
Abstract
Contrast-induced nephropathy (CIN) is a significant cause of morbidity and mortality and effective strategies for its prevention are greatly needed. The purpose of this retrospective, single-center study was to investigate whether nitrate use during percutaneous coronary artery intervention reduces the incidence of CIN. Chart review of all individuals who underwent percutaneous coronary intervention (PCI) from April 2010 to March 2011 was done. Included in the study were patients who were admitted to the hospital after percutaneous coronary artery intervention and had baseline and follow-up creatinine measured. Patients with end-stage renal disease requiring dialysis and those patients with insufficient information to calculate Mehran score were excluded. There were 199 patients who met the eligibility criteria for inclusion in this study. In the identified population, postprocedure renal function was compared between 112 patients who received nitrates prior to coronary intervention and 87 who did not. Baseline characteristics were similar between the 2 groups. Contrast-induced nephropathy was defined as either a 25% or a 0.5 mg/dL, or greater, increase in serum creatinine during the first 48 to 72 hours after contrast exposure. Overall, 43 (21.6%) patients developed CIN post-PCI. Of the patients who received nitrates, 15.2% developed renal impairment when compared to 29.9% in those who did not (odds ratio [OR] = 0.42, 95% confidence interval [CI] 0.21-0.84, P = .014). Multivariate logistic regression analysis demonstrated that nitrate use was independently correlated with a reduction in the development of contrast nephropathy (OR = 0.334, 95% CI 0.157-0.709, P = .004). Additionally, of the various methods of nitrate administration, intravenous infusion was shown to be the most efficacious route in preventing renal impairment (OR = 0.42, 95% CI 0.20-0.90, P = .03). In conclusion, the use of nitrates prior to PCI, particularly intravenous nitroglycerin infusion, may be associated with a decreased incidence of CIN.
Introduction
Contrast-induced nephropathy (CIN) is a complication of percutaneous coronary intervention (PCI) that, when present, usually develops 48 to 72 hours after exposure to contrast media. 1 –3 Considered one of the leading causes of acute kidney injury in hospitalized patients, the incidence of CIN has been reported in the range of 0% to 50%, depending on the presence of comorbidities and risk factors. 4 –10 When it does occur, it is associated with an increased morbidity, in-hospital death, and late mortality. Additionally, while less than 1% of the patients undergoing PCI ultimately require hemodialysis as a result of CIN, these patients have been shown to have an even higher in-hospital mortality and worse long-term survival. 9,10
The pathophysiology of CIN is not well understood; however, studies in animal models have proposed that decreased levels of nitric oxide may contribute to its development. 11,12 Since nitrates increase nitric oxide, these findings suggest a potential therapeutic benefit for the use of nitrates in the prevention of CIN. We evaluated the effects of nitrate administration on the incidence of CIN in patients undergoing percutaneous coronary artery intervention.
Methods and Materials
After obtaining approval from the institutional review board, we performed a retrospective chart review study to determine whether the exposure to nitrates before PCI could prevent CIN. The charts of all patients who underwent PCI between April 2010 and March 2011 were reviewed. Included in the study were patients who were admitted to the hospital after PCI and had baseline and follow-up creatinine measured. Patients with end-stage renal disease requiring dialysis and those patients with insufficient information to calculate Mehran score 13 were excluded. The baseline creatinine level was measured before the procedure, and the maximum creatinine was recorded within the first 72 hours after exposure. The CIN was defined as an increase in baseline serum creatinine of 25% or ≥0.5 mg/dL postprocedure. Nitrate use was defined as treatment with any type of nitrates, at any dose, including intravenous infusion, patch, oral or sublingual, up to 24 hours prior to, and during the procedure. All patients included in the study had PCI of at least 1 coronary artery. The PCI was performed using the low osmolar contrast agent iohexol or the iso-osmolar agent iodixanol.
The degree of hydration was evaluated and defined using a dichotomous variable, that is, those patients who received any amount of intravenous fluids including normal saline and half-normal saline before and after the procedure and those who did not. There was variability in the intravenous fluids protocol selected by different physicians, and since this was a retrospective study no standardized protocol of fluids administration was utilized. Anemia was defined as a hematocrit value <39% for men and <36% for women. Hypotension was defined as systolic blood pressure < 80 mm Hg for at least 1 hour, requiring inotropic support with medications or intra-aortic balloon pump, within 24 hours of the procedure. The risk of developing CIN was estimated utilizing the validated score proposed by Mehran et al 13 and the score was used as an independent variable in our analysis. The score was calculated using the following parameters: hypotension (5 points), intra-aortic balloon pump use (5 points), congestive heart failure (5 points), age > 75 years (4 points), anemia (3 points), diabetes mellitus (3 points), serum creatinine > 1.5 (4 points), and contrast volume used (1 for each 100 cm3).
Statistics
Continuous variables are reported as mean ± standard deviation. Categorical variables are reported as frequencies and percentages. To compare continuous variables between groups, an independent sample t test was utilized and for categorical variables a Fisher exact test or Pearson chi-square was used. Univariable logistic regression analyses were performed to identify those variables related to CIN. After univariable analysis, all variables with P values ≤.2 and those variables previously associated with CIN were included in a multivariable logistic regression model. An analysis of variance was used to compare the mean days of hospitalization in patients who developed CIN with those who did not. Standard Kaplan-Meier curves were used to assess survival using a Mantle Cox calculation. Data on survival were obtained from public online record consultation. A P value ≤.05 was considered statistically significant. The statistical analyses were performed using SPSS software (version 17.0; SPSS Inc, Chicago, Illinois).
Results
Overall, the records of 1110 patients that underwent PCI during this time period were screened. The majority of the patients were excluded due to the lack of post-PCI follow-up renal function. A small cohort was excluded because they were already on renal replacement therapy. A total of 199 patients were identified who met the inclusion criteria, of which 112 (56%) received nitrate therapy before the procedure and 87 (44%) did not. The baseline characteristics were similar between the 2 groups, with the exception that males constituted 61 (54.5%) of the 112 patients in the nitrate group and 63 (72.4%) of the 87 patients in the non-nitrate group, P = .01 (Table 1). In the nitrate group, 81 (72%) patients received intravenous nitroglycerin infusion, 16 (14%) received transdermal nitrates, 11 (10%) received oral nitrates, and 4 (4%) received sublingual nitrates (Table 2).
Baseline Characteristics of the Study Participants.

Abbreviation: SD, standard deviation.
Univariable Association of the Type of Nitrates With Contrast-Induced Nephropathy.

Abbreviations: CI, confidence interval; CIN, contrast-induced nephropathy.
Overall, 43 (21.6%) patients developed CIN post-PCI. Of the patients receiving nitