
Abstract
The development and subsequent clinical application of the β-adrenergic receptor blocking drugs represent one of the major advances in human pharmacotherapeutics. No other class of synthetic drugs has demonstrated such widespread therapeutic utility for the treatment and prevention of so many cardiovascular diseases. In addition, these drugs have proven to be molecular probes that have contributed to our understanding of the disease, and on the molecular level, both the structure and function of the 7 transmembrane G protein receptors that mediate the actions of many different hormones, neurotransmitters, and drugs. The evolution of β-blocker drug development has led to refinements in their pharmacodynamic actions that include agents with relative β1-selectivity, partial agonist activity, concomitant α-adrenergic blockers activity, and direct vasodilator activity. In addition, long-acting and ultra-short-acting formulations of β-blockers have also demonstrated a remarkable record of clinical safety in patients of all ages.
Catecholamines are neurohumoral substances that mediate a wide variety of physiologic and metabolic activities. The effects of various catecholamines, both natural and synthetic, ultimately depend on their chemical interactions with adrenergic receptors that are discrete macromolecular structures located on the cell membrane. 1 In 1948, Ahlquist conducted a series of classic pharmacologic studies and concluded from his findings that there were 2 distinct organ responses to catecholamine, which he called “α- and β-receptor mediated.” 2
The β-Adenergic Receptor
The concept of adrenergic receptor stimulation for mediating catecholamine actions had been recognized throughout the 20th century, 3 and during the past 35 years the scientists began to study the molecular steps that lay between the putative receptors and agonists and the response elements within the cell. 4 It was found that adrenergic receptors, when stimulated, can trigger the production of second messengers (eg, adenyl cyclase) via an interaction with the coupling proteins attached to the β receptor. The β- and α-receptors are a part of a major class of G protein-coupled receptors or 7 transmembrane receptors—the most important targets of clinically used drugs—that also zero in on serotonin receptors, histamine receptors, and angiotensin II receptors (Figure 1).4,5

Seven transmembrane receptors. Adapted from Lefkowitz RJ.
Using radioligand labeling techniques and purification methods, Lefkowitz and his colleagues 6 helped to identify the structures of the adrenergic receptors as membrane-bound polypeptide chains with a molecular weight of about 67 000 Da. The β-receptors consist of 7 transmembrane α-helices of 20 to 28 amino acids joined by alternating extracellular and cytoplasmic loops (Figure 2).4,7 Lefkowitz and colleagues 4 were successful in reconstituting the β-receptors and demonstrated that the receptors could convey catecholamine responsiveness when transplanted to previously unresponsive organic systems. Subsequently, the receptor genes and complementary DNAs for β-receptors were cloned in 1986, 8 and the 3-dimensional crystalline structure of the β2 receptor was recently described in 2007. 9

Proposed model for the membrane topography of the β1-adrenergic receptor. Reproduced from Ref 6 with permission.
In recognition of his pioneering work in helping to understand β-receptor structure and function, including receptor desensitization, Lefkowitz and a former graduate student of his, Brian Kobilka, won the 2012 Nobel Prize in Chemistry. 10
Development of the β-Blockers
In the early 1960s, James Black (who ultimately won the Nobel Prize in Medicine and Physiology in 1988) and his associates at Imperial Chemical Industries in Great Britain were working on a series of β-adrenergic blocking compounds, pronethanol and propranolol, that they hypothesized would lower myocardial oxygen consumption by interfering with the effects of catecholamines and therefore would be useful for the treatment of angina pectoris, hypertension, and arrhythmia. 11 Although pronethanol was effective in patients with angina pectoris, it was propranolol that became the prototype β-blocker with proven efficacy in both intravenous and oral forms for the treatment of cardiovascular disease. In 1964, propranolol became the first major advance in the treatment of angina pectoris since the introduction of nitroglycerin almost 100 years earlier. In addition, it quickly became an accepted treatment for arrhythmia, hypertension, and hypertrophic cardiomyopathy.
