
Abstract
Objective:
To assess heart failure (HF) knowledge, adherence to lifestyle recommendations, and quality of life (QOL) among Koreans with HF and identify factors influencing QOL.
Methods:
A cross-sectional and correlational design was used and a total of 142 Koreans with HF were recruited between April 2012 and September 2013. Data were analyzed using multiple logistic regression with SPSS version 21.0.
Results:
The mean age of participants was 64.1 ± 7.4 years. A higher proportion of participants were male, married, unemployed, had a high education level, and class I New York Heart Association (NYHA) functional status. A higher proportion of participants had ≥2 comorbidities and the most prevalent comorbidity was diabetes. The mean score of HF knowledge was 6.9 (possible range 0-15) and the most frequent incorrect items were “proper actions to reduce thirst” and “causes of leg swelling” in both better and worse QOL groups. Among the recommended lifestyle, pneumococcal vaccination had the least adherence in both groups. Multiple logistic regression showed that patients in NYHA class I, with a higher left ventricular ejection fraction, who had knowledge of “amount of fluid intake a day” and consumed more than moderate alcohol tended to have better QOL.
Introduction
The number of patients with heart failure (HF) has increased worldwide 1 and the prevalence of HF increased by 13.2% from 116 000 in 2014 to 132 000 in 2018, resulting in nearly doubled medical costs over 4 years in South Korea. 2 The treatment of HF has advanced over the past decade, and the health-care focus for patients with HF has changed from acute to chronic, with an increased emphasis on promoting a healthy lifestyle and alleviating symptoms. 3 Patients with HF experience many typical HF symptoms such as dyspnea, fatigue, and reduced exercise tolerance. 4 According to large studies conducted in Europe, patients with HF have deteriorated quality of life (QOL), compared to patients with other chronic conditions such as chronic obstructive pulmonary disease or cancer. 5 Lower levels of QOL are associated with limited mobility, high prevalence of pain/discomfort and anxiety/depression, 5 HF exacerbation, and hospitalization or death. 6 In patients with HF, adherence to lifestyle recommendations was low. In particular, the lowest adherence rate was noted for the exercise of 10.0% to 14.8%. 7,8
Lifestyle recommendations include low sodium diet, regular exercise, smoking cessation, alcohol restriction, and vaccination. Healthy lifestyle habits reduce the severity of chronic diseases 9 and promote patients’ control over their daily activities and QOL. 10 Smoking is a significant predictor of HF symptom aggravation, 11 and alcohol has cardiotoxic effects in patients with HF. 12 Influenza and pneumococcal vaccinations can prevent morbidity and mortality and improve QOL in patients with HF. 13 To improve the QOL among patients with HF, guidelines emphasize the importance of HF knowledge in addition to healthy lifestyle. 4 However, among these patients, HF knowledge remains low. 14 -16 Recent investigations have found that only 18.7% to 46.3% of patients with HF possessed a suitable understanding of HF, disease treatment, and symptom awareness. 15,16 In particular, only 34.6% of respondents correctly identified the “recommended frequency of weight monitoring,” and only 30.3% knew the “cause of rapidly worsening symptoms of heart failure.” 14 Several studies found that higher levels of HF knowledge were related to better adherence to a healthy lifestyle and higher levels of QOL. 14,15 Through a literature review, we found that understanding of certain domains of HF knowledge and adherence to healthy lifestyle habits were particularly low. These deficiencies could adversely affect QOL in these patients. However, there is little information on which specific HF knowledge or lifestyle influences QOL.
We aimed to explore the relationship between each component of HF knowledge and lifestyle and QOL among patients with HF. An inability to understand how each component of HF knowledge and lifestyle affects QOL may hinder effective tailoring of interventions to improve QOL. For focused tailoring of interventions for patients with HF, this study assessed which lifestyle serve more importantly to improve or deteriorate QOL. It is important to understand how well Korean patients with HF understand their disease and perform recommended lifestyle and to explore the factors associated with QOL. Therefore, the primary aim of this study was to assess which components of HF knowledge and lifestyle most affect QOL. We hypothesized that specific component of HF knowledge and lifestyle would be highly associated with QOL.
Methods
Study Design
This study adopted a cross-sectional, descriptive, and correlational design to examine HF knowledge, adherence to lifestyle recommendations, and QOL and determine the factors that predict QOL among community dwellers with HF living in Korea.
Participants
The target population in this study consisted of community dwellers with HF living in Korea. To represent a target population, patients were recruited from outpatient clinics to form a heterogenous study cohort. The patients were recruited from university and community hospitals in the southern region of Korea between April 25, 2012 and September 26, 2013. The inclusion criteria were aged 50 to 80 years, diagnosis of HF with left ventricular ejection fraction (LVEF) of ≤45%, able to walk independently with or without assistive walking devices, such as a cane, able to communicate without hearing difficulties or cognitive problems, and speaking Korean. The exclusion criteria were hospitalization due to HF exacerbation within 3 months. The sample size was calculated using G*Power version 3.1 program 17 for multiple regression analysis. A sample of 114 participants was required to reach a power of β = 0.80, with an α-error probability of <.05 based on the 9 independent variables and a medium effect size (f2 = 0.15). A total of 142 patients were included in the analysis.
Data Collection
The protocol of the present study was approved by the institutional review boards of each site (nos. 05-2012-014, D-1205-003-001, and 2013-04-018-001) before data collection. Eligible patients were referred to the researchers by health-care providers in the clinics. Eligible participants received a detailed explanation regarding the study from a trained research assistant and signed written informed consent. The participants completed the questionnaire and provided their demographic information. Trained research assistants reviewed medical records to obtain clinical information such as New York Heart Association (NYHA) class, LVEF, comorbid conditions including diabetes, hypertension, myocardial infarction, and arrhythmia.
Measures
Heart failure knowledge
Heart failure knowledge was assessed using the Dutch HF knowledge scale. 18 The instrument was first translated into Korean by 2 researchers on the research team. A back-translation was carried out by 2 bilingual experts with no prior exposure to the questionnaire. Differences in the translations were discussed, the agreement was reached on the final version, and content validity was assured by researchers. Dutch HF knowledge scale consisted of 15 items with multiple-choice options covering general knowledge of HF, disease treatment, and symptom recognition. One point was given if patients chose the correct response among 3 options. The total score ranged from 0 to 15, with higher scores indicating better knowledge. Internal consistency of this instrument was assessed in patients with HF, and Cronbach α in this population was 0.62. 18 Construct validity was assessed using a known-groups technique. The instrument was able to distinguish between 2 groups of patients who should—theoretically—produce different scores on the instrument (t = −7.14, P < .001). 18
Recommended lifestyle
The recommended lifestyles assessed in this study included ≤3 g sodium restriction, regular exercise, smoking cessation, alcohol consumption, and pneumococcal and influenza vaccination status based on the recommendations of the HF Society of America. 19
Daily sodium intake
The Dish Frequency Questionnaire-70 (DFQ-70) developed by Korean researchers was used to estimate daily sodium intake. 20 The DFQ-70 consists of a total of 70 food items that Koreans frequently consume, such as kimchi, noodle, and stew. Participants were asked to recall how often they consumed each food item listed on the DFQ-70 with its usual portion size. This information (frequency and actually consumed serving size) was used as a weight and multiplied with the amount of sodium in each food per serving to compute daily sodium intake. When the estimated sodium intake based on the DFQ-70 was compared with the 24-hour-sodium excretion, there was a 3% difference between the 2. 20
Regular exercise
Participants were asked whether they regularly engaged in exercise. Participants who responded to engaging regularly in exercise were asked to further describe the types of exercise, frequency, and duration. Based on this information, metabolic equivalent of task (MET) scores, defined as the amount of oxygen consumed during rest for 1 minute, were computed. 21 The HF Society of America recommends walking for 30 minutes per day for 5 days in a week, which corresponds with 495 MET-min/week. 19 We used 495 MET-min/week as the cutoff to define an adequate level of exercise. Participants were grouped into 2: the inactive to the minimum exercise group (<495 MET-min/week) and adequate exercise group (≥495 MET-min/week).
Smoking, alcohol consumption, and pneumococcal and influenza vaccination
Participants were asked about their smoking status (current smoker or non-smoker), alcohol consumption patterns (type of alcoholic beverage, amounts, and frequency), and pneumococcal and influenza vaccination statuses. Moderate alcohol consumption was defined as ≥1 glass of alcoholic beverages for females or ≥2 glasses for males.
