg, rosuvastatin 10 mg, rosuvastatin 5 mg, simvastatin 40 mg, simvastatin 20 mg, lovastatin 40 mg; low intensity: simvastatin 10 mg.
By combining data on statin intensity and the combination with non-statin agents at baseline and at the end of visit/discharge, we identified patients in whom treatment was intensified, remained unchanged or was reduced. Definitions of LLT changes from baseline to the end of the visit/discharge are detailed in the Supplemental material.
Statistical Analysis
Distribution of continuous data was tested with the Kolmogorov–Smirnov and the Shapiro-Wilk tests. Normally distributed variables were expressed as mean ± standard deviation (SD), and compared using the Student t test, whereas non-normally distributed variables as median and interquartile range (IQR) and compared with the Mann-Whitney U test. Categorical variables were reported as numbers and percentages and compared using the χ2 or Fisher exact tests, as appropriate.
Clinically relevant variables were included in univariable logistic regression analysis to identify the baseline features associated to the failure in the achievement of the LDL-C goal (≥70 mg/dL) at the time of enrollment. A multivariable stepwise logistic regression model was performed to identify a set of independent predictors of LDL-C ≥ 70 mg/dL. Results were reported as odds ratios (OR) with 95% confidence intervals (CI).
Moreover, an explorative analysis was conducted to evaluate the LLT changes according to LDL-C goal <55 mg/dL. For all tests, a P value of <0.05 was considered statistically significant. All tests were 2-sided. Analyses were performed with SPSS system software, version 24.
Results
Baseline Features and Predictors of Failure to Achieve the LDL-C Goal
The study population included 903 patients (mean age 65.5 ± 11.5 years; 79.6% males). Of them, 429 (47.7%) showed LDL-C values < 70 mg/dL, 474 (52.5%) ≥70 mg/dL.
The baseline characteristics are reported in Table 1. There was no difference in terms of age between groups. Off-target patients were more often females (23.2% vs. 17.2%, P = 0.031) and with prior history of hypercholesterolemia (79.4% vs. 70.4%, P = 0.002). Noteworthy, the rate of hypertension (81.5% vs. 75.3%, P = 0.024) and prior percutaneous coronary intervention (PCI; 92.3% vs 87.3%, P = 0.016) was significantly higher among patients with a better control of LDL-C serum levels.
Baseline Characteristics of the Study Population (N = 903).

BMI, body mass index; CABG, coronary artery bypass graft; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; LDL-C, low-density lipoprotein cholesterol; MI, myocardial infarction; NSTEMI, non-ST-elevation myocardial infarction; PAD, peripheral artery disease; PCI, percutaneous coronary intervention; SBP, systolic blood pressure; STEMI, ST-elevation myocardial infarction; TIA, transient ischemic attack. *Clinically evident bleeding with haemoglobin reduction ≥2g/dL or requiring transfusion or hospitalization.
The majority of patients presented a low education level (445, 59.0%); of them, 170 (38.2%) had elementary school or none degree (Table 2). There was a statistical, graded, association between LDL-C and the level of education (P = 0.020). Patients with higher degree (high school of university) showed a significantly better control of LDL-C value compared to those with low education level (P = 0.008).
Demographic Features of the Study Population (N = 903).

LDL-C, low-density lipoprotein cholesterol.
§ Data available: 754 pts.
* Low education level was defined as none, elementary school or secondary school degree.
** High education level was defined as high school or university degree.
The 50.8% of patients included in the analysis were retired, whereas 5.9% and 8.2% were unemployed or housewife/houseman, respectively. There was no difference in terms of occupation, number of books and of persons in household between the groups of interest.
At multivariable logistic regression analysis, low education level was an independent predictor of LDL-C≥70 mg/dL (OR: 1.582; 95%CI, 1.156-2.165; P = 0.004). Conversely, the history of hypertension was associated with the achievement of LDL-C goal (OR: 0.650; 95%CI, 0.443-0.954; P = 0.028) (Table 3).
Predictors of LDL ≥70 mg/dl in the Study Population (N = 903).
