
Abstract
Background:
Increasing numbers of blood pressure lowering (BPL) agents are being prescribed for both primary and secondary prevention of cardiovascular disease, especially in the older population. The aim of this study is to describe the temporal trends and patterns of BPL dispensing among older Australians (aged ≥65 years).
Methods:
We utilized prescription claims data from the Australian Pharmaceutical Benefits Scheme (PBS) for a 10% random sample of people aged ≥65 years. The PBS, funded by the Federal government, provides subsidies to make medicines more affordable for Australian residents. We restricted our analysis to “long-term concession” individuals, who would use PBS for the majority of their medication needs. BPL agents were identified using the World Health Organization Anatomical Therapeutic Chemical classification codes. The annual prevalences and proportional distributions of BPL dispensing by categories were summarized from 2006 to 2016. Direct standardization was applied to indicate changes of BPL dispensing over time.
Results:
Age-standardized dispensing of BPL agents increased by 8% among older Australians from 2006 to 2016 (58%-66%). BPL dispensing in males has exceeded that in females since 2009. Angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers were the dominant BPL agents dispensed, with more than 55% of all BPL users over time. Dispensing of diuretics decreased from 27% to 21%, calcium channel blockers decreased from 30% to 25%, while β-blockers remained stable (29%-31%). The use of fixed-dose combinations increased over time from 23% to 31%.
Conclusion:
The prevalence of BPL dispensing steadily increased among older Australians from 2006 to 2016. The changes in the patterns of BPL dispensing were largely in line with contemporary changes to clinical guidelines for an aging population.
Background
Cardiovascular disease (CVD) is a major contributor to the burden of disease in Australia, 1 with most of the burden borne by older people. According to the 2015 Australian National Health Survey (NHS), 53% of the 65-74 year-old population and 66% of those aged 75 years and above reported at least one form of CVD. 2 Hypertension, ischemic heart disease, cerebrovascular diseases, and heart failure are the most prevalent forms of CVD. 1
Blood pressure lowering (BPL) agents are widely used for both primary and secondary prevention of CVD. 3 The most commonly dispensed BPL agents are angiotensin-converting enzyme inhibitors (ACEIs)/angiotensin II receptor blockers (ARBs), β-receptor blockers (BBs), calcium channel blockers (CCBs), and (low-dose) diuretics. Different BPL agents are used as first-line treatment for various manifestations of CVD. 4 –6 For example, ACEIs and diuretics are first-line medications for heart failure, 4 and ACEIs and BBs are indicated for ischemic heart disease. 5 According to the 2008 Australian National Heart Foundation guidelines, diuretics together with CCBs and ACEIs were recommended as first-line pharmacotherapy for uncomplicated hypertension, 6 whereas the updated guideline in 2016 weakened the role of diuretics as first-line medications for older adults (≥65 years). 7
The use of fixed-dose combinations (FDC) is now common, especially for the management of CVD and diabetes. 8 The combinations of different categories of BPL agents have a proven additive effect on lowering blood pressure, superior to increasing the dose of a single BPL agent. 9 Evidence also suggests improved adherence to FDC compared to multiple single agents 10 . Furthermore, the use of FDC reduces out-of-pocket costs (dispensing fee) for patients. 8 Since 2000, a variety of FDC of BPL agents have been listed under the national Pharmaceutical Benefits Scheme (PBS), most of which contains either an ACEI or an ARB agent. 11
Since the 1960s, the incidence and mortality of coronary heart disease and stroke have been declining in Australia, especially among the older population. 1 This may be related to the increasing use of preventive medications such as BPL agents and statins. However, there are limited data and evidence of the temporal trends and the patterns of BPL dispensing among older Australians aged 65 years and above. Therefore, in this study, we sought to bridge this gap.