Quality of life
Quality of life was assessed using the Minnesota Living with Heart Failure Questionnaire (MLHFQ). The instrument was first translated into Korean by 2 researchers on the research team, back-translated by 2 bilingual experts, and content-validated by the research team. This self-administered questionnaire consists of 21 questions covering physical, psychological, and socioeconomic aspects of life, relative to the burdens associated with HF. 22 The items are rated on a 6-point Likert scale from 0 (no) to 5 (very much burdensome). The total score is the sum of the responses from each item and can range from 0 to 105. Higher scores reflect worse QOL. The total scores had good reliability as indicated by a Cronbach α = 0.94. 23
Demographic and clinical characteristics
Data regarding demographic characteristics (eg, age, gender, marital status, employment status, and level of education) and clinical characteristics (eg, NYHA class, LVEF, diagnosis duration, and comorbid conditions) were collected via patient interview and review of the medical records.
Data Analysis
Descriptive statistics including frequencies, percentages, means, and standard deviations were used to present participants’ demographic and clinical characteristics, HF knowledge, adherence to lifestyle recommendations, and QOL. The participants were categorized into 2 groups using the median scores of QOL of this study. To identify factors that influenced the participant’s QOL group (better or worse), univariate analysis was performed using the t test and χ2 test. Multiple logistic regression analysis was performed to evaluate the influence of demographic and clinical characteristics, HF knowledge, and adherence to recommended lifestyle. The level