
Abstract
Chronic angina pectoris is associated with considerable morbidity and mortality, especially if treated suboptimally. For many patients, aggressive pharmacologic intervention is necessary in order to alleviate anginal symptoms. The optimal treatment of stable ischemic heart disease (SIHD) should be the prevention of angina and ischemia, with the goal of maximizing both quality and quantity of life. In addition to effective risk factor modification with lifestyle changes, intensive pharmacologic secondary prevention is the therapeutic cornerstone in managing patients with SIHD. Current guidelines recommend a multifaceted therapeutic approach with β-blockers as first-line treatment. Another important pharmacologic intervention for managing SIHD is nitrates. Nitrates can provide both relief of acute angina and can be used prophylactically before exposure to known triggers of myocardial ischemia to prevent angina. Additional therapeutic options include calcium channel blockers and ranolazine, an inhibitor of the late inward sodium current, that can be used alone or in addition to nitrates or β-blockers when these agents fail to alleviate symptoms. Ranolazine appears to be particularly effective for patients with microvascular angina and endothelial dysfunction. In addition, certain antianginal therapies are approved in Europe and have been shown to improve symptoms, including ivabradine, nicorandil, and trimetazidine; however, these have yet to be approved in the United States. Ultimately, there are several different medications available to the physician for managing the patient with SIHD having chronic angina, when either used alone or in combination. The purpose of this review is to highlight the most important therapeutic approaches to optimizing contemporary treatment in response to individual patient needs.
Introduction
The most common cause of morbidity and mortality in the world is coronary artery disease (CAD). In 2013, cardiovascular disease resulted in approximately 800 000 deaths, resulting in about 1 of every 3 fatal cardiac events in the United States. 1 Based on data from 2009 to 2012, approximately 15.5 million people in the United States carried a diagnosis of CAD, 7.6 million had myocardial infarction (MI), and 7.8 million had angina pectoris. 1 Angina is the initial manifestation of CAD in 50% of patients, and the incidence of chronic angina or stable ischemic heart disease (SIHD) in patients ≥45 years of age is approximately 565 000 cases per year. 1,2 Although the age-specific mortality from CAD has been declining over the past several decades, CAD remains the most common cause of death worldwide and the prevalence is projected to increase by about 18% by the year 2030. 1 Furthermore, the total direct medical costs for management of cardiovascular diseases are projected to triple in the United States from US$273 billion to US$818 billion by the year 2030. 3
Each year approximately 660 000 patients are diagnosed with a new MI in the United States, and even more patients are hospitalized for unstable angina and for evaluation and management of chest pain syndromes. 1,4 In addition to hospitalizations, chronic chest pain syndromes are associated with markedly increased indirect costs due to several factors including decreased productivity, inability to work, loss of employment, and reduced quality of life. The Randomized Intervention Treatment of Angina trial poignantly illustrates these points: among men aged ≤60 years of age, 22% of those who underwent coronary artery bypass grafting and 26% of those who underwent percutaneous transluminal coronary angioplasty PTCA were unemployed 2 years afterward due to heart disease-related reasons. 5 Additionally, patients with angina compared to those without angina had a significant decline in many facets of quality of life despite having only mild angina (Canadian Cardiovascular Society angina grade 1). 5 Similarly, in the Bypass Angioplasty Revascularization Investigation trial, approximately 30% of those who underwent coronary revascularization did not resume working and 15% to 20% of patients who underwent revascularization rated their health as “fair” or “poor.” 6 A more recent 2013 study by Jespersen et al found that compared to patients without angina, those with anginal symptoms and angiography showing normal-appearing coronary arteries, diffuse nonobstructive CAD, or obstructive CAD had a 3-fold higher probability of disability pension and a 1.5-fold higher probability of premature exit from the workforce. 7 From these data, it can be concluded that chronic angina is associated with considerable morbidity and impaired quality of life, which highlights the need for aggressive management to alleviate anginal symptoms and provide secondary prevention for future cardiovascular events.
Current Guidelines for the Treatment of Stable Angina
The most recently published 2012 American College of Cardiology (ACC)/American Heart Association (AHA) and 2013 European Society of Cardiology guidelines for the management of SIHD recommend aggressive risk factor modification in addition to intensive medical therapy (defined as optimal medical therapy [OMT]) as the first treatment strategy for a majority of these patients. 4,8 The dual goals of these recommendations are to improve “quantity” of life by reducing morbidity and mortality and to improve “quality” of life by reducing symptom burden. Aggressive lifestyle modifications include cigarette smoking cessation, maintaining a healthy weight, engaging in physical activity (at least 30-60 minutes a minimum 5 days/week), and adopting a healthy diet (low in trans fat, saturated fat, and cholesterol; high in fresh fruits, vegetables, and whole grains; and reduced sodium intake). Risk factor modification should be aimed at keeping the blood pressure, low-density lipoprotein cholesterol, and glucose levels at target goals, as shown in Table 1.
Guideline-Recommended Dual Goals in the Management of Patients With SIHD.