Methods
We utilized national prescription claims data from the Australian PBS provided by the Commonwealth Department of Human Services. These data included medication dispensing records from a 10% randomly selected Australians eligible for PBS from 2006 to 2016. From these data, we obtained information on people’s demographic characteristics (sex, year of birth, and year of death), medication item codes, the quantity of dispensing, and dispensing date. These data were de-identified with unique patient identifiers. For every medicine dispensed under the PBS scheme, patients make out-of-pocket co-payments up to a certain amount, known as the “co-payment threshold.” For example, the co-payment threshold for general patients was $35.4 AUD per script in 2012, whereas the threshold for concessional patients was $5.80 AUD per script in the same year. Since a number of BPL agents were priced below the “co-payment threshold” for general patients, we decided to restrict our analysis to “long-term concession” individuals, 12 whose BPL dispensing was more likely to be consistently captured by the PBS over time.
Eligible individuals in this study were “long-term concession” Australians aged 65 years and above at the time of medication dispensing from 2006 to 2016 inclusive. The subgroup of people with “long-term concession” status comprised about 80% of older Australians. 13 We extracted the dispensing of BPL agents catalogued under the World Health Organization (WHO) Anatomical Therapeutic Chemical (ATC) codes C02 (antihypertensives), C03 (diuretics), C07 (BBs), C08 (CCBs), and C09 (ACEIs/ARBs). We then divided BPL agents into the following sub-categories: low-ceiling diuretics (C03A and C03B), other diuretics (C03C high-ceiling diuretics, C03D potassium-sparing agents, and C03E diuretics and potassium-sparing agents in combination), BBs with an indication for heart failure management (bisoprolol, carvedilol, and nebivolol), other BBs (atenolol, labetalol, metoprolol, oxprenolol, pindolol, and propranolol), dihydropyridine CCBs (C08C), non-dihydropyridine CCBs (C08D), ACEIs/ARBs in singular form (C09A and C09C), and FDC containing ACEIs or ARBs (C09B and C09D).
We estimated the prevalence of BPL dispensing by age and gender, with the denominators being the number of people who had at least one dispensing record of any medication in a given year and the numerators being the number of people who had at least one dispensing of any BPL agent in the same calendar year. The annual standardized prevalence of BPL dispensing was summarized in the target population over the 11-year study period. We applied direct standardization using the 2001 world standard population from the WHO. 14 Multivariable logistic regression models were applied to investigate the temporal trends in BPL dispensing, adjusting for age and sex.
We further described the patterns of BPL dispensing over time. In these analyses, the numbers of older adults with BPL dispensing were used as denominators and the number of people with specific categories or sub-categories of BPL dispensing as numerators. We also summarized the proportion of BPL users by the number of categories of BPL agents (at ATC 3 level) dispensed per year over time. The data analysis was performed with R Studio version 1.1.383.
The study received approval from the Monash University Human Research Ethics Committee. The analyses and the final article was approved by the Commonwealth Department of Human Services.
Results
More than 1.6 million person-years of observations were included in our study, of which more than 1 million person-years involved BPL dispensing. Summary statistics of the study sample by calendar year are presented in supplemental Tables 1 and 2. Overall, the standardized prevalence of BPL dispensing increased from 58.2% in 2006 to 65.9% in 2016 (P < .01; Table 1). BPL dispensing in males has exceeded that in females since 2009 and the differences have increased over time (67.6% vs 64.2% in males and females in 2016; Figure 1 and Table 1).
Logistic Regression on the Prevalence of Blood Pressure Lowering Agents Dispensing Over Time.


Prevalence of blood pressure lowering agents dispensing by gender over time (direct standardization by age and gender).
We observed greater increases in BPL dispensing among males than females across all age groups over time (Figure 2 and Table 1). BPL dispensing was consistently higher in males than females in the 65-74 year age group. The magnitude of the differences increased over time (65.1% versus 59.2% in males and females in 2016). In contrast, BPL dispensing was higher among females in the older age groups. However, the magnitude of the differences between males and females gradually decreased over time, especially in the 75-84 year age group (71.7% versus 72.3% in males and females in 2016).

Prevalence of blood pressure lowering agents dispensing by age and gender over time.