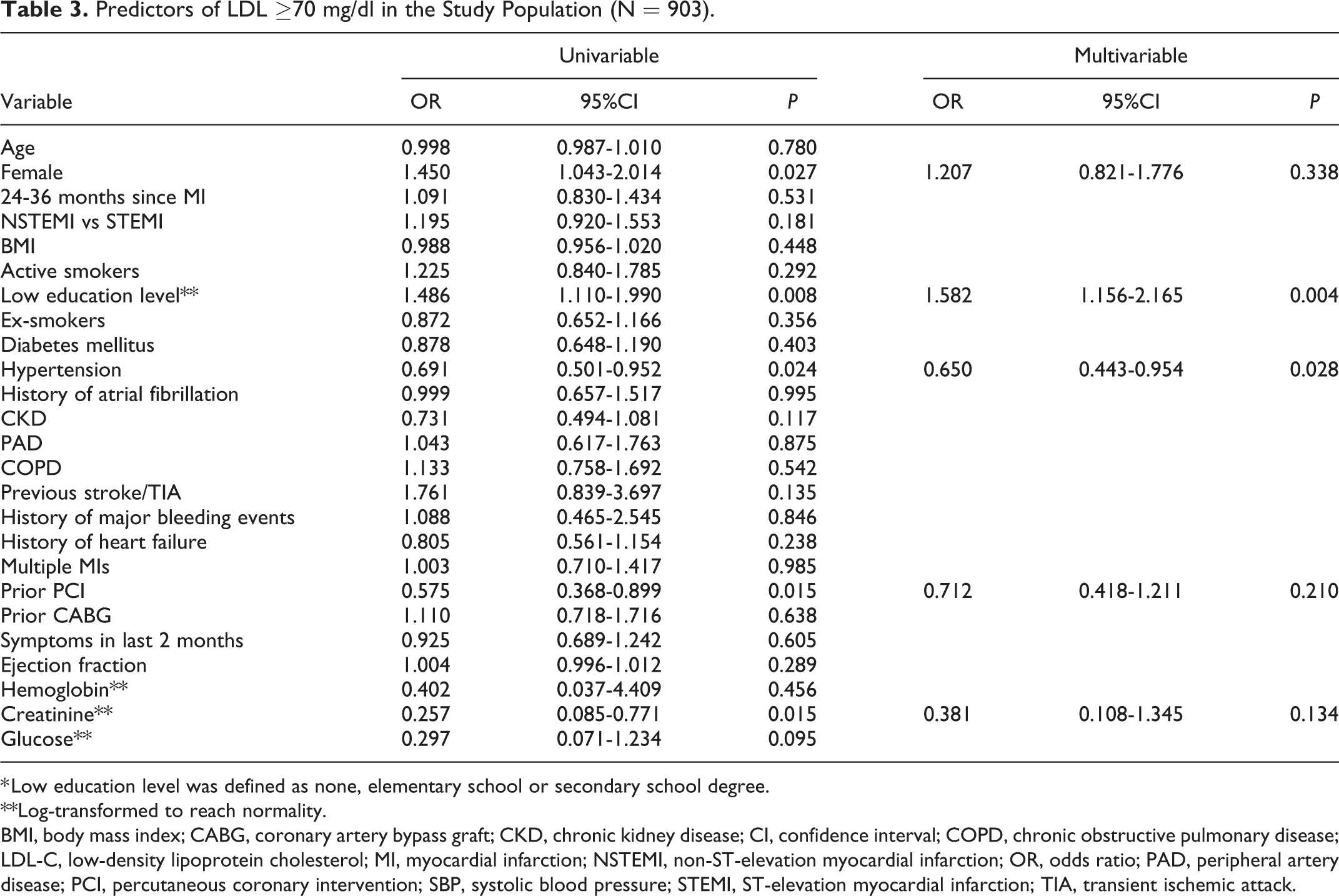
* Low education level was defined as none, elementary school or secondary school degree.
**Log-transformed to reach normality.
BMI, body mass index; CABG, coronary artery bypass graft; CKD, chronic kidney disease; CI, confidence interval; COPD, chronic obstructive pulmonary disease; LDL-C, low-density lipoprotein cholesterol; MI, myocardial infarction; NSTEMI, non-ST-elevation myocardial infarction; OR, odds ratio; PAD, peripheral artery disease; PCI, percutaneous coronary intervention; SBP, systolic blood pressure; STEMI, ST-elevation myocardial infarction; TIA, transient ischemic attack.