Abbreviations: ACE, angiotensin-converting enzyme; ARB, aldosterone receptor blockers; BP, blood pressure; CABG, coronary artery bypass grafting; HMG Co-A, 3-hydroxy-3 methyl-glutaryl-CoA; PCI, percutaneous coronary intervention; SIHD, stable ischemic heart disease.
aGuidelines for the management of SIHD broken down into symptomatic treatment (quality of life) and mortality-reducing therapy (quantity of life). bModified from Padala et al. 9
Mechanisms of Coronary Arterial Function/Dysfunction
Since 1974, when Gould and Lipscomb described the effects of gradual coronary artery narrowing on resting and maximal coronary blood flow, SIHD has been thought to be the result of a mismatch between oxygen supply and metabolic requirements of the myocardium due to significant epicardial coronary stenosis. 10 Health-care providers often equate signs and symptoms of ischemia with the presence of coronary stenosis. However, of those patients with angina, 40% present with normal epicardial coronary arteries on angiography, particularly among women with suspected CAD. 11 The Women’s Ischemia Syndrome Evaluation database showed that 3 to 4 million patients in the United States have no objective evidence of obstructive atherosclerosis but have objective signs and symptoms of ischemia. 12,13 Several mechanisms have been proposed to explain the physiopathology behind these observations, including inflammation, macrovascular and microvascular spasm, microvascular dysfunction, coagulation abnormalities, and endothelial dysfunction. 14,15 Among these, endothelial dysfunction is the main pathogenic mechanism and has been shown to be present in patients with risk factors for CAD, even without obstructive disease.
Although guidelines have endorsed the importance of these pathological pathways in the diagnostic criteria for ischemic heart disease, many patients receive little or no therapy when coronary angiography reveals no epicardial coronary obstruction. 8,16,17 Such patients are frequently assumed to have noncardiac chest pain. Unfortunately, a significant percentage of these patients go on to develop acute cardiovascular events because of disease involving the arteriolar resistance vessels or coronary microcirculation and endothelial dysfunction leading to impaired coronary flow reserve. 18,19
Introduction to Treatment Options in the Management of Angina and SIHD
Optimal medical therapy is the mainstay for all patients with SIHD, and a summary of OMT treatment options for SIHD based on the 2012 ACC/AHA guidelines is shown in Table 2. Great strides have been made in both the understanding of the pathophysiology of CAD and the development of new therapeutic “disease-modifying” agents, which have led to proven survival benefits. 20 These therapies include antiplatelet agents, statins, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, and aldosterone antagonists. In addition to improving survival with OMT, it is important to reduce both symptoms and the burden of ischemia using β-blockers, calcium channel blockers, nitrates, and more recently ranolazine (late inward sodium channel inhibitor), as shown in Table 3. These agents can be used alone or in combination as dictated by guidelines according to the clinical scenario.
Summary of Guidelines for the Management of SIHD.a,b
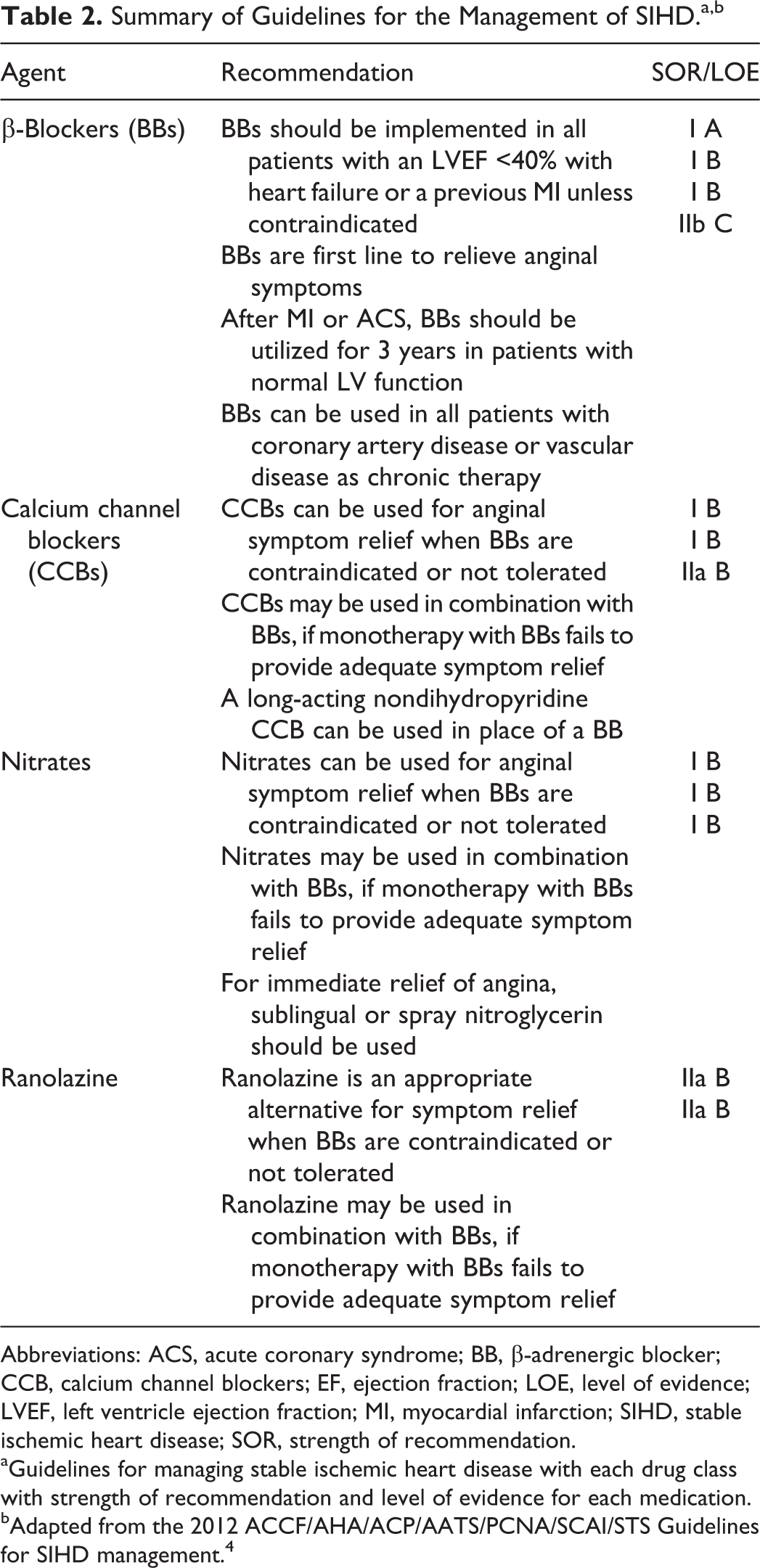
Abbreviations: ACS, acute coronary syndrome; BB, β-adrenergic blocker; CCB, calcium channel blockers; EF, ejection fraction; LOE, level of evidence; LVEF, left ventricle ejection fraction; MI, myocardial infarction; SIHD, stable ischemic heart disease; SOR, strength of recommendation.
aGuidelines for managing stable ischemic heart disease with each drug class with strength of recommendation and level of evidence for each medication.
bAdapted from the 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guidelines for SIHD management. 4
Anti-Ischemic Drugs for Treatment of Angina Pectoris.a

Abbreviations: ACS, acute coronary syndromes; AV, atrioventricular; COPD, chronic obstructive pulmonary disease; CYP3A, cytochrome P450 3A; CYP3A4, cytochrome P450 3A4; EF, ejection fraction; ISDN, isosorbide dinitrate; ISMN, isosorbide-5-mononitrate; ISMN SR, isosorbide mononitrate sustained release; LV, left ventricular; MI, myocardial infarction; PDE, phosphodiesterase; SBP, systolic blood pressure.
aAdverse effects, contraindications, and recommended ideal patient population for each drug class in the management of stable ischemic heart disease.
bNondihydropyridines (verapamil and diltiazem).
Antianginal or Anti-Ischemic Therapies for Stable Angina
β-Blockers