The potential adverse reactions related to the anticatecholamine effects of propranolol on heart rate, myocardial contractility, and bronchial tone led to ongoing refinements in the pharmacologic structure of β-blockers (Figure 3) and subsequent advances in drug delivery. 12 The evolution in drug development (Table 1) led to the introduction of drugs having relative selectivity for cardiac β1-receptors (metoprolol, atenolol), partial adrenergic agonist activity (pindolol), concomitant α-adrenergic blocking activity (labetalol, carvedilol), and direct vasodilator activity (nebivolol) 13 . In addition, long-acting and ultra-short-acting formulations of β-blockers were developed.

Molecular structure of the β-adrenergic agonist isoproterenolol and some β-adrenergic blocking drugs.
Pharmacodynamic Properties of β-Adrenergic Blocking Drugs.a

a ++ = strong effect; + = modest effect; 0 = absent effect. Adapted with permission from Frishman WH.
b Bisoprolol is also approved as a first-line antihypertensive therapy in combination with a very-low-dose diuretic.
c Carvedilol has peripheral vasodilating activity and additional α1-adrenergic blocking activity.
d Labetalol has additional α1-adrenergic blocking activity and direct vasodilatory activity.
e Nebivolol has direct vasodilatory activity related to potentiation of nitric oxide.
f Sotalol has an additional type of antiarrhythmic activity.
Pharmacodynamics of β-Blockers
β1-Selectivity
β-adrenergic blockers are now classified as being β1-selective or nonselective, according to their relative abilities to antagonize the actions of sympathomimetic amines at lower doses in some tissues than what is required in other tissues. When used in low doses, β1-selective blocking drugs inhibit cardiac β1-receptors but have less influence on β2-receptors in bronchial and vascular locations 14 ; however, given in higher doses the β1-selective agents also block β2-receptors. Accordingly, β1-selective agents may be safer than nonselective ones in patients with bronchospastic disease, since β2-receptors are still able to be stimulated and in the process mediate adrenergic bronchodilation. Nevertheless, even selective β-blockers need to be used with caution in patients with reversible bronchospasm. 14
A second theoretical advantage is that unlike nonselective β-blockers, β1-selective blockers in low doses may not block the β2-receptors that mediate dilation of arterioles. 1 During the infusion of epinephrine, nonselective blockers can cause a pressure response by blocking β2-receptor-mediated vasodilation, since α-adrenergic vasoconstrictor responses are still operative. Selective β1-antagonists may not induce the pressor effect in the presence of epinephrine and may lessen the risk of peripheral blood flow being reduced. It is possible that leaving β2-receptors unblocked (and responsive to epinephrine) may be functionally important in a subset of patients with asthma, drug-induced hypoglycemia, and/or peripheral vascular disease who need to be treated with β-blocking drugs. 1
Intrinsic Sympathomimetic Activity (partial agonist activity)
The two earliest β-blocking drugs that were synthesized, dichloroisoproterenol and pronethalol, were found to inhibit the effects of catecholamines while at the same time to stimulate adrenergic receptors, although with less potency (partial agonist activity). This concept did not catch on, and these were quickly abandoned as clinical agents. Subsequently, other agents that had much less intrinsic sympathomimetic activity (ISA; pindolol, carteolol, and penbutolol) were synthesized and then approved for clinical use. The level of ISA with these particular β-blockers caused a minor stimulation of the receptor (in the absence of catecholamines), which could be blocked by propranolol. In the presence of catecholamines, β-blockers with ISA remain effective antihypertensive agents; however, it is still debated whether a β-blocker with the potential for ISA constitutes an overall advantage or disadvantage in cardiac therapy.15,16 Drugs with ISA cause less slowing of the heart rate at rest than do propranolol and metoprolol, although the increases in heart rate with exercise are similarly blunted. 16 These β-blocking agents directly reduce peripheral vascular resistance and may also cause less depression of atrioventricular conduction than drugs lacking this action.16,17 Some investigators have made claims that ISA in a β-blocker protects against myocardial depression, adverse lipid changes, bronchial asthma, and peripheral vascular complications seen in some patients on a compound without ISA, such as propranolol. 16 The evidence to support this claim still remains unconvincing.
α-Adrenergic Activity
Labetalol and carvedilol are 2 β-blocking agents that have antagonistic effects at both α- and β-adrenoceptors, and both have direct vasodilator effects. 1 Labetalol has been shown to be 6 to 10 times less potent than phentolamine on α-adrenergic receptors and 1.5 to 4 times less potent than propranolol at β-adrenergic receptors.1,18 Labetalol is itself much less potent at α- than at β-receptors. However, the additional α-blocking property does lead to a reduction in peripheral vascular resistance in patients and better preservation of cardiac output than what is observed with propranolol. The drug is useful as a parenteral agent for treating hypertensive urgencies or emergencies and as an oral drug for chronic hypertension management in the patient receiving multiple antihypertensive agents. 19
Although carvedilol has somewhat less α-adrenergic blocking potency than labetalol (the ratio of α1 to β-adrenergic blockade for carvedilol is 1:10, as compared to 1:4 for labetalol), it is useful as a treatment for systemic hypertension and for patients with symptomatic congestive heart failure related to ischemic and nonischemic causes. 20 Unlike labetalol, carvedilol has also been shown to have antioxidant and antiproliferative properties. 20
Direct Vasodilator Activity
Nebivolol is a β1-selective adrenergic receptor antagonist with additional nitric oxide-mediated vasodilatory action on arteries and veins. In addition, the drug has similar antioxidant effects to those observed with carvedilol. Nebivolol was recently approved for clinical use in patients with systemic hypertension 21 and has been studied in patients with congestive heart failure.
Pharmacokinetics of β-Blockers
Although β-adrenergic blocking drugs as a group have similar therapeutic or pharmacodynamic actions in patients with systemic hypertension, angina pectoris, and arrhythmias, these compounds have quite varied pharmacokinetic properties and a multitude of different delivery systems that facilitate their use.14,22 For example, propranolol is a compound first introduced in an intravenous form for the treatment of angina pectoris. In its intravenous form, it is fully bioavailable. Alternatively, when given orally there is a large first pass effect that clearly influences its absolute bioavailability. Its pharmacologic half-life is approximately 3 to 4 hours, requiring that the drug be given in 4 divided doses for the treatment of angina pectoris.17,23 The drug also is very lipophilic and as such readily crosses the blood–brain barrier.15,20 Subsequently, 2 sustained-release formulations of propranolol, including 1 with delayed-release action, were developed to reduce the drug’s dosing intervals, allowing for once-daily use. 1 A delayed-release form of metoprolol is also now available, and a once-daily form of carvedilol has been introduced for use in patients with hypertension and with congestive heart failure.24,25
The nonselective β-blocker nadolol and β1-selective blocker atenolol are also intrinsically longer acting agents and are drugs excreted unchanged by the kidney.26,27 In addition, they are much less lipid soluble and will concentrate to a lesser extent in the brain.26,27
Intravenous propranolol was introduced for the treatment of arrhythmias. Intravenous forms of atenolol and metoprolol have become available for use in the hyperacute phase of myocardial infarction, 28 and intravenous labetalol has been approved for use in hypertensive emergencies. Esmolol, an ultra-short-acting β1-selective agent with a unique metabolic pathway related to hepatic and blood esterases, became available for the treatment of arrhythmias.29,30 It has been observed that there are genetic polymorphisms that can influence the hepatic metabolism of various β-blocking drugs including propranolol, metoprolol, timolol, and carvedilol.20,24,31,32
Cardiovascular Applications
The therapeutic efficacy and safety of β-adrenergic blocking drugs have been well established after 50 years of clinical use in human beings. Their clinical utility has been documented in patients with angina pectoris, cardiac arrhythmias, congestive cardiomyopathy, and hypertension and for reducing the risk of mortality and possibly nonfatal reinfarction in survivors of acute myocardial infarction. Of course, not all of the agents in the class of β-blockers have shown benefit in each of the clinical applications listed above. These drugs may be useful as a primary protection against cardiovascular morbidity and mortality in patients with hypertension. The drugs have also been found to be of use for a host of other cardiovascular disorders (Table 2).