Lipid-Lowering Pharmacological Therapy
Medications at baseline are shown in Supplementary Table 1, Statin therapy was reported in 841 (93.1%) patients, with a greater use in the LDL-C <70 group (P = 0.001). Atorvastatin was the most prescribed one (716, 85.0%) and its use was significantly prevalent in patients on-target (P = 0.026). Overall, there was no difference in terms of statin intensity. Non-statin drugs were taken by 214 (23.7%) patients, and in 196 (21.7%) were associated with statins. Non-statin therapy consisted of ezetimibe (147, 16.3%) and/or omega-3 fatty acids (74, 8.2%) in the majority of cases, whereas the use of fibrates and PCSK9 inhibitors was marginal (4 patients for each class of drugs). No therapy with bile acid sequestrants was reported. No difference in the use of statins in combination with other LLT agents were detected among groups.
Figure 1 and Supplementary Tables 2-5 detail changes of statin intensity and/or of other non-statin agents from baseline to the end of the visit/discharge. Among 474 patients with LDL-C ≥70 mg/dL, statin therapy was intensified only in 31 (6.5%). Overall, LLT was unchanged in 626 (71.6%) patients at the end of the visit/discharge, intensified in 103 (11.8%) and reduced in 150 (16.0%) (Supplementary Table 5). Among off-target patients, LLT was not modified in the majority of cases (67.3%) and intensified in only 85 (18.6%).
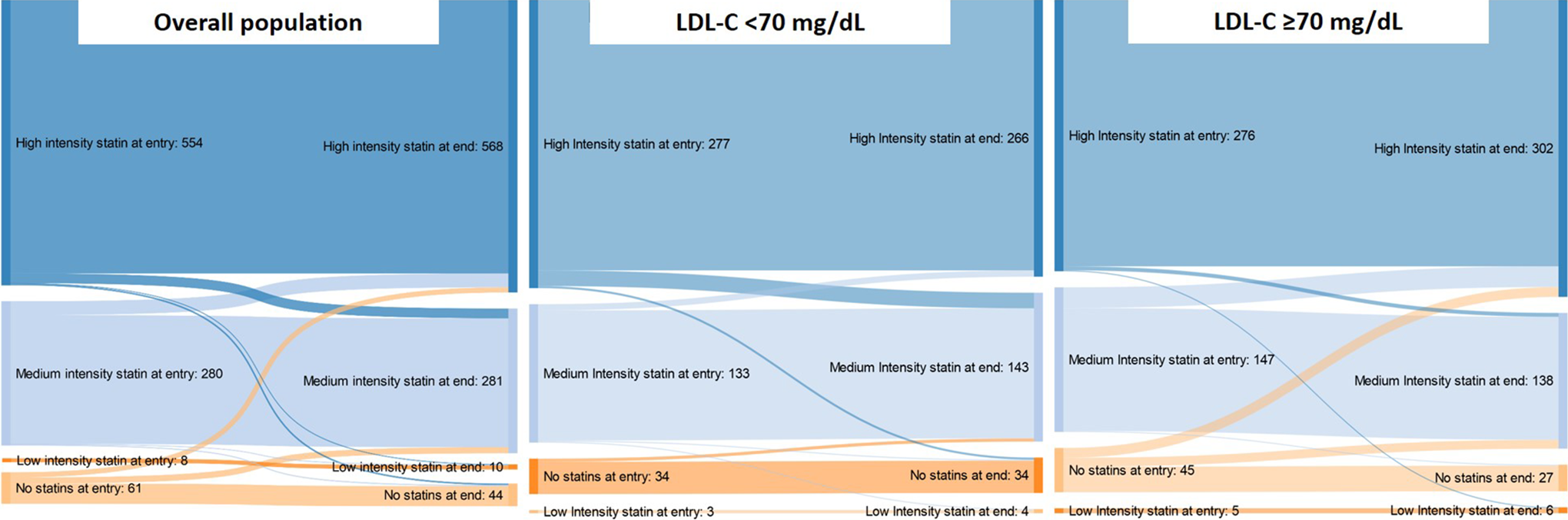
Changes of statin therapy intensity from the baseline to the end of the visit/discharge in the overall population and in the study groups.
The exploratory analysis using the LDL-C cut-off of 55 mg/dL is reported in Supplementary Table 6. Patients with LDL-C level ≥55 mg/dL underwent LLT intensification in only 13.7% of cases; LLT was unchanged in 477 patients (68.0%) and was even reduced in 101 (14.4%).
Discussion
The main findings of the current analysis can be summarized as follows: 1) the LDL-C goal recommended by 2016 guidelines was achieved in less than half the study population; 2) a low education level was an independent predictor of LDL-C ≥70 mg/dL; 3) patients with history of hypertension showed a better lipid control and hypertension by itself was independently associated with the achievement of the LDL-C goal; 4) LLT is underused, particularly in those who did not achieve the LDL-C goal.