β-Blockers are first line in symptom management in patients with SIHD, especially those with prior or recent MI, and are a vital component of anti-ischemia therapy. 4 β-Blockers exert their antianginal effects by lowering the heart rate, afterload, rate-pressure product, and contractility, all which work to reduce myocardial oxygen demand (Figure 1). In addition, they increase diastolic filling time and coronary perfusion, which improves oxygen supply. In patients with acute coronary syndrome (ACS) and heart failure, β-blockers significantly reduce mortality rates. 21 -26
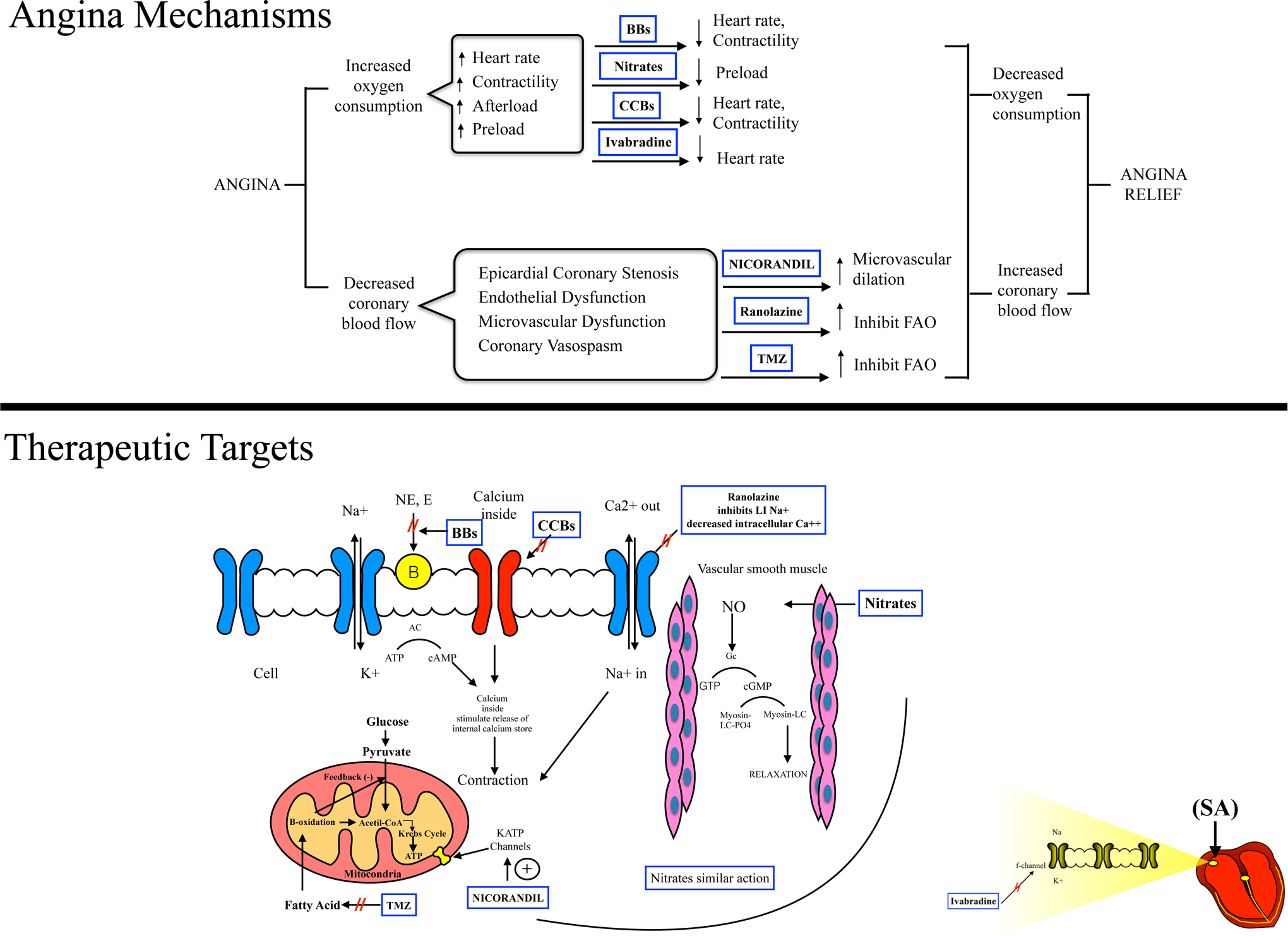
Angina mechanisms and therapeutic target for chronic ischemic heart disease. β-Blockers (BBs) inhibit the action of endogenous catecholamines epinephrine and norepinephrine (E, NE) on adrenergic receptors lowering the heart rate, afterload, rate-pressure product, and contractility reducing myocardial oxygen demand. Calcium channel blockers (CCBs) bind to and inhibit L-type calcium channels, reducing calcium influx into cells and reducing systemic arterial vasodilators that reduce BP (blood pressure) as well as cardiac contractility. Organic nitrates act as a substrate for NO (nitric oxide) formation, which in turn activates soluble guanylate cyclase (Gc) to produce cyclic guanosine monophosphate (cGMP) from guanosine triphosphate (GTP), relaxing vascular smooth muscle inducing arterial, and venous vasodilation resulting in decreased afterload and preload. Ranolazine inhibits the late sodium channel influx (late INa) during repolarization reducing intracellular calcium concentrations and results in lower ventricular diastolic wall tension, reduction in oxygen consumption, and improvement in angina symptoms. Trimetazidine (TMZ) (1-[2,3,4-trimethoxybenzyl] piperazine dihydrochloride) partially inhibits fatty acid oxidation (FAO) in favor of glucose oxidation (impaired in ischemic heart). Nicorandil is an adenosine triphosphate (ATP)–sensitive potassium channel agonist that causes arterial vasodilation and systemic venous and coronary vasodilation through a mechanism similar to nitrates. Ivabradine works by selectively inhibiting the If pacemaking current in the sinoatrial node (SA), which lowers the heart rate without affecting contractility or blood pressure. AC indicates adenyl cyclase; cAMP, cyclic adenosine monophosphate; Myosin-LCPO4, myosin-light chain phosphatase.