of QOL (better vs worse) was entered as a dependent variable and variables with P < .05 in the univariate analysis were entered as independent variables. In the models, a backward elimination of insignificant variables was used. Then, odds ratios (ORs), associated 95% confidence intervals (CIs), and P values were computed. Statistical analyses were performed using IBM SPSS software, version 20.1 (IBM Corp., Armonk, New York). Analysis items with P < .05 were considered statistically significant.
Results
Characteristics of the Participants
The mean age of 142 participants was 64.1 ± 7.4 years. Most of the participants were male, had a spouse, were unemployed, had an education level of high school or above, had NYHA class I, and had less than 3 years duration of diagnosis. The mean LVEF was 34.3%, more than half of the patients had 2 or more comorbidities, and approximately one-fourth of them had diabetes or hypertension (Table 1).
Demographic and Clinical Characteristics According to QOL.a
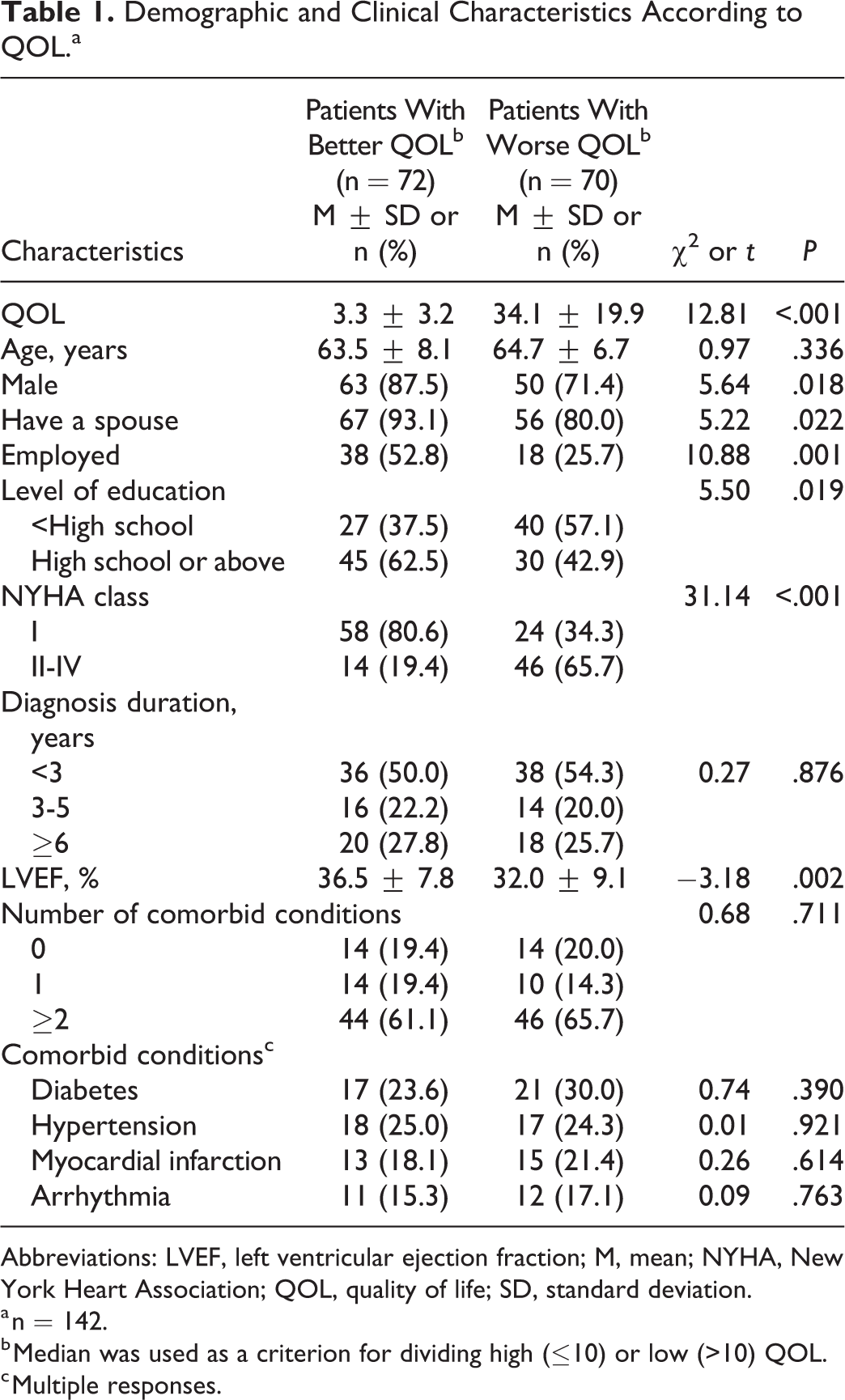
Abbreviations: LVEF, left ventricular ejection fraction; M, mean; NYHA, New York Heart Association; QOL, quality of life; SD, standard deviation.
a n = 142.
b Median was used as a criterion for dividing high (≤10) or low (>10) QOL.
c Multiple responses.
The average score of the Dutch HF knowledge scale for the entire142 participants was 6.9 ± 2.1. Three items that were most frequently responded to correctly in both better and worse QOL groups were “medication treatment” (86.1% and 87.1%, respectively), “exercise” (86.1% and 82.9%, respectively), and “action to worsening symptoms” (81.9% and 72.9%, respectively). Three items that were most frequently responded to incorrectly were “cause of rapidly