Reported Cardiovascular Indications for β-Adrenoceptor Blocking Drugs.a
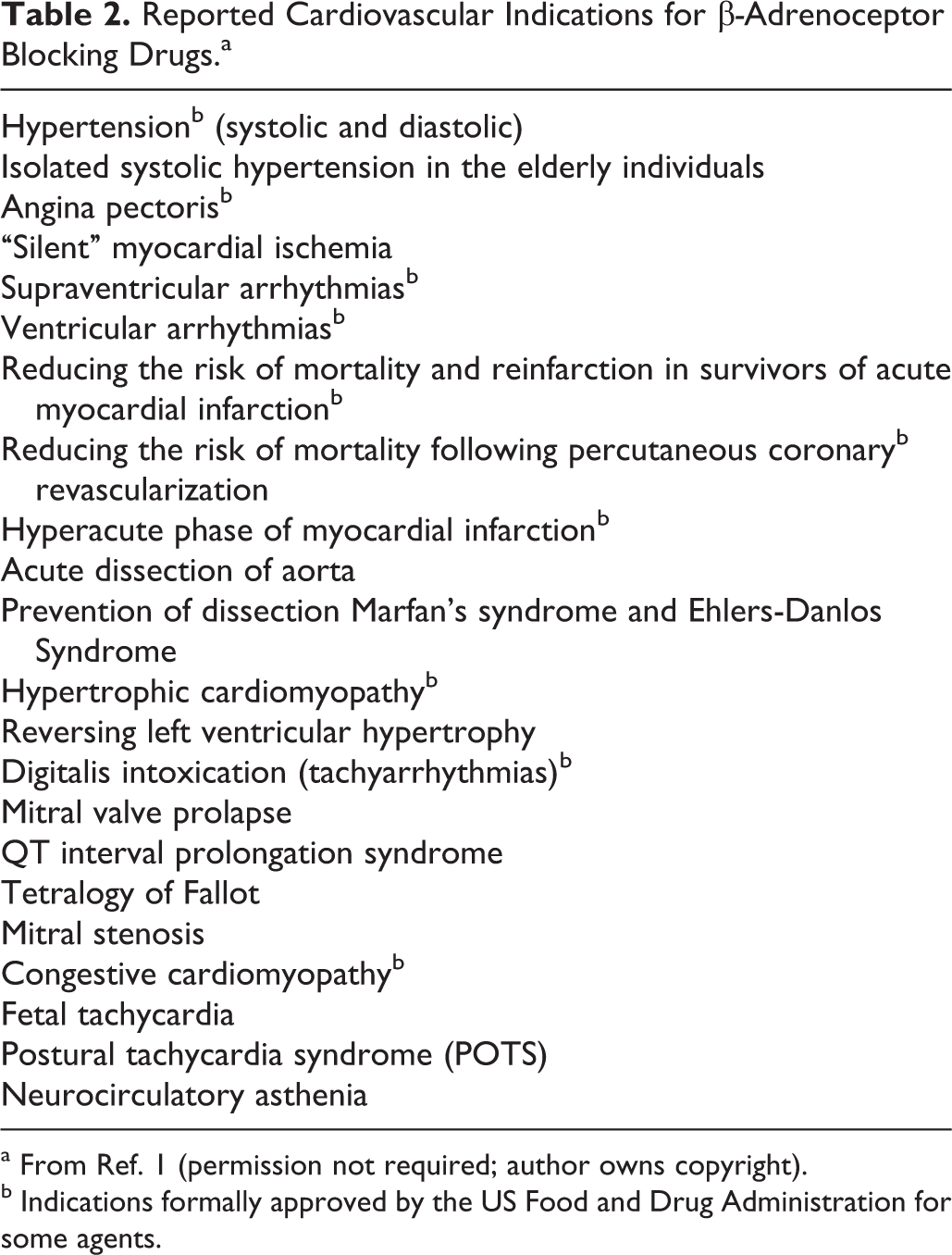
a From Ref. 1 (permission not required; author owns copyright).
b Indications formally approved by the US Food and Drug Administration for some agents.
