
Abstract
Background:
The benefit of cytochrome P450 (CYP450) enzyme system metabolized medications, especially clopidogrel, was reported more pronounced in smoking than nonsmoking patients, but limited evidence was available from Asian patients. We analyzed data from a large registry-based study of Chinese patients with acute myocardial infarction (AMI) to understand if the above finding could be reproduced.
Methods:
A total of 14 658 patients with AMI were prospectively recruited from 101 hospitals across China. Generalized estimating equation was applied to assess the association between CYP450 enzyme system metabolized medications (clopidogrel, statins, calcium channel blockers) and in-hospital death in smoking and nonsmoking patients, separately, adjusting for hospital clustering effects and propensity score of using the medication in question.
Results:
There were 86%, 93%, and 10% of study patients who received clopidogrel, statins, and calcium channel blockers during the hospitalization. Compared with patients not receiving clopidogrel, patients receiving the drug had a significantly lower risk of in-hospital death (adjusted relative risk [RR] = 0.61, 95% confidence interval [CI]: 0.40-0.91) in current smokers but an insignificant lower risk (adjusted RR = 0.85, 95% CI: 0.71-1.01) in nonsmokers, and the P for interaction was <.01. The corresponding adjusted RR was 0.45 (95% CI: 0.24-0.86) in current smokers and 0.94 (95% CI: 0.68-1.29) in nonsmokers (P for interaction <.01) for statins use and 1.00 (95% CI: 0.53-1.89) in current smokers and 0.66 (95% CI: 0.48-0.90) in nonsmokers (P for interaction = .23) for calcium channel blockers use.
Conclusions:
Our study in a large cohort of Chinese patients with AMI found that the treatment effect in reducing risk of in-hospital death was significantly larger in smokers than in nonsmokers as for clopidogrel and statins but not for calcium channel blockers.
Introduction
Acute myocardial infarction (AMI) is a highly life-threatening condition and a major contributor to global mortality. 1,2 With substantial evidences from large-scale randomized trials, guidelines worldwide advocate the use of evidence-based medications including clopidogrel, statins, and calcium channel blockers for patients with AMI either in or after the acute phase, unless there are contraindications. 3,4 These 3 medications usually require oxidization by cytochrome P450 (CYP450) enzymes to be transformed into their active metabolites. 5,6 Genetic and environmental influences on CYP450 enzymes activity are thought to underlie the substantial interpatient variability in response to these medications. 7,8
Interestingly, smoking patients with AMI showed greater effectiveness of clopidogrel in inhibiting platelet aggregation and lowering adverse clinical outcomes than nonsmoking patients. 9,10 Such “smoker’s paradox” was revealed by post hoc analyses of randomized trials and meta-analysis mostly among patients in North America and Europe. 11 The proportion of Asian ancestry was less than 5% in the Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management and Avoidance (CHARISMA), and the Clopidogrel versus Aspirin in Patients at Risk of Ischemic Events (CAPRIE) studies 12,13 and was not reported in other relevant studies in which the reported proportion of nonwhite population was generally less than 23%. 14 -16 Considering the heterogeneity of genetic characteristics, the smoker’s paradox needs to be investigated in Asian patients. Further, the smoker’s paradox has rarely been studied for statins and calcium channel blockers, although they are also metabolized through CYP450 enzyme system.
The purpose of the present study was to confirm whether the smoker’s paradox reported among patients in North America and Europe could be reproduced among Chinese patients with AMI and whether the phenomenon found for clopidogrel would be reproduced for statins and calcium channel blockers. The knowledge gained from this study could help to improve understanding of the clinical effectiveness of these medications and their pharmacological mechanisms.
Methods and Materials
Data Source and Study Population
Data used for the present study were drawn from the Clinical Pathways for Acute Coronary Syndromes–Phase 3 (CPACS-3) Study (ClinicalTrials.gov identification: NCT01398228). 17,18 Briefly, CPACS-3 study was a stepped-wedge cluster randomized trial that sought to evaluate the effect of a quality of care improvement intervention in reducing the risk of in-hospital major cardiovascular events among patients with acute coronary syndrome (ACS). A total of 101 rural, non-PCI regional county hospitals across China were randomized into 4 wedges with stratification by province. No intervention was applied in the first 6-month cycle in all participating hospitals. And the intervention commenced in one of the 4 wedges in every 6 months afterward. All hospitals received the intervention in the last 6-month cycle. The intervention included establishing a quality of care improvement (QCI) team, training clinical staff, implementing ACS clinical pathways, sequential site performance assessment and feedback, online technical support, and patient education. The details in the study design and patient selection have been reported previously. 17 Adult patients (aged ≥18 years) with a final diagnosis of ACS identified at the time of death or discharge were prospectively included. Patients were excluded if they were dead on arrival or died within 10 minutes after arriving at hospital. In our analysis, patients were further excluded for missing information of smoking status.