worsening symptoms of HF” (6.9%), “causes of leg swelling” (13.9%), and “action to reduce thirst” (18.1%) in the better QOL group, and “action to reduce thirst” (10.0%), “recommended frequency of weight monitoring” (11.4%), and “causes of leg swelling” (21.4%) in the worse QOL group (Table 2).
Heart Failure Knowledge.a
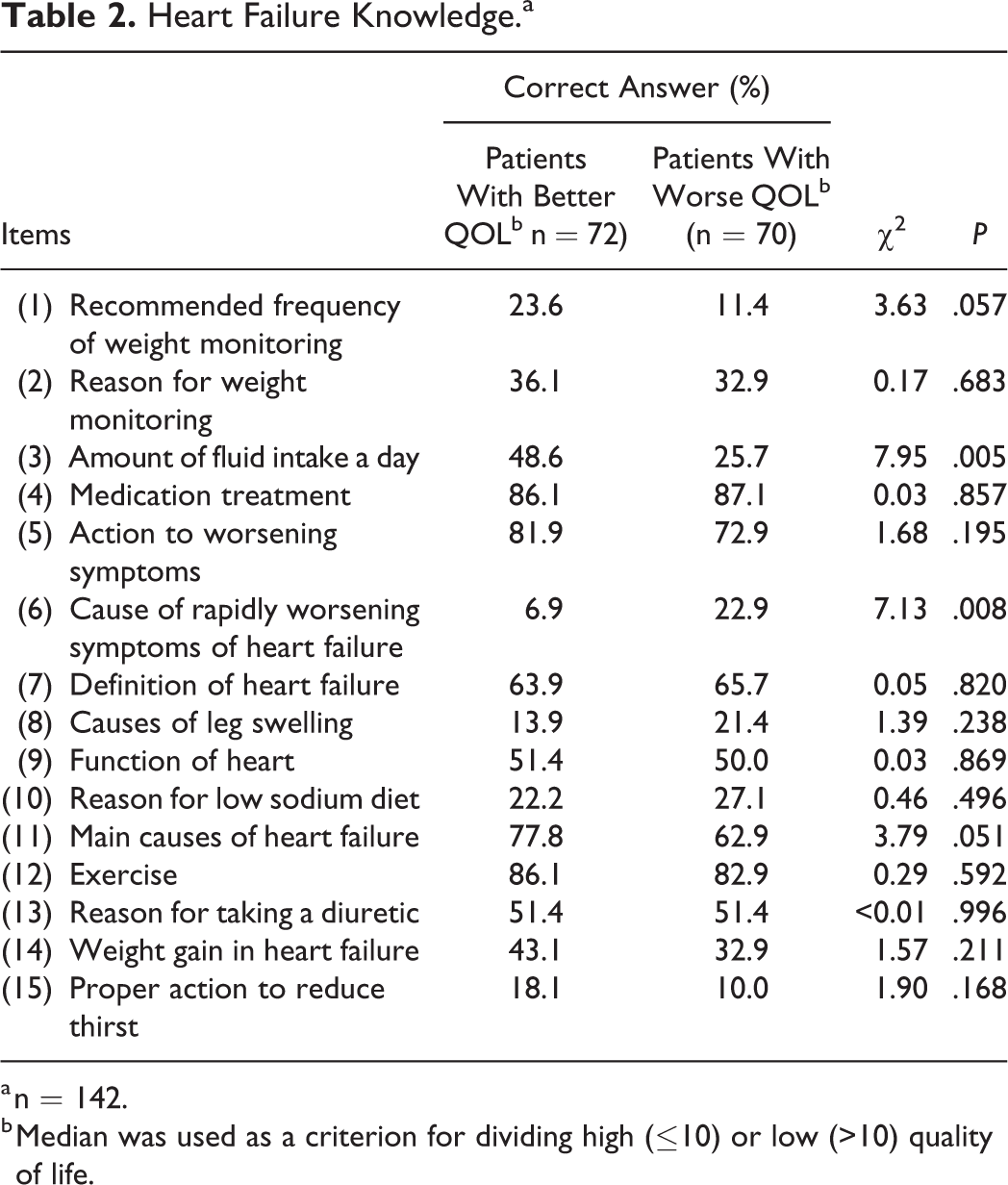
a n = 142.
b Median was used as a criterion for dividing high (≤10) or low (>10) quality of life.
Among the 6 lifestyle recommendations, smoking cessation (84.7%) was the most performed in the better QOL group and moderate alcohol consumption (82.9%) was the most performed in the worse QOL group. Pneumococcal vaccination was the least likely performed in both better and worse QOL groups (11.1% and 8.6%, respectively) followed by adequate sodium intake (≤2 g/d; 25.0% and 31.4%, respectively), regular exercise (38.9% and 40.0%, respectively), and flu vaccinations (48.6% and 52.9%, respectively; Table 3).
Adherence to Recommended Lifestyle.a,b

a Adherence to above lifestyles was defined as sodium intake ≤2 g/d; regular exercise >495 metabolic equivalent of task; no smoking; alcohol consumption of ≤1 glass for females or ≤2 glasses for males; and having annual pneumococcal and flu vaccination.
b n = 142.
c Median was used as a criterion for dividing high (≤10) or low (>10) quality of life.
The average score of the MLHFQ for the entire 142 patients was 18.5 ± 21.0 and the median score was 10.0. Based on the median scores on the MLHFQ, we grouped the participants into better (≤10) and worse (>10) QOL reflecting higher MLHFQ scores indicate worse QOL. The average scores of the MLHFQ for the participants with better and worse QOL were 3.3 ± 3.2 and 34.1 ± 19.9, respectively.