However, similar mortality benefits have not been demonstrated in the SIHD population. In a retrospective study of the Reduction of Atherothrombosis for Continued Health registry by Bangalore et al, β-blockers were not shown to reduce cardiovascular death, nonfatal MI, or nonfatal stroke in patients with CAD with or without a previous MI. 27 In a retrospective analysis of the Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management, and Avoidance trial, utilizing β-blockers in patients with a previous MI, but without a history of heart failure, did not have a significant reduction in mortality compared to patients not receiving β-blocker therapy (5.3% vs 6.7%, P = .20). 28 To date, the use of β-blockers in patients with SIHD has not been shown to clearly reduce mortality. Yet, β-blockers reduce the frequency of angina and increase the threshold for angina when used alone or with calcium channel blockers or nitrates. 29 -33 Support for the use of β-blockers to manage angina comes from the International Multicenter Angina Exercise (IMAGE) study and the Total Ischemic Burden Bisoprolol Study (TIBBS). 32,33 In the IMAGE study, monotherapy with metoprolol CR 200 mg daily or nifedipine modified-release 20 mg twice daily were compared, as well as monotherapy versus combination therapy with both agents in 280 patients with SIHD. Monotherapy with a β-blocker was superior to monotherapy with calcium channel blockers as measured by time to ST-segment depression on exercise stress testing. Combination therapy with both agents did not seem to exhibit an additive effect in individual patients. 33 The TIBBS randomized trial also compared the effectiveness of β-blockers and calcium channel blockers in treating SIHD and found that both medications effectively reduced the frequency and duration of ischemic episodes. However, β-blockers were found to be significantly superior to calcium channel blockers in both categories. 32 As a result of these data, the recent SIHD guidelines endorse β-blockers as first-line therapy for relief of angina. 4 A summary of the available β-blockers with their pharmacokinetic and pharmacodynamic properties is shown in Table 3.
Nitrates
Organic nitrates have been an integral part of the therapeutic armamentarium for angina since 1879 when William Murrell first used one for the treatment of angina. 34 Nevertheless, there is no evidence to show that nitrates reduce mortality in SIHD. In addition to its utility in the SIHD population in terms of symptom relief, nitroglycerin (NTG) is also used to provide relief of chest pain in patients with ACS, in the treatment of hypertension, and as an “unloading” agent in acute and chronic heart failure. 35,36
Organic nitrates act as a substrate for nitric oxide (NO) formation, which in turn activates soluble guanylate cyclase to produce cyclic guanosine monophosphate (cGMP), relaxing vascular smooth muscle.
37
Endothelial dysfunction disrupts the endothelial
Nitrates induce arterial and venous vasodilation resulting in decreased afterload and preload, which decreases left ventricular (LV) wall tension and end-diastolic pressures. This results in a reduction in the cardiac workload, which in turn reduces myocardial oxygen demand. Nitrates have been shown to augment coronary perfusion by various mechanisms including vasodilation of the epicardial coronary arteries, vasodilation of coronary stenoses, prevention or reversal of coronary vasoconstriction, improvement of endothelial dysfunction, and enhanced collateral blood flow. 39 All these effects redistribute coronary blood flow to ischemic zones. Although coronary steal syndrome is a concern in patients with CAD, nitrates are unlikely to cause this syndrome.
The organic nitrates currently marketed in the United States for the management of angina are NTG, isosorbide dinitrate (ISDN), and isosorbide-5-mononitrate (ISMN). These agents are comparable in terms of anti-ischemic potency and likelihood of tolerance development but have different pharmacokinetic properties and availability of dose delivery systems, as shown in Table 4. Short-acting nitrates are typically prescribed for relief of acute anginal symptoms. They can also be used prophylactically before exercise as they have been shown to improve exercise tolerance and avert exercise-induced anginal attacks. 45,46 Short-acting nitrates can also be used for breakthrough anginal symptoms in patients already on long-acting nitrates. Long-acting nitrates such as ISDN and ISMN are frequently used alone or with other antianginal medications to reduce or eliminate the incidence of angina in SIHD. 47 -49
Pharmacokinetics of Available Nitrate Formulations.

Abbreviations: ISDN, isosorbide dinitrate; ISMN, isosorbide-5-mononitrate; SR, sustained release.
aPharmacologic information of the various nitrate formulations including route of administration, dosing, onset and duration of action.
The mainstay treatment for both acute angina and angina prophylaxis is sublingual NTG tablets or spray. A small randomized study involving 20 healthy patients demonstrated that sublingual NTG spray resulted in faster (2 minutes vs 3 minutes) and more sustained (15 minutes vs less than 10 minutes) brachial artery dilation, assessed by ultrasound compared with sublingual NTG tablets. 50 Similarly, ISDN oral spray was significantly more rapid in abating anginal symptoms following bicycle ergometry in 9 elderly patients compared to the sublingual tablet (61.6 ± 24.4 seconds vs 112.4 ± 70 seconds; P < .0005). 51 The time required for dissolution of sublingual NTG tablet may vary, as substantial intersubject variability exists. This explains the slightly delayed action of sublingual tablet compared to sublingual spray, which is absorbed instantly. Furthermore, NTG spray was superior to NTG tablet in alleviating exercise-induced anginal pain in 10 patients. 52 Hence, sublingual NTG spray may be more beneficial in patients living in warmer climates, those with dry mouth, or in elderly patients with dentures. In addition, the spray may be more convenient and easier to administer compared to the tablet, especially in elderly patients.