A total of 29 346 consecutive patients with ACS were recruited between October 2011 and December 2014. In the present study, we restricted the analyses to patients with AMI. Of the 14 997 patients with AMI, 339 patients were excluded for missing information of smoking status. Therefore, a total of 14 658 patients were included in the final analyses.
Data Collection
Data of each patient were collected from medical chart and from patient interview before hospital discharge. Centrally trained and certified research personnel entered all these data into the dedicated web-based CPACS-3 Data Management System. Data quality was maintained through on-site and online monitoring activities. The collected information included sociodemographic characteristics, disease histories, cardiovascular risk factors, vital signs at hospital admission, treatment during hospitalization, diagnosis at discharge, event of in-hospital death, in addition to smoking status. Details of these variables are shown in Table 1. To ensure the data completeness and accuracy, the information of smoking status was collected through a face-to-face interview with patients.
Baseline Characteristics of Patients With AMI Grouped by In-Hospital Use of Clopidogrel, Statins, and Calcium Channel Blockers.
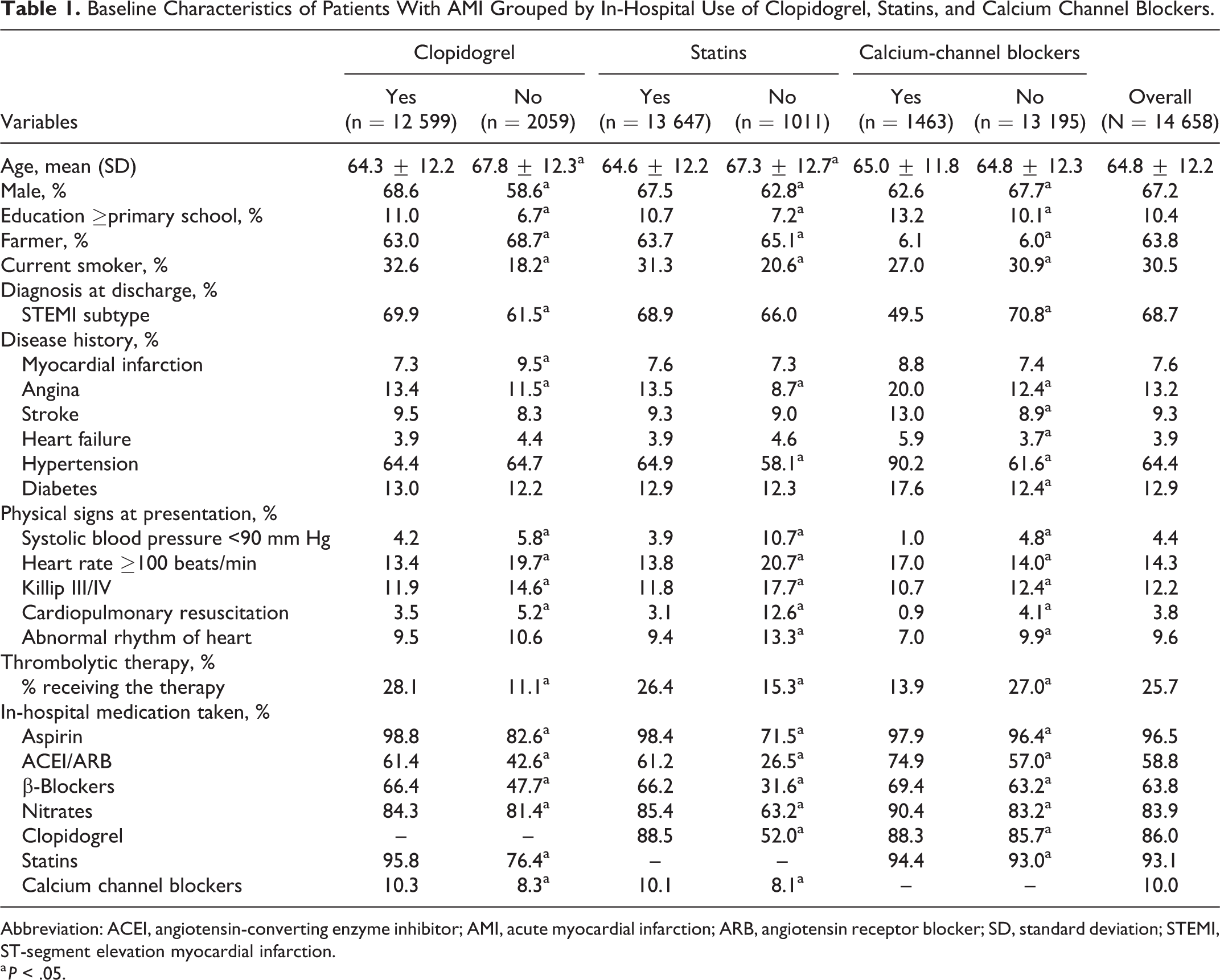
Abbreviation: ACEI, angiotensin-converting enzyme inhibitor; AMI, acute myocardial infarction; ARB, angiotensin receptor blocker; SD, standard deviation; STEMI, ST-segment elevation myocardial infarction.
a P < .05.
Definitions
Current smokers were defined as smoking at least 1 cigarette per day at enrollment. Nonsmokers included former smokers and never smokers. Hypertension was defined according to medical history of hypertension, antihypertension medication use, or measured systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg when presenting at the hospital. Abnormal rhythm of heart was defined as ventricular tachycardia, ventricular fibrillation, or atrial fibrillation detected from continuous electrocardiogram monitoring within 24 hours after admission.
The primary outcome was in-hospital all-cause death. All death events were adjudicated by an independent committee blinded to the patients’ randomization status.
Statistical Analysis
For descriptive purpose, clinical characteristics were described as percentage for categorical variables and mean with standard deviation for continuous variables. Comparison was done by Pearson χ2 or t tests between patients with and without CYP450 enzyme system metabolized medications (clopidogrel, statins, calcium channel blockers) prescribed.