Factors Predictive of QOL
Univariate analysis
Univariate analysis showed that gender (P = .018), marital status (P = .022), occupational status (P = .001), level of education (P = .019), NYHA class (P < .001), LVEF (P = .002; Table 1), knowledge of “amount of fluid intake a day” (P = .005), knowledge of “cause of rapidly worsening symptoms of heart failure” (P = .008; Table 2), and alcohol consumption (P < .001; Table 3) significantly differed between the better and worse QOL groups. The participants with worse QOL were disproportionately female, less likely to have a spouse, more likely to be unemployed, had lower levels of education, exhibited higher NYHA classes, and had lower LVEF than the participants with better QOL. In terms of HF knowledge, the participants with worse QOL had less understanding of the “amount of fluid intake a day” and more knowledge of the “cause of rapidly worsening symptoms of HF” than the participants with better QOL. In terms of adherence to lifestyle recommendations, the participants with worse QOL were more likely to consume moderate amounts of alcohol than the participants with better QOL.
Multiple logistic regression analysis
Table 4 shows the results of the final model using the backward method. The factors included in the final logistic regression model explained 46.6% of the variation in QOL (Nagelkerke R2 = .466, χ2 = 3.57, P < .001). In the classification table, the probability of accurately predicting participants with better and worse QOL was 75.0% and 81.4%, respectively, with 78.2% accuracy in classification of QOL for the regression model. Participants with NYHA class I had an almost 9-fold higher chance of having better QOL than participants with NYHA class II to IV (OR = 8.77, 95% CI: 3.51-21.94, P < .001), and each unit of LVEF increased the chance of having a better QOL by 1.06 times (OR = 1.06, 95% CI: 1.01-1.12, P = .020). Participants who had knowledge of “amount of fluid intake a day” had 3.54 times higher chance of having a better QOL than participants who did not have this knowledge (OR = 3.54, 95% CI: 1.38-9.09, P = .009). Participants who consumed more than moderate alcohol had 4.90 times higher chance of having a better QOL than participants who adhered to moderate alcohol consumption (OR = 4.90, 95% CI: 1.77-13.57, P = .002). That is, it was predicted that participants who had NYHA class I, with a higher LVEF, had knowledge of “amount of fluid intake a day,” and consumed more than moderate alcohol would have a better QOL.
Predictors of QOL Among Heart Failure Patients.a,b
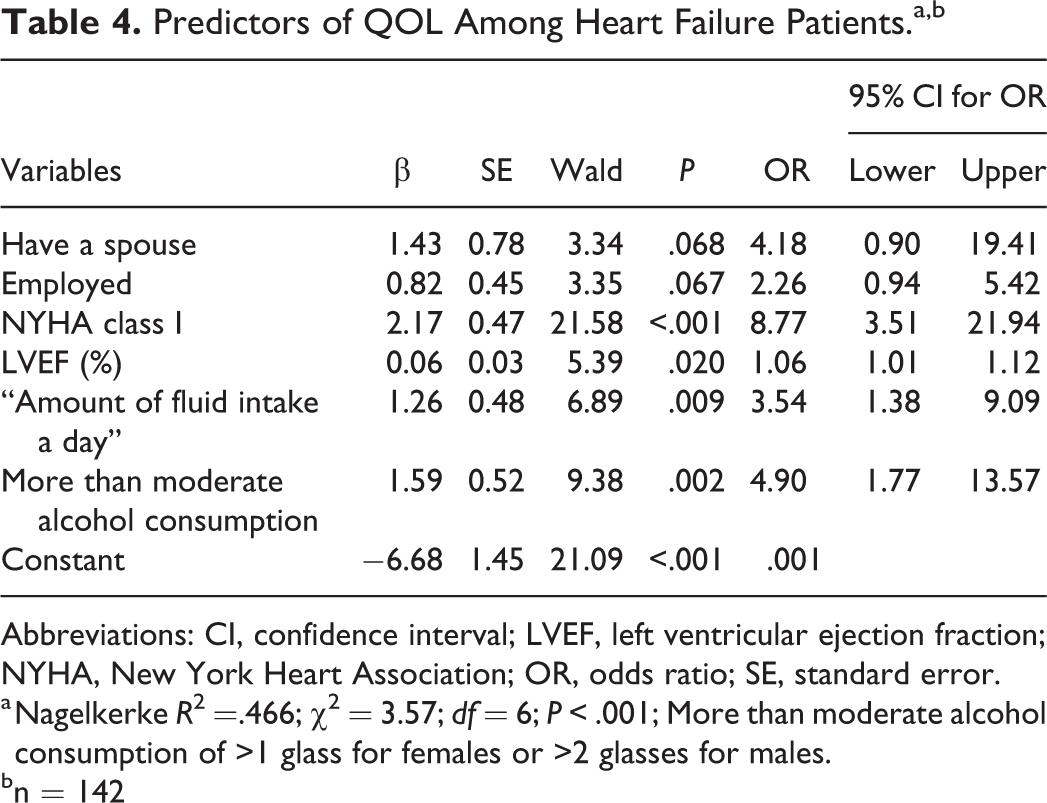
Abbreviations: CI, confidence interval; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association; OR, odds ratio; SE, standard error.