The major concern with continued use of nitrates is the development of nitrate tolerance/tachyphylaxis, which results in the diminution of its anti-ischemic effects. Patients on long-acting nitrates are more likely to develop tolerance than those who require only short-acting nitrates. The precise mechanism of tolerance is not known. One hypothesis is that short-term treatment with nitrates may result in a pseudotolerance where a counterregulatory response leads to activation of vasoconstrictor signals and intravascular volume expansion. On the other hand, long-term treatment may result in vascular tolerance where there is a loss of nitrovasodilator responsiveness due to increased production of vascular superoxide and vasoconstrictor hypersensitivity. 53 Escalating nitrate dose does not circumvent tolerance. Instead, providing a nitrate-free interval typically restores nitrate responsiveness and is the primary strategy in preventing tolerance. A 10- to 12-hour period free of nitrate exposure is recommended with long-acting nitrate preparations such as with NTG patches and ointment or preparations of ISDN or ISMN. The prevention of tolerance can be achieved by altering administration times, allowing for this nitrate-free interval to occur at nighttime, when angina is least likely to occur. 54
Nitrate rebound or withdrawal can also occur when long-acting nitrates are discontinued abruptly and typically presents as worsening anginal pain. Gradually titrating the dose or adjusting the timing of the nitrate administration along with other antianginal agents can mitigate this unfortunate phenomenon.
In patients with SIHD, nitrates effectively reduce the occurrence of anginal episodes, enhance exercise duration, and increase time to ST-segment depressions during exercise treadmill testing. 55 -57 The current guidelines recommend instituting long-acting nitrates for the management of angina when β-blockers are contraindicated or not tolerated due to side effects. They can also be combined with β-blockers, when β-blocker therapy alone is ineffective in providing anginal relief. 4 For acute angina, sublingual NTG or NTG spray is recommended in all patients with SIHD. 4
Calcium Channel Blockers
Calcium channel blockers can be broadly classified into 2 classes: dihydropyridines (nifedipine and amlodipine) and nondihydropyridines (verapamil and diltiazem). They reduce heart rate, afterload, and contractility, thereby decreasing myocardial oxygen demand and improve oxygen supply through coronary vasodilation. Calcium channel blockers effectively reduce anginal frequency, ST-segment depressions on Holter monitoring, NTG consumption, and improve exercise duration. 58 -60 Data supporting the use of calcium channel blockers in SIHD comes from the Circadian Anti-Ischemic Program in Europe trial. 58 In this double-blinded, parallel trial, 250 patients with symptomatic stable angina were randomized to amlodipine or placebo. Amlodipine reduced the frequency of ST-segment depression (60% vs 44% reduction, P = .025), angina frequency (70% reduction vs 44% reduction, P = .0001), and patient-reported NTG use (67% reduction vs 22% reduction, P = .0006). 58 Calcium channel blockers are also effective in preventing coronary vasospasm and are the first-line agent for Prinzmetal (variant) angina as monotherapy or in combination with nitrates. 61,62
Although calcium channel blockers are effective antianginal agents, similar to β-blockers, they do not reduce mortality in SIHD, as was demonstrated in the literature. 63 In this study, participants with SIHD were randomized to nifedipine 60 mg daily or placebo, in addition to background therapy. There was no significant difference in the death rate when comparing the nifedipine arm to the placebo arm (nifedipine was 1.64 per 100 patient years compared to 1.53 per 100 patient years in the placebo arm, P = .41). When added to standard therapy, calcium channel blockers did not reduce mortality or the primary end point of death, acute MI, refractory angina, new overt heart failure, debilitating stroke, and peripheral revascularization. 63 The guidelines recommend calcium channel blockers as monotherapy for angina relief when β-blockers are contraindicated or cause intolerable side effects. 4 They can also be used as a combination therapy with β-blockers when β-blockers alone fail to alleviate anginal symptoms. 4 Current available calcium channel blockers are summarized in Table 3.
Ranolazine
Ranolazine functions by inhibiting the late sodium channel influx (late INa) during repolarization. This reduces intracellular sodium concentrations and results in lower ventricular diastolic wall tension, reduction in oxygen consumption, and improvement in angina symptoms 64 In addition, it has been suggested that ranolazine plays a role in the inibition of fatty acid oxidation with resultant attenuation of oxidative stress. 65 Ranolazine reduces angina without any significant change in hemodynamic parameters, which makes it a useful therapeutic option in patients with hypotension or bradycardia. Ranolazine also prolongs the ventricular action potential and QTc interval through inhibition of the rapid delayed rectifier potassium current (IKr) in a dose-dependent manner. Ranolazine alone or with other therapies significantly decreases the frequency of angina and NTG use, improves exercise duration, and delays the onset of ST-segment depression during exercise. 66 -69 Several randomized trials have evaluated the efficacy of ranolazine in the management of SIHD. 66,67,69,70 The Monotherapy Assessment of Ranolazine in Stable Angina trial randomized 191 patients with angina-limited exercise to various doses of ranolazine or placebo. 66 A significant dose-related increase in exercise duration was demonstrated in all groups managed with ranolazine (P < .005 for all comparisons), with negligible changes in blood pressure and heart rate. 66 The Combination Assessment of Ranolazine in Stable Angina (CARISA) trial also found improvements in exercise tolerance in patients taking ranolazine compared to placebo. 67 In this study, 823 adults were randomized to placebo and either 750 mg or 1000 mg of ranolazine. The participants then underwent exercise treadmill testing 2, 6, and 12 weeks into treatment. Patients taking ranolazine at either dose had increased exercise tolerance on treadmill testing (P < .02). 67 Additionally, ranolazine was shown to be associated with a dose response decrease in angina attacks per week in comparison with placebo. 67