In this study, we tested the treatment effect of CYP450 metabolized medications (clopidogrel, statins, calcium channel blockers) in smoking and nonsmoking patients separately. Then we further tested the disparity in the treatment effect of these 3 medications between smoking and nonsmoking patients by including the interaction term of the medication in question by smoking status in models.
We used generalized estimating equations (LINK = log DIST = Poisson) with an exchangeable working correlation structure to adjust for the hospital clustering effect. Because of the nature of the observational study, we further adjusted for the propensity score of using the CYP450 metabolized medication in question. For propensity score calculation, we fit a multivariable logistic regression model with the use of the CYP450 metabolized medication in question as the dependent variable and baseline characteristics listed in Table 1 as the independent variables (enter method). In calculation of the propensity score for one of the 3 CYP450 metabolized medications, the other 2 medications were also included in the model as independent variables. We conducted both unadjusted and propensity score-adjusted analyses accounting for the clustering effect of hospital. We used the propensity score regression rather than propensity score matching in our analyses so that all study participants could be included to ensure a larger statistical power. The effects were summarized as the relative risk (RR) and 95% confidence interval (95% CI). In addition, goodness-of-fit statistics were calculated for generalized estimating equations models.
In addition to revealing the possible disparity in treatment effect of the CYP450 metabolized medications between smoking and nonsmoking patient, we also analyzed the possible disparity in increasing the risk of major bleedings (adverse effect) with the same strategy and methods.
Statistical analyses were done using SAS version 9.4 (SAS Inc, Cary, North Carolina). All analyses were 2 sided, with a P value less than .05 as statistical significance.
Ethics Approval
Ethics approval for CPACS-3 study was obtained from the institutional review board of Peking University. All participants provided written informed consents. Patients’ data in the Data Management System are protected by password and only de-identified data are available to designated users with appropriate authorization level.