a Nagelkerke R2 =.466; χ2 = 3.57; df = 6; P < .001; More than moderate alcohol consumption of >1 glass for females or >2 glasses for males.
bn = 142
Discussion
Knowledge deficit was a serious problem among the patients in our sample. An average of 7 of 15 items assessing HF knowledge was correctly answered. When compared to the results of previous studies, the mean score of HF knowledge was much lower in our study (mean, 6.9) than in the other studies (mean, 11.3-11.4). 24,25 A lack of comprehensive understanding of HF and its management negatively contributes to adherence to lifestyle recommendations. 25 In our study, 14.8% of the participants knew that HF could be exacerbated by a cold or flu; 49.3% had an annual flu shot. As our sample did not understand that fluid overload contributes to HF symptoms, a majority of them responded “drink a large amount of water in case of feeling thirsty” instead of “sucking on ice chips” and did not restrict their sodium intake. Similarly, most patients reported they drank more when they were thirsty, and only 4% reported using ice chips to decrease their thirst in a study conducted in Sweden, the Netherlands, and Japan. 26 The most frequently reported reasons for thirst were salty or spicy food. This was more frequently reported by Asian, rather than Western, patients. 26 In previous studies, thirst can be distressing 27 and can decrease QOL 28 for patients with HF. Therefore, it is important to educate patients on strategies to decrease thirst. Since our sample had insufficient knowledge of HF, it is hardly expected that they followed a healthy lifestyle recommendation to prevent HF exacerbation.
We explored adherence to 6 lifestyle recommendations among Korean patients with HF. Having pneumococcal vaccination, proper sodium intake, and performing regular exercise were the least performed lifestyle recommendations. This finding was similar to the findings obtained by Tawalbeh and colleagues, 29 who indicated that avoiding getting sick by having a vaccine was one of the least performed lifestyles among patients with HF. It seems that patients with HF have less information about the vaccine and its importance. Health providers need to highlight vaccination to patients with HF to prevent HF exacerbation. Indeed, many patients with HF may be hospitalized for other causes related to influenza virus and bacterial pneumonia. 30 The result regarding proper sodium intake in this study was not consistent with the results of previous studies conducted in Jordan, 29 Japan, 31 and Iran 32 which indicated that asking for a low-salt diet was a frequently performed lifestyle. Further research is needed to examine the cultural limitations that Korean food can have, such as the taste of low-sodium foods, diet preferences, and food preparation styles in Korea.
Among the patients in our sample, 60.6% did not engage in regular exercise based on the recommended activity level by the HF Society of America (walking 30 minutes per day for 5 days per week). The proportion of non-adherence to regular exercise in our sample was slightly higher than that of Japan (53.0%), although our sample had a relatively higher functional status (57.7% in NYHA I) than that obtained in Japan (40.9% in NYHA I). 33 Experience is thought to play a role in the development of expertise in a healthy lifestyle; 34 that is, patients who had insufficient experience in managing symptoms were unable to identify triggers such as dietary indiscretions or overexertion that precede a bout of fluid retention. Patients included in our study had a mean LVEF of 34.3%, which was higher than that of 28.4% to 33.7% 5,35 -37 among patients in other studies, and more than half of the patients in our study had NYHA class I at enrollment. Therefore, it could be suggested that patients in our study rarely had severe symptoms at that time and seemed to overlook the need for a healthy lifestyle. However, HF patients who follow a healthy lifestyle before symptoms escalate are assumed to have better QOL eventually than those with poor adherence to lifestyle recommendations. 35 Thus, health-care providers should focus on teaching HF patients about HF knowledge especially in “recommended frequency of weight monitoring,” “cause of rapidly worsening symptoms of heart failure,” “causes of leg swelling,” and “proper action to reduce thirst” in which patients in our study rarely had knowledge. Health-care providers should assist patients to promote a healthy lifestyle, for example, helping patients see that when they adhere to a low-sodium diet, they retain less fluid, which decreases the likelihood of low QOL in the near future. Considering the lack of educational opportunities under the Korean health-care system 14 and that physicians’ face-to-face time with patients during visits is 3.5 minutes in Korea, 38 nurses who are the main professionals who follow patients with chronic diseases 39 must plan and implement strategies that can improve knowledge and lifestyle in this population in Korea.