In the randomized, double-blinded Metabolic Efficiency With Ranolazine for Less Ischemia in Non-ST-Elevation Acute Coronary Syndromes–Thrombolysis in Myocardial Infarction (MERLIN-TIMI) 36 trial, patients with non-ST-segment elevation MI were managed with either ranolazine or placebo in addition to the background therapy. 70 The use of ranolazine was not associated with a significant decrease in the primary composite end point of cardiovascular death, MI between the 2 groups (21.8% ranolazine vs 23.5% placebo, P = .11). 70 However, recurrent ischemia was significantly reduced in the ranolazine group (13.9% vs 16.1% for placebo; P = .03). 70 Furthermore, despite a small increase in QTc, there was no significant increase in documented arrhythmia (3.0% vs 3.1%, P = .84), supporting the safety of this medication. 70 In a prespecified analysis, the authors of the MERLIN-TIMI 36 trial evaluated the antianginal efficacy of ranolazine in a subgroup of patients with chronic angina who presented with ACS. 71 Ranolazine compared to placebo was associated with a significant reduction in the primary composite end point of cardiovascular death, MI, or recurrent ischemia. However, this was primarily a result of a reduction in recurrent ischemia and ranolazine did not impact cardiovascular death or MI in patients with chronic angina. These findings from MERLIN-TIMI 36 trial demonstrate that ranolazine is an effective antianginal agent but does not reduce mortality. 71
In patients with diabetes mellitus, ranolazine has demonstrated significant reductions in glycosylated hemoglobin (HbA1c), thus making it an appealing option for managing angina in these patients. 72,73 In a post hoc analysis of the CARISA trial, there was a 0.48% ± 0.18% (P = .008) reduction in HbA1c with 750 mg twice-daily dosing and a 0.70% ± 0.18% (P = .0002) reduction in HbA1c with 1000 mg twice-daily dosing when compared to placebo after 12 weeks of therapy. 72 A recent randomized controlled trial, the Type 2 Diabetes Evaluation of Ranolazine in Subjects with Chronic Stable Angina (TERISA), enrolled 949 patients with diabetes, CAD, and stable angina who were being treated with 1 to 2 antianginals at baseline to treatment with ranolazine or placebo. 69 Ranolazine was found to significantly lower weekly angina frequency and weekly sublingual NTG use. 69 A subgroup analysis of the TERISA trial grouped patients by HbA1c levels and found that ranolazine was significantly better than placebo at all levels of HbA1c and that reduction in weekly angina episodes was greater in those patients with greater HbA1c levels. 69 Additionally, as a part of the MERLIN-TIMI 36 trial, the effects of ranolazine on hyperglycemia were prospectively evaluated. 73 Patients with diabetes treated with ranolazine had a significant reduction in HbA1c, had a greater likelihood of having an HbA1c <7% at 4 months, and were less likely to have a ≥1% increase in HbA1c at 1 year. 73
The guidelines for the management of SIHD recommend ranolazine as monotherapy for anginal relief when β-blockers are contraindicated or cause intolerable side effects. Ranolazine can also be used along with β-blockers as a combination therapy, when β-blockers alone fail to alleviate anginal symptoms. 4
Antianginal Agents Currently Approved in Europe Only
Trimetazidine
Trimetazidine is approved as a second-line agent for the prevention of angina in Europe for those patients already on β-blockers or calcium channel blockers (class IIb, B). 8 Trimetazidine inhibits the enzyme 3-ketoacyl-CoA thiolase and diverts the metabolism from fatty acid oxidation to glucose oxidation, which requires less oxygen, thereby decreasing myocardial oxygen requirements. Trimetazidine does not impact heart rate, blood pressure, or myocardial contractility. 74 Gastrointestinal symptoms are the primary side effect, but this is uncommon. In a meta-analysis of randomized studies, using trimetazidine alone or in addition to other antianginal medications reduced the number of angina episodes per week, delayed time to ST-segment depression, and had comparable efficacy to conventional antianginal therapies. 75
Nicorandil
Nicorandil is an adenosine triphosphate–sensitive potassium channel agonist, approved as a second-line agent in combination with β-blockers or calcium channel blockers for angina prevention in Europe only (class IIa, B). 8 Nicorandil is unique in that it causes arterial vasodilation as its primary mechanism but also contains a nitrate moiety that induces systemic venous and coronary vasodilation. 76 These 2 mechanisms of action allow nicorandil to reduce preload and afterload as well as increase coronary blood flow. In randomized, double blinded trials, nicorandil has demonstrated that it improves exercise tolerance compared to placebo and is as effective antianginal agent as nitrates, β-blockers, or calcium channel blockers as measured by exercise tolerance testing. 77 Side effects include potential flushing, headache, palpitations, nausea, vomiting, and gastrointestinal ulcerations.