Among those with BPL dispensing from 2006 to 2016, the proportions of multicategory BPL dispensing (≥3 categories of BPL agents at ATC3 level) were higher in the older age groups, but overall maintained at around 14% in the target population. The proportions increased in the ≥85 years age group from 16.9% in 2006 to 19.7% in 2016. The proportion of those with ≥4 BPL categories dispensing slightly increased in all age groups (1.5% to 2% in the 65-74 years; 2.4% to 3% in the 75-84 years; and 2.6% to 3.7% in the ≥85 years) over time (Figure 3).

Proportion of multicategory blood pressure lowering agents dispensing (at ATC3 level). ATC indicates Anatomical Therapeutic Chemical.
Dispensing patterns are summarized in Figure 4 and Table 2. While ACEIs/ARBs in singular form remained dominant, we observed a 37% increase in FDC (containing at least one ACEI/ARB agent) dispensing over time, from 22.6% in 2006 to 30.9% in 2016. The dispensing of CCBs (29.7%-24.7%) and low-ceiling diuretics (9.1%-4.6%) declined by 17% and 49%, respectively. There were little changes in the dispensing of BBs (28.6%-30.9%) and other diuretics (high-ceiling, potassium-sparing, and FDC of diuretics; 18.0%-16.5%). Finally, despite low volumes, the dispensing of antihypertensives in the C02 category slightly increased from 4.9% to 6.2%.

Patterns of blood pressure lowering agents dispensing over time.
Logistic Regression on the Proportion of Blood Pressure Lowering Agents Dispensing by Sub-Categories.a
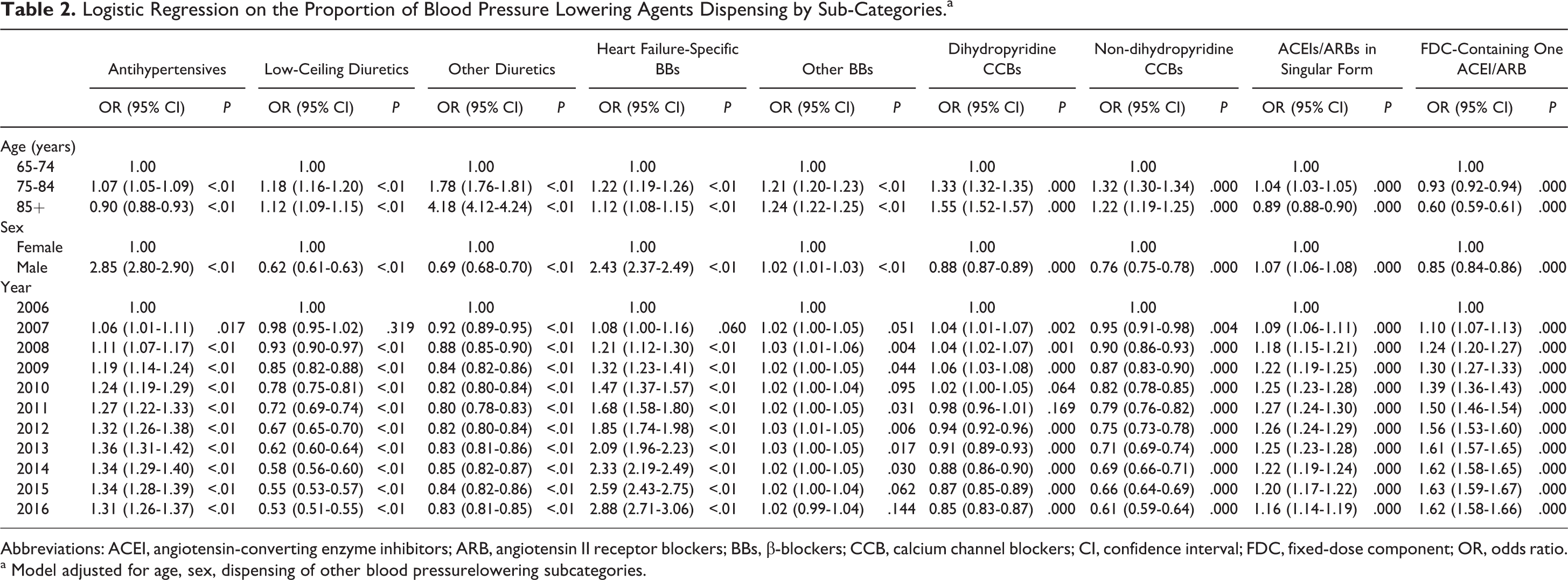
Abbreviations: ACEI, angiotensin-converting enzyme inhibitors; ARB, angiotensin II receptor blockers; BBs, β-blockers; CCB, calcium channel blockers; CI, confidence interval; FDC, fixed-dose component; OR, odds ratio.