Results
Clinical Characteristics of Study Patients
Table 1 presents demographics and clinical characteristics of study patients. The study patients were predominantly males (67.2%), and the mean age was 64.8 years. Among 14 658 patients with AMI, majority of patients received clopidogrel (86.0%) and statins (93.1%), while only 10.0% of patients received calcium channel blockers. In addition, the proportion of current smokers was 30.5%.
Effectiveness of CYP450 Metabolized Medications by Smoking Status
Table 2 showed the crude rates and RRs of in-hospital death by use of CYP450 metabolized medications in smoking and nonsmoking patients separately. Both for smoking patients and for nonsmoking patients, use of each of the 3 medications was associated with reduced likelihood of in-hospital death. The unadjusted RRs were statistically significant except for calcium channel blockers in smoking patients.
Rates and RRs of In-Hospital Death for Each of the 3 Cytochrome P450 Enzyme Metabolized Medications Among Current Smokers and Nonsmokers.

Abbreviations: CI, confidence interval; RR, relative risk.
After adjustment for the propensity score and clustering effect, clopidogrel use was significantly associated with a reduced risk of in-hospital death only among smoking patients (RR = 0.61, 95% CI: 0.40-0.91, P = .02) but not among nonsmoking patients (RR = 0.85, 95% CI: 0.71-1.01, P = .07). The interaction between smoking status and clopidogrel was significant (P for interaction <.01; Figure 1).

Multivariable- and cluster-adjusted RRs of in-hospital death by smoking status for each of the 3 cytochrome P450 enzyme metabolized medications. CI indicates confidence interval; RR, relative risk.
Similarly, statins use was significantly associated with a reduced risk of in-hospital death only among smoking patients (RR = 0.45, 95% CI: 0.24-0.86, P = .02) but not among nonsmoking patients (RR = 0.94, 95% CI: 0.68-1.29, P = .69). The interaction between smoking status and statins was significant (P for interaction <.01).
For calcium channel blockers, there was no significant difference between smokers and nonsmokers in the treatment effect of reducing in-hospital death (P for interaction = .23). The goodness-of-fit statistics of the fitted generalized estimating equations models are showed in Supplementary Table 1.
Risk of Severe Bleeding and Smoking Status
The adjusted RRs of clopidogrel in increasing the risk of major bleeding were 0.69 (95% CI: 0.39-1.23), 0.44 (0.13-1.52), and 0.83 (0.46-1.49) among overall, smoking, and nonsmoking patients, respectively. Further, clopidogrel use was positively associated with an increasing risk of developing hemorrhagic stroke in smoking patients (0.12% vs 0.00%, respectively; Table 3).
Bleedings (%) by Clopidogrel Use and RRs (95% CI) Among Patients With AMI.
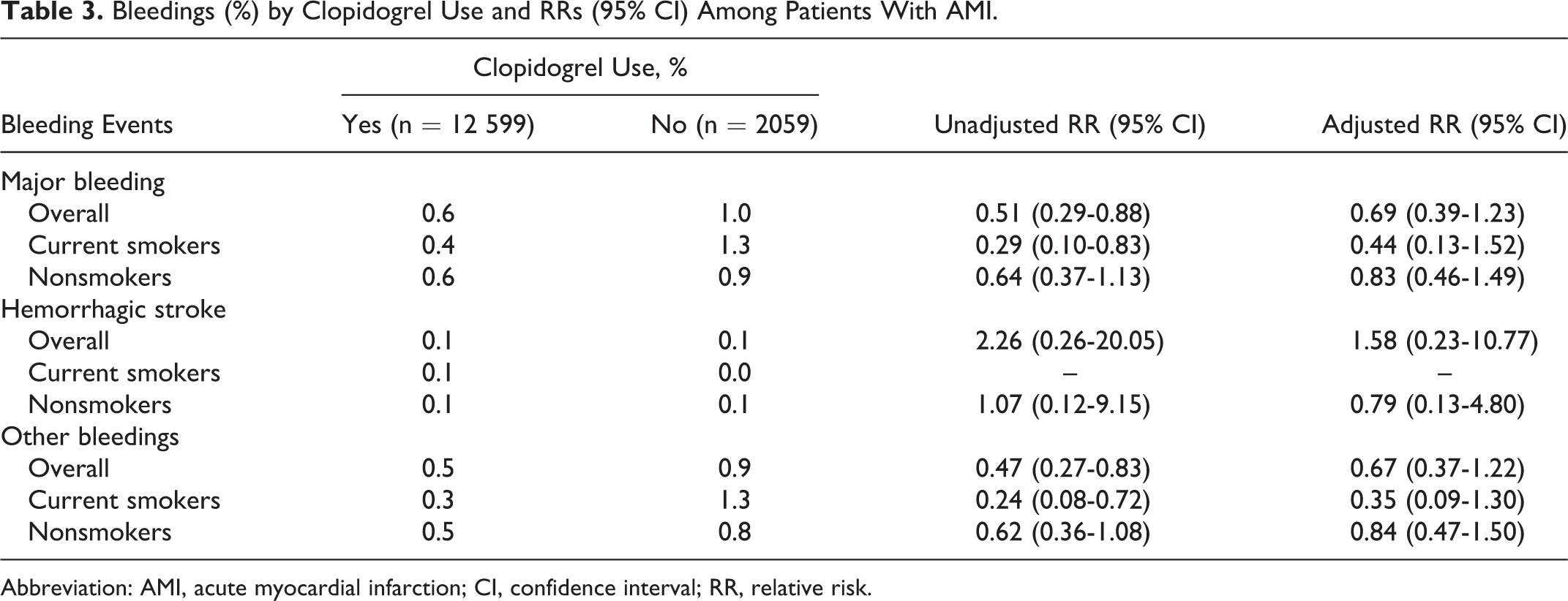
Abbreviation: AMI, acute myocardial infarction; CI, confidence interval; RR, relative risk.
Discussion