Angina Pectoris
β-blockers were first conceived as possible treatment for patients with angina pectoris, and oral propranolol was approved for this use almost 45 years ago. 33 By blunting catecholamine-induced increases in heart rate, blood pressure, and myocardial contractility, myocardial oxygen consumption is reduced, allowing patients to increase their exercise capacity before both angina symptoms and myocardial ischemia occurs. 34 This compound can also be used in combination with nitrates and calcium channel blockers to increase antianginal effectiveness beyond what is seen with these compounds individually. In addition, β-blockers and nitrates have been shown to be first-line treatments for patients with unstable angina (preinfarction angina). 1
Virtually all available β-blockers, whether or not they have ISA, α-adrenergic action, and nonselective or β1-selective properties, produce some form of increased work capacity without pain in patients with angina pectoris.1,35 The orally active β-blockers that have been approved for use in angina pectoris include propranolol, metoprolol, atenolol, and nadolol.24,36–38
Arrhythmias
Intravenous propranolol was approved over 40 years ago for the treatment of arrhythmias, and shortly thereafter it become available in an oral form for the same indication. 1 The antiarrhythmic effects of propranolol appear to stem from its anticatecholamine electrophysiologic actions and not from the weak “quinidine-like"” effect that propranolol manifests at very high doses.1,39 Although β-blockers were thought to have their greatest effect on the prevention and treatment of supraventricular arrhythmias,40,41 it quickly became apparent that they were also safe and effective for the prevention and treatment of ventricular arrhythmias. 1
Subsequently, oral acebutolol, a drug with both β1-selectivity and ISA, was approved as a treatment for patients with ventricular arrhythmias, 1 and intravenous esmolol, a β1-adrenergic blocker, was approved for intravenous use to treat supraventricular arrhythmias.29,42 Finally, oral sotalol, a nonselective β-blocker with unique type III antiarrhythmic properties, was approved as a treatment for both supraventricular and ventricular arrhythmias.1,43,44
As a class of antiarrhythmic drugs, no other group of agents have shown the favorable long-term safety profile exhibited by β-blocking agents.
Hypertension
Prichard and Gillam 45 demonstrated that propranolol had antihypertensive actions, and, after resistance by some investigators, the drug was approved for clinical use as an oral antihypertensive agent. Propranolol was also used as an adjunct therapy to phentolamine in the treatment of pheochromocytoma. 36 Subsequently, labetalol in its intravenous form was determined to be of some use in the treatment of hypertensive emergencies and in an oral form for hypertensive urgencies. 19
Fourteen β-blockers have received approval for oral use in patients with systemic hypertension: the nonselective β-blockers without ISA (propranolol, nadolol, and timolol); the β1-selective agents (metoprolol, atenolol, betaxolol, acebutolol, and bisoprolol); the β-blockers with ISA (pindolol, carteolol, and penbutolol), the α-/β-blockers (labetalol and carvedilol), and the β-blocker with direct vasodilator activity (nebivolol). Sustained-release formulations of metoprolol, propranolol, and carvedilol have allowed these shorter acting β-blockers to be used once daily in hypertension.