a Model adjusted for age, sex, dispensing of other blood pressurelowering subcategories.
Detailed dispensing patterns by age groups are presented in Figure 5. Despite steady increases in all age groups, FDC dispensing was consistently lower in the older age groups, but the dispensing of other diuretics (high-ceiling, potassium-sparing, and FDC of diuretics) was higher. BB dispensing remained relatively consistent over time among people aged 65-74 years and 75-84 years, but increased among those aged ≥85 years (29.5%-36%). The dispensing of heart failure-indicated BBs more than doubled from 2006 to 2016 in all age groups. Dihydropyridine CCBs were more commonly used than non-dihydropyridine CCBs. Over time, the dispensing of dihydropyridine CCBs declined in the 65-74 and 75-84 years groups, but slightly increased among those aged ≥85 years. The dispensing of non-dihydropyridine CCBs almost halved in all age groups from 2006 to 2016 (Figure 5).

A, Categories of blood pressurelowering medication dispensing by age. B, Sub-Categories of blood pressurelowering medication dispensing by age.
Discussion
To the best of our knowledge, this is the first study describing long-term temporal trends of BPL dispensing among older Australians. The findings provide important insight into the management of a common condition, notwithstanding a variety of indications for these drugs (e.g. coronary heart disease and heart failure).
The dispensing of BPL agents increased steadily among older Australian aged 65 years and above from 2006 to 2016. The proportions of multicategory BPL dispensing increased with age. As for categories, ACEIs/ARBs in singular form were the dominant BPL agents (with >50% BPL dispensed being singular form ACEIs/ARBs) over the 11-year study period. The uptake of FDC containing either an ACEI or ARB agent increased over time in all age groups and was consistently higher in the younger age groups. Low-ceiling diuretics remained consistently low and decreased over time in all age groups. Other diuretics were more frequently dispensed among those aged ≥85 years. The dispensing of CCBs, especially non-dihydropyridine CCBs, dropped in all age groups over time. BBs dispensing slightly increased in the ≥85-year group and remained steady in the younger age groups.
The steady increase in the dispensing of BPL agents to older Australians is likely related to the increasing adoption of primary and secondary prevention in Australian primary care. It may also contribute to the improved control of blood pressure in this population. According to data from the Australian National Health Survey (NHS), the prevalence of measured high blood pressure decreased by 40% from 2000 to 2012 among those aged ≥65 years. 1 There is evidence on gender differences in cardiovascular risk management. An Australian study reported that compared to females, older males were less likely to be prescribed with medications for CVD risk management. 15 However, we observed a greater increase in BPL dispensing among males than females from 2006 to 2016, suggesting the gap in preventive use of BPL agents between males and females is closing. It is possible that the awareness of the gender differences in cardiovascular risk management may be responsible for this change over time.
Over the 11-year study period, ACEIs/ARBs remained the dominant BPL agents among older Australians. This is comparable to the European studies 16 –18 and reflective of contemporary national clinical guidelines for CVD management, in which ACEIs/ARBs are recommended as first-line pharmacotherapy for most cardiovascular conditions. 4 –6 We observed increasing dispensing of FDC agents (combination of an ACEI/ARB and another agent) over time. This is consistent with emerging evidence supporting combined therapy for the control of blood pressure. 19,20 Nevertheless, FDC dispensing decreased with age, which is also in line with the clinical recommendations. Despite no evidence suggesting higher incidence of adverse effects compared to the use of the same components in their singular forms, the dispensing of FDC agents in older patients warrants discretion 21 due to the increasing risks of BPL-induced adverse events in this population, including falls, 22 hip fractures, 23 and orthostatic hypotension.