Our study using data from a large registry-based study in China confirmed the previous findings that the effectiveness of clopidogrel in reducing the risk of in-hospital death was significantly larger in smoking patients than that in nonsmoking patients with AMI. To our best knowledge, this is the first study revealing the modification effect of smoking status on the effectiveness of clopidogrel in lowering the risk of in-hospital death in a large cohort of Asian patients. Our findings were in concordance with a recently published meta-analysis, which included 7 post hoc analyses of randomized controlled trials among mainly non-Asian populations. 11 The meta-analysis reported that smoking status positively modified the clinical efficacy and pharmacodynamic effects of clopidogrel. 11 Nevertheless, some other studies demonstrated no interaction between smoking status and clopidogrel’s effect in inhibiting platelet aggregation. 19,20
Statins and calcium channel blockers are also widely used in routine care of patients with AMI, both of which are metabolized through CYP450 enzyme system like clopidogrel. Thus, we also analyzed the possible smoker’s paradox for statins and calcium channel blockers in our study. 21,22 Ninety-two percent of our study patients used atorvastatin, simvastatin, lovastatin, or fluvastatin, all of which are metabolized through CYP450 enzyme system. Similarly, CYP450 enzymes metabolized calcium channel blockers including nifedipine, diltiazem, amlodipine, and so on, which accounted for 94% of calcium channel blockers users in our study. Thus, our conclusion might not be influenced by the few statins and calcium channel blockers that are not metabolized through CYP450 enzyme system.
Previous studies suggested several possible explanations for the smoker’s paradox. Some researcher suggested that the greater inhibition of platelet aggregation by clopidogrel in smoking patients might because cigarettes is a potent inducer of CYP450 1A2 and therefore potentially capable of affecting the pharmacokinetics and pharmacodynamics of clopidogrel. 23,24 Some other studies suggested that this smoker’s paradox was probably because smoking patients tended to be younger and healthier than nonsmoking patients. 25 In our study, smoking patients were indeed younger and had less history of cardiovascular diseases but presented with more ST-segment elevation myocardial infarction subtype (see Supplementary Table 2). After adjustment for age, gender, disease histories, cardiovascular risk factors, physical signs at presentation, and treatments, the smoker’s paradox still existed. Thus, the main explanation for the smoker’s paradox might come from other aspects, for example, the heterogeneity in genetic backgrounds between smokers and nonsmokers.
The positive findings for clopidogrel and statins but negative findings for calcium channel blockers seemed contradictory to each other, and if true it would raise a question on whether the 3 medications are really metabolized through the same CYP450 enzyme system. In the treatment of patients with AMI, clopidogrel and statins were often used together. To minimize the chance that the interaction between smoking status and statins is a reflection of the interaction between smoking status and clopidogrel, we calculated the propensity score of the use of one of the 3 medications (eg, clopidogrel), with the other 2 medications (eg, statins, calcium channel blockers) included in the logistic model. The same adjustment was done in analyzing the effectiveness of statins and calcium channel blockers. Thus, there might be less possibility that the smoker’s paradox of statins was actually a mirror reflection of that for clopidogrel, or vice versa.