Ivabradine
Ivabradine is approved for treating heart failure but not angina in the United States. The European guidelines recommend ivabradine as a second-line agent for the treatment of angina for a specific patient population, namely, patients with normal sinus rhythm with a heart rate >60 beats per minute and with a contraindication or an inability to tolerate β-blockers (class IIa, B). 8 Ivabradine works by selectively inhibiting the If pacemaking current in the sinoatrial node, which lowers the heart rate without affecting contractility or blood pressure. 8 This, in turn, increases the diastolic filling time, thereby increasing coronary perfusion. The side effect profile for ivabradine includes bradycardia, heart block, dizziness, blurred vision, and transient luminous visual disturbances, such as phosphenes. 78 It has been demonstrated that ivabradine is comparable to atenolol and amlodipine in improving exercise performance, reducing the quantity of angina attacks and NTG use, and in delaying time to ST-segment depression and time to limiting angina. 79,80
In morBidity–mortality EvAlUaTion of the If inhibitor ivabradine in patients with coronary disease and left ventricULar dysfunction (BEAUTIFUL) trial, 12 473 patients with SIHD with left ventricular ejection fraction (LVEF) <40% were randomized to ivabradine or placebo. 81 Ivabradine was not shown to impact the primary composite outcome of cardiovascular death, admission for acute MI, or new-onset/worsening heart failure compared to placebo. However, in a specified subgroup of patients with heart rate ≥70 beats per minute, there was a significant reduction in the secondary end points of admission to the hospital for fatal and non-fatal MI and coronary revascularization. These data have led to recent Food and Drug Administration approval of ivabradine in the United States for patients with reduced LVEF.
In the recently published randomized, double-blinded, placebo controlled Study Assessing the Morbidity–Mortality Benefits of the If inhibitor Ivabradine in Patients with Coronary Artery Disease (SIGNIFY) trial, patients with SIHD without evidence of clinical heart failure and a heart rate of 70 beats per minute or more were randomized to either ivabradine or placebo added to standard background therapy. 82 Ivabradine did not significantly reduce the composite primary end point of cardiovascular death or nonfatal MI. 82 Data from the BEAUTIFUL and SIGNIFY trial suggest that ivabradine should be used in patients with SIHD with heart failure and a reduced ejection fraction only.
Future Directions
Rapamycin
Rapamycin (sirolimus) is a potent immunosuppressive agent that interrupts cellular pathways for cell growth and regulation by inhibiting the mammalian target of rapamycin. Rapamycin ameliorates angina through 2 major mechanisms: reducing LV mass and inhibiting atherosclerosis. Rapamycin has been shown to significantly reduce LV mass over time in small sample sizes of both heart and kidney transplant patients. 83,84 Theoretically, reduction in LV mass will decrease myocardial oxygen demand and could reduce angina symptoms. Current studies investigating the effects of rapamycin are limited to animal studies but have shown promising results. In LDL receptor–deficient mice, the administration of everolimus significantly reduced the burden of atherosclerotic plaque compared to placebo. 85 These investigators proposed that decreased atherogenesis is likely a consequence of reduced macrophage influx into the arterial wall, inhibiting lesion development in its earliest stages. 85 To date, randomized controlled trials utilizing rapamycin for the treatment of angina are lacking, but it remains an important area of interest for future research.
Conclusion
Angina pectoris is distressing and is associated with marked reductions in quality of life and increased risk for ACS. Angina is a manifestation of epicardial flow insufficiency as well as microvascular and endothelial dysfunction. The antianginal therapeutic armamentarium includes a number of effective anti-ischemic agents, available in various formulations and drug delivery systems. These agents are absolutely essential in targeting the “quality-of-life” goals as part of the management of SIHD. Although they do not impact overall mortality, β-blockers are first line in the management of angina symptoms. With intolerable side effects or failure to relieve symptoms, adjuvant therapy with calcium channel blockers and ranolazine provide alternative methods of controlling angina. Ranolazine is also a useful therapeutic option in patients with hypotension or bradycardia and in diabetic patients with angina. The short-acting nitrates are very effective in relieving acute anginal pain prophylactically prior to activities that may precipitate angina, such as exercise or emotional stress. Tolerance to nitrates is something that must be considered when determining optimal therapy; however, tolerance with short-acting nitrates is less likely compared to long-acting nitrates. Nevertheless, nitrate product selection should be patient specific, determined by pharmacological differences and physician/patient preference. In Europe, trimetazidine, nicorandil, and ivabradine also have indications for the management of angina in particular groups of patients.
Footnotes
Author Contributions
Santosh K. Padala, Mandeep S. Sidhu, Katherine P. Cabral, and Doralisa Morrone contributed to conception, design, acquisition, analysis, and interpretation. Santosh K. Padala, Michael P. Lavelle, Mandeep S. Sidhu, Katherine P. Cabral, and Doralisa Morrone drafted the manuscript. Michael P. Lavelle contributed to design, acquisition, analysis, and interpretation. William E. Boden contributed to conception, design, analysis, and interpretation. Peter P. Toth contributed to conception, design, analysis, and interpretation. All authors critically revised the manuscript, gave final approval, and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.