We explored which HF knowledge and lifestyle were associated with QOL because this information may guide researchers and clinicians to design educational programs to promote each lifestyle, which will in turn increase QOL. Surprisingly, more than moderate alcohol consumption was associated with better QOL. This finding may be explained by the fact that drinking alcohol is one of the common ways to socialize with peers among Korean adults, especially men. 40 In our sample which comprised predominantly men, abstinence or restriction of alcohol consumption may negatively affect their social relationships with others, which may contribute to impaired QOL. Another possible explanation is the cross-sectional nature of these data, not the causality of the relationship. Patients with worse QOL may exhibit limited socialization due to their severe HF symptoms. Worse QOL may motivate these individuals to pursue healthy lifestyle habits rather than healthy lifestyle habits causing a decline in QOL. These findings suggest that researchers are encouraged to study these relationships over time longitudinally, as the relationships postulated here are merely associative.
Our study has several limitations to note. Although the analysis was performed by specifying the relationships, the dynamics of the relationship are hard to discern with cross-sectional data. Researchers will need to measure the variables over time to make any predictive statements in the future. Participants in this study were recruited from outpatient clinics affiliated to a university and community hospitals in the southern region of Korea; a majority of the patients had NYHA I and were male. Therefore, the generalizability of our results to the HF population and HF management may be limited. Further studies with a larger sample are needed to improve the representativeness of these findings. As we relied on self-reported adherence to lifestyle recommendations, it is possible that participants over-reported their adherence. However, we fully explained the importance of honestly answering questions to study participants to minimize social desirability bias. Even with the limitations mentioned above, this article adds new insight into specific HF knowledge domains and healthy lifestyle habits that most affect QOL. This information is critically important for informing education efforts that focus on patients with HF in clinical practice.
Conclusion
In this study, we found that Korean patients with HF did not have adequate levels of HF knowledge and adherence to lifestyle recommendations yet. Although knowledge does not always translate into engagement, having sufficient knowledge to understand the entire picture of HF and its management is required to improve adherence to recommended lifestyles. Having NYHA class I HF, higher LVEF, knowledge of “amount of fluid intake a day,” and consuming more than moderate amounts of alcohol are significant factors for better QOL among patients with HF.
A prominent aspect of our study was the assessment of specific HF knowledge and healthy lifestyle that determine QOL among patients with HF in Korea. This study found that there is a need for targeted and focused education such as proper actions to reduce thirst, causes of leg swelling, and amount of fluid intake a day. Longitudinal approaches are required to pass the methodological limitations of this study and more active interventions targeting healthy lifestyle such as pneumococcal vaccination are required to improve QOL and clinical outcomes in this population.
Footnotes
Authors’ Note
Institution where the work was done: Pusan National University Hospital, Pusan National University Yangsan Hospital, BHC Hanseo Hospital. Ethics approval and consent to participate.The ethics review boards of Pusan National University Yangan Hospital (05-2012-014), Pusan National University Hospital (D-1205-003-001), and Kyungpook National University Hospital (2013-04-018-001) approved the study protocol, and informed consent was obtained from all participants.
Author Contributions
Haejung, L. contributed to the conception, design of the study, analysis and interpretation of data, and critically revised the manuscript. Gaeun, P. contributed to the analysis and interpretation of data, and drafted the manuscript and critically revised the manuscript. Kyoung Suk, L. contributed to the analysis and interpretation of data, and drafted the manuscript. Hyekyung, J. contributed to the acquisition and analysis of data, and drafted the manuscript. Kook Jin, C. and Jong Hyun, K. contributed to the acquition of data. All authors gave final approval and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a 2-Year Research Grant of Pusan National University.