The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure has considered β-blockers to be a first-line alternative treatment for hypertension. 46 However, recent meta-analyses with atenolol have shown that this compound is less efficacious than other antihypertensive drugs,47–49 and some have considered this a class effect of all β-blockers. Atenolol may not be an effective drug when used once daily, and more frequent oral dosing may be necessary to achieve blood pressure control at a level seen with other β-blockers and other antihypertensive drug classes. 50 In patients with angina pectoris and hypertension or congestive heart failure and hypertension, and in patients who have had myocardial infarction with hypertension, β-blockers remain important first-line treatments.48,49,51–53 When compared with other antihypertensive agents for primary prevention, however, they may be less effective in preventing strokes. 48
The Glycemic Effects in Diabetes Mellitus: Carvedilol-Metoprolol Comparison in Hypertensives (GEMINI) trial 54 compared the effects of β-blockers with different pharmacological profiles on glycemic and metabolic control in participants with hypertension and diabetes already receiving renin–angiotensin system blockade, in the context of cardiovascular risk factors. This trial compared the effects of carvedilol and metoprolol tartrate on glycemic control after equivalent blood pressure lowering; the mean glycosylated hemoglobin increased significantly with metoprolol but not carvedilol. Insulin sensitivity significantly improved with carvedilol but not metoprolol. Progression to microalbuminuria was less frequent with carvedilol than with metoprolol. Based on this and other studies, it appears that the pharmacological differences among the β-blockers can affect the utility of these agents in patients with hypertension having diabetes and those with the metabolic syndrome.55,56
Survivors of Acute Infarction
β-Blockers were the first class of pharmacologic agents to be shown conclusively to reduce mortality and reinfarction in survivors of acute myocardial infarction. In the early 1980s, a series of trials using the nonselective β-blockers timolol and propranolol demonstrated survival benefit in survivors of infarction. 28 Although the β1-selective agents, atenolol and metoprolol, demonstrated survival benefit in survivors of infarction as well, there was conflicting evidence regarding the duration of effect.28,57–59 Both oral propranolol and timolol received approval as long-term postinfarction therapy, and subsequently the β1-selective agents atenolol and metoprolol were approved for both early intravenous use and long-term oral use. Oral carvedilol given twice daily was approved for use in survivors of acute myocardial infarction with clinical evidence of left ventricular dysfunction with or without symptoms of heart failure, who are also on standard treatments and who are also receiving angiotensin-converting enzyme inhibition and other contemporary postmyocardial infarction treatments. 60 Carvedilol is now available as a once-daily sustained-release formulation. 25
Congestive Cardiomyopathy
For 25 years, β-blockers were contraindicated in patients with acute or chronic congestive heart failure because of fears that the negative inotropic effect of adrenergic blockade would further reduce myocardial function. Preliminary studies by Swedish investigators in the 1980s demonstrated the benefits and tolerability of β-blockers in patients with congestive heart failure. 61 Subsequent placebo-controlled studies with the β1-selective agents bisoprolol and metoprolol and the nonselective α-/β-blocker carvedilol demonstrated the efficacy and safety of using β-blockers to reduce the mortality risk in patients with symptomatic heart failure who were already receiving diuretics and angiotensin-converting enzyme inhibitors.62,63 Sustained-release metoprolol is approved for clinical use in patients with New York Heart Association classes II and III heart failure, and carvedilol, in both its twice-daily and sustained-release once-daily formulations, is approved for use in patients with mild to severe heart failure. Carvedilol is also approved for reducing mortality in patients with left ventricular dysfunction who are survivors of a myocardial infarction. Nebivolol has also been shown to be effective in reducing all-cause mortality and hospital admissions in older patients with congestive heart failure but is not approved for this indication.21,64 Not all β-blockers tested have been shown to significantly reduce mortality in patients with heart failure (eg, bucindolol). 65 It has been suggested that β-blockers might reduce accelerated myocardial apoptotic cell death seen in patients with cardiac dilatation and high levels of circulating plasma catecholamines. 1
Other Cardiovascular Uses