LDL-C is a leading, modifiable, risk factor for cardiovascular disease and its control is strongly recommended by current guidelines. Our study demonstrates that the lipid goal is not reached in more than half of cases and emphasizes that management of elevated LDL-C levels 1 to 3 years after MI is still suboptimal in the real world. These results are consistent with data from the EUROASPIRE surveys, which investigated primary and secondary preventive practices in patients with established coronary heart disease in Europe since 1995-1996. 17 The most recent survey (EUROASPIRE V) reported the achievement of LDL-C <70 mg/dL in less than 30.0% of cases; this percentage was slightly higher among those on high-intensity LLT. 18 A recent subanalysis from the EPHESUS study, a cross-sectional Turkish registry enrolling patients with atherosclerotic diseases, documented the achievement of the LDL-C goal in only 18% of cases. 19 The attainment of LDL-C target was even lower in a cohort of patients with recent acute coronary syndrome enrolled in a retrospective Germany registry, being observed in just 11.5% of cases. 20
In comparison with these studies, our analysis included a selected population of subjects who experienced MI more than a year prior enrollment. In this patient setting, we found a large proportion of patients out of LDL-C target, which emphasizes the high necessity to implement the guidelines in daily practice. In fact, these patients are particularly vulnerable to recurrent ischemic event, related or not to the treated coronary lesion, 21,22 and need a close monitoring and optimized pharmacological therapy, including LLT, to minimize their residual risk.
Consistently with previous observations, 18,19,23,24 in our study higher level of education was associated with greater LDL-C goal achievement. Socioeconomic indicators may affect multiple spheres of individual life, including the opportunities of access to health-care facilities and the adherence to long-term therapy. 25 Accordingly, recent data from the Prospective Urban Rural Epidemiologic (PURE) study, which included subjects from 21 high-, middle-, or low-income countries, showed that low education level was the single largest risk factor contributing to death. 26
In this study, we found that patients with hypertension had a lower risk to be off-target. This result is consistent with a previous cross-sectional study on 67,100 patients with coronary artery disease (CAD), showing that hypertension significantly correlated with the achievement of LDL-C goal. 27 Moreover, in a retrospective administrative cohort of patients with CAD or diabetes, the odds to attain the LDL-C value of 100 mg/dL or lower was higher among those with history of hypertension. 28 We hypothesize that patients with hypertension have a higher perceived cardiovascular risk, which might influence the frequency of medical visit, adherence to prescribed drugs and the adoption of behavior education measure. These attitudes and practices might explain the higher probability of these patients achieving the recommended LDL-C goal.
Several factors may influence the achievement of the LDL-C goal such as non-persistence or poor adherence to LLT due to lifestyle, multiple drug assumption, older age and comorbidities. 29 In the EUROASPIRE V, intolerance to statins or patient’s refusal to increase dose were the main reasons for LLT reduction. 18 The majority of patients reduced LLT based on the advice of their physician without any detailed explanation or was unsure of the reason of the change. 18
The EYESHOT post-MI study was not conceived to investigate lipids as primary objective and, thus, the reasons for the undertreatment of LDL-C are not reported. Consistently with previous evidence, one might expect LLT intolerance be involved in a percentage of cases in our study population. A further explanation could be the underestimation of the ASCVD risk by both the patients and the physicians. The EYESHOT post-MI registry focused on patients who experienced MI more than 1 year before. The misperception that, beyond the first year after MI, patients become chronic and stable may favor a detrimental phenomenon of therapeutic inertia, particularly in the elderly and in those with multiple comorbidities, and may have contributed to the substantial undertreatment of patients with LDL-C ≥70 mg/dL.
Statin LLT is the standard of care for lipid management after MI. The PINNACLE registry, designed to evaluate the adherence to guidelines in the management of dyslipidemia, showed a substantial gap in care of CAD patients, who did not receive statin in 28% of cases. 30 In our cohort, however, statins were adopted in the vast majority of cases (93%). Although statin use was significantly higher among those with LDL-C <70 mg/dL, it was reported in 90% of off-targets and, among them, a large proportion (65%) were on high-intensity treatment. The failure to achieve the LDL-C goal in spite of statin LLT, has been previously described. An analysis of the DYSIS (Dyslipidemia International Study), a cross-sectional study focused on statin-treated outpatients throughout 30 countries worldwide, showed the attainment of the LDL-C goal with statins in only one-fifth of cases at very high cardiovascular risk. 31 In this scenario, the marginal prescription of highly effective and well-tolerated LLT drugs, including PCSK9 inhibitors, sheds light on the need for guidelines implementation. Our real-world data advocates a wider use of these agents among patients who experienced MI and who are still off-target despite conventional LLT.