We found relatively low dispensing of diuretics (20%-28% of people receiving BPLs) among older Australians, compared to the 40%-50% reported in European studies. 16 –18 This is despite that thiazide diuretics were recommended as one of the first-line pharmacotherapies for uncomplicated hypertension in older people. 6 A 2016 update of the guidelines downplayed the role of thiazide diuretics as first-line BPL agents in this population, but the flow-on effects of this would not have been evident in our cohort, which was followed until 2016. 7 The positive correlation between age and the use of high-ceiling and potassium-sparing diuretics likely reflects the age-related prevalence of edema and heart failure. According to the Australian NHS, 12.1% Australians aged ≥85 years self-reported being diagnosed with heart failure in 2012, which was 50% higher than those aged 75-84 years. 1
We observed a decrease in CCB dispensing across all age groups over time, which is consistent with the results from the German health examination survey. 16 The drop in non-dihydropyridine CCBs was especially notable. Compared with other BPL agents, there seems to be more uncertainties regarding the clinical utility of CCB as a first-line medication for blood pressure management, 24 as well as the effect of CCBs in preventing future cardiovascular events. 25 In addition, the fact that non-dihydropyridine CCBs generally should not be used along with BBs due to the concerns about heart block is another contributing factor. BB dispensing was consistently higher and became increasingly popular in the older age groups over time. This is possibly attributable to the increasing prevalence of coronary artery disease, heart failure, and tachycardia arrhythmia with age in the older population. 1 There were sharp increases in the uptake of heart failure-indicated BBs across all three age groups, especially in the ≥85-year group. This is in line with the timing of the updates from the European Cardiac Society and the National Heart Foundation of Australia guidelines in 2011, in which the use of bisoprolol, carvedilol, and nebivolol in stabilized heart failure patients was emphasized. 26
The American National Health and Nutrition Examination Survey estimated that about 13% of patients under medical treatment for hypertension had resistant hypertension. 27 This accords with our finding that 14% of individuals with BPL dispensing received 3 or more categories of BPL agents over time.
There are limitations of our study that warrant mention. First, we were unable to ascertain the indications for BPL dispensing as no other clinical information was available in the PBS data set. Nor were we able to verify whether people actually took the dispensed BPL agents. These limit comparisons of our data with external data, but not “internal” comparisons across the various categories of BPL agents over time, which was the primary focus of our study. Secondly, persons with BPL dispensed outside the PBS were excluded. Most BPL agents, being off patent, can be purchased privately at low cost. However, very few “long-term concession” older Australians would purchase medications privately ouside the PBS. 13 On a related matter, “long-term concession” older Australians may not be representative of all Australians aged ≥65 years. They do, however, comprise more than 80% of the target population. 13 Finally, due to the lack of prescribing information in the PBS data set, the number of categories of BPL dispensing calculated in our study may not accurately reflect concomitant of BPL agents.
Conclusion
The prevalence of BPL dispensing steadily increased among older Australians from 2006 to 2016. The changes in BPL dispensing patterns were largely in line with contemporary changes to clinical guidelines for an aging population.
Footnotes
Authors’ Note
S. Si, R. Ofori-Asenso, J. Ilomaki, C. Reid, and D. Liew contributed to conception. S. Si, T. Briffa, and F. Sanfilippo contributed to design. S. Si, R. Ofori-Asenso, and J. Ilomaki contributed to acquisition and interpretation. S. Si and C. Reid contributed to analysis. T. Briffa and F. Sanfilippo contributed to interpretation. S. Si drafted the article. All the authors critically revised the article and gave final approval. S. Si agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Acknowledgments
The authors would like to acknowledge the Australian Government Department of Human Services for providing the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.