Some β-blockers are also approved for the treatment of hypertrophic cardiomyopathy to reduce the symptoms of dyspnea, angina, and syncope.1,66 Since the introduction of propranolol in the 1960s, β-blockers have been shown to be useful in treatments of patients with mitral valve prolapse, 67 with the hereditary electrocardiogram QT prolongation syndrome, 68 and for children with tetralogy of Fallot. 69
In treatment of acute aortic dissection, β-blockers are often combined with α-blockers to reduce the extent of injury. 70 The α-/β-blocker labetalol has been used as a monotherapy in acute dissection. 70 In addition, β-blockers with and without angiotensin-converting enzyme inhibitors are useful for preventing first dissections in high-risk individuals with Marfan syndrome, 71 for preventing recurrent dissection in survivors of a first dissection, 70 and for the Ehlers Danlos syndrome. 72 β-blockers are often used to reduce tachycardia and hypertension in patients with high levels of anxiety and atypical chest pain.73,74 Low-dose oral propranolol has been shown to significantly attenuate tachycardia and improve symptoms in postural tachycardia syndrome. 75
β-Adrenergic blockers will reduce perioperative ischemia, and studies published in the 1990s suggested that their routine administration before surgery provided protection against perioperative cardiovascular complications.76–78 Based on these early studies, several national organizations endorsed the perioperative use of β-blockers as a best practice in certain patients.79,80 However, more recent evidence has been accumulating to suggest that routine use of β-blockers may not benefit in many patients as was once hoped and may actually cause harm in some individuals.76,81–83 The benefit of β-blockers may be only in high-risk patients undergoing high-risk surgery. Currently, the best evidence supports their use in 2 patient groups: patients undergoing vascular surgery who have known ischemic heart disease or multiple risk factors for it and for those patients who are already receiving β-blockers for cardiovascular conditions.76,84
The results of the Perioperative Ischemic Evaluation (POISE) trial suggested that β-blockers should only be administered in the immediate preoperative period with great caution, after ensuring that the patient is clinically stable and without evidence of infection, hypovolemia, anemia, or other conditions that would make heart rate titration misleading or use of the drugs harmful. 81 The criticism of POISE was the fact that a high metoprolol extended-release dose was used in many patients who had never received β-blockers. 81 When feasible, β-blockers should be started a month before surgery, titrated to a heart rate of 60 bpm, and continued for 1 month. If the drug is then to be discontinued, it should be withdrawn gradually.76,85
Adverse Effects
After 50 years of clinical use, β-blockers have remained remarkably safe drugs when employed in the appropriate dose and in the appropriate patient populations. Definite contraindications to β-blocker use include active bronchospasm, Raynaud phenomenon, and acute pulmonary edema. 1 Patients with bradyarrhythmias and heart block can be treated with the drugs if there is concurrent artificial pacemaker use. Chronic heart failure is no longer a contraindication with carvedilol and metoprolol succinate (other agents still carry a contraindication in their prescribing information for patients with overt cardiac failure), and patients with intermittent claudication can receive the drugs but with caution.
β-blockers may cause a slight increase in body weight and can worsen mild hypoglycemia, hyperglycemia, and hyperlipidemia.86,87 The α-/β-blocker carvedilol has been shown to cause fewer metabolic problems when compared to metoprolol. 54 For years, there was a fear that continued β-blocker use just prior to coronary artery bypass surgery would put patients at risk of myocardial depression undergoing general anesthesia. However, studies with continuous perioperative β-blocker use have shown the opposite to occur, that is, better clinical outcomes and fewer postoperative arrhythmias. 88 Indeed, abrupt β-blocker withdrawal in patients with ischemic heart disease and/or heart failure can be associated with an unfavorable rebound effect and increased mortality and should be avoided whenever possible.89,90
Conclusion
Based on the concept of a functional adrenergic receptor that could mediate the effects of catecholamines, the introduction of β-blockers has caused a revolution in human pharmacotherapeutics. The use of these drugs has also clarified the importance of the sympathetic nervous system in the pathophysiology of these conditions. In addition, their introduction has opened the door to fundamental discoveries in the molecular biology of receptor function. β-blockers are not always interchangeable within the class. Pharmacological differences among them may be of clinical importance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.