Although perception, knowledge, and adherence with the guidelines have increased, the attainment of the LDL-C goal after MI is still far in most of the patients. To favor the largest LDL-C reduction possible in the highest-risk patients, the latest 2019 edition of ESC guidelines for the management of dyslipidemia have even reduced the LDL-C treatment goal of <55 mg/dL for very-high-risk patients. 13 This might result in a wider discrepancy between the theoretical cut-off and the poor lipid control observed in patients after MI. Data from real-world registries have the potential to improve secondary preventive strategies by raising awareness of physicians and of the whole community on the efforts still needed.
Our results need to be interpreted taking into account the observational and cross-sectional design of the EYESHOT post-MI registry. The absence of patient information over time did not allow to evaluate changes in LDL-C and the achievement of the percentage reduction recommended in very-high risk categories. 13,15
Even if the participating centers were asked to include in the registry all consecutive post-MI patients, we were not able to verify the enrolment process, due to the absence of administrative auditing. However, it is unlikely that selective enrolment in few sites may have substantially changed the study results.
Another limitation of this post-hoc analysis concerns the lack of data about adherence, adverse events and reasons for changes or discontinuation of LLT. Lipid evaluation and treatment were not the primary objective of the EYESHOT post-MI registry, which aimed to investigate the broader secondary preventive strategy in a real-world post-MI setting.
The use of statin intensity groups may have affected the granularity of data and the possibility to capture minor dosage modification within the same statin intensity category. Also, the definitions adopted for LLT changes from baseline to the end of the visit/discharge did not account for the type of non-statin agent added or discontinued. However, these assumptions were required for the analysis and the understanding of the results.
Conclusions
In patients presenting to cardiologists 1 to 3 years from the last MI event, LDL-C levels are suboptimal in a large proportion of patients, particularly in those with a low education level, which might have influenced the frequency of medical visit, drug compliance and the adoption of behavior education measures.
Despite the availability of many effective and well-tolerated statin and non-statin LLT, there is still a substantial underuse of such drugs in patients at very high cardiovascular risk. The failure to reach the LDL-C goal recommended by the guidelines remains a matter of concern in the real world.
Supplemental Material
Supplemental_material_07.06.2020 - Prevalence and Predictors of Out-of-Target LDL Cholesterol 1 to 3 Years After Myocardial Infarction. A Subanalysis From the EYESHOT Post-MI Registry
Supplemental_material_07.06.2020 for Prevalence and Predictors of Out-of-Target LDL Cholesterol 1 to 3 Years After Myocardial Infarction. A Subanalysis From the EYESHOT Post-MI Registry by Angelo Silverio, Rossella Maria Benvenga, Federico Piscione, Michele M. Gulizia, Jennifer M. T. A. Meessen, Furio Colivicchi, Federico Nardi, Cesare Baldi, Gennaro Galasso, Carmine Vecchione, Andrea Di Lenarda, Domenico Gabrielli, Leonardo De Luca and on behalf of the EYESHOT Post-MI Investigators in Journal of Cardiovascular Pharmacology and Therapeutics
Footnotes
Appendix A
Author Contributions
AS, RMB and FP contributed to the conception or design of the work; FP, MMG, JMTAM, FC, FN, ADL, DM and LDL contributed to the acquisition, analysis, or interpretation of data for the work; AS, RMB and LDL drafted the manuscript; FP, MMG, JMTAM, FC, FN, CB, GG, CV, ADL, DG and LDL critically revised the manuscript. All gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy. Angelo Silverio and Rossella Maria Benvenga equally contributed to this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The sponsor of the study was the Heart Care Foundation, a non-profit independent organization, which also owns the database. Database management, quality control of the data and data analyses were under the responsibility of the ANMCO Research Centre Heart Care Foundation. The EYESHOT Post-MI was partially supported by an unrestricted grant by Astra Zeneca, Italy. No compensation was provided to participating sites, investigators, nor members of the Steering Committee. The Steering Committee of the study had full access to all of the data in this study and takes complete responsibility for the integrity of the data and the accuracy of the data analysis.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.