The interpretation of our results required caution due to the following limitations. First, our study was an observational study and we could not account for unmeasured and unknown confounders. However, the C-statistics shown in the multivariable- and cluster-adjusted models indicated that residual confounding from the unknown variables was small. Second, the information of smoking status was self-report. However, we used face-to-face interview to obtain the information, and the proportion of smoking status in our study is comparable with the data from 2013-2014 nationally representative China Chronic Disease and Risk Factor Surveillance survey. 26 Thus, we believed the information of smoking status in our study was accurate. Third, we did not further stratify nonsmokers to former and never smokers because limited patients reported themselves as former smokers. Thus, we could not answer the question on whether the smoker’s paradox existed for former smokers or not. Fourth, propensity score regression method was used in our analyses in order to make full use of all patients’ information. The propensity score was mostly well balanced except the 10% of patients with the highest propensity score (Supplementary Tables 3-5).
If this smoker’s paradox phenomenon could be confirmed true and future studies could reveal the reason, the new mechanisms that lead to better treatment effects in smoking patients may help to develop more efficient treatment strategies, as well as better understanding of the disease and the causal risk factor. Given the risks of cigarette smoking and the benefits of using the study medications following an AMI, the main implications of our findings are a need for greater awareness of this issue among clinicians and researchers. Our findings indicate that the cytochrome CYP450 pathway mechanism deserves more researches to understand why the smoker’s paradox could happen. Because those understandings will help us to develop novel strategies that might help nonsmokers to enhance the effectiveness of CYP450 metabolized medications, and even development of novel medications that do not use the CYP450 pathway but function better than medications using the pathway.
Conclusion
Our study found that use of clopidogrel and statins but not calcium channel blockers was significantly associated with a reduced risk of in-hospital death in smoking patients than that in nonsmoking patients with AMI. Our findings advocated future studies to be conducted in order to deeply understand the mechanisms behind the phenomenon.
Supplemental Material
Supplemental Material, Revised_Supplementary - Influences of Smoking Status on Effectiveness of Cytochrome P450 Enzyme System Metabolized Medications in Reducing In-Hospital Death in 14 658 Patients With Acute Myocardial Infarction: Data From CPACS-3 Study
Supplemental Material, Revised_Supplementary for Influences of Smoking Status on Effectiveness of Cytochrome P450 Enzyme System Metabolized Medications in Reducing In-Hospital Death in 14 658 Patients With Acute Myocardial Infarction: Data From CPACS-3 Study by Min Li, Lin Feng, Xian Li, Runlin Gao and Yangfeng Wu in Journal of Cardiovascular Pharmacology and Therapeutics
Supplemental Material
Supplemental Material, STROBE_checklist_cohort - Influences of Smoking Status on Effectiveness of Cytochrome P450 Enzyme System Metabolized Medications in Reducing In-Hospital Death in 14 658 Patients With Acute Myocardial Infarction: Data From CPACS-3 Study
Supplemental Material, STROBE_checklist_cohort for Influences of Smoking Status on Effectiveness of Cytochrome P450 Enzyme System Metabolized Medications in Reducing In-Hospital Death in 14 658 Patients With Acute Myocardial Infarction: Data From CPACS-3 Study by Min Li, Lin Feng, Xian Li, Runlin Gao and Yangfeng Wu in Journal of Cardiovascular Pharmacology and Therapeutics
Footnotes
Acknowledgments
The authors thank all patients participating in the CPACS-3 Study and all study hospitals who made efforts to collect and contribute the data for analyses.
Author Contributions
Yangfeng Wu conceived the study design. Min Li analyzed the data and drafted the manuscript. Lin Feng verified the statistical analyses. Yangfeng Wu, Xian Li, and Runlin Gao participated in the interpretation of results and commented on the manuscript. All authors contributed to the revision and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Sanofi, China. The sponsor of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The principal investigators had full access to all data in the study and final responsibility for the decision to submit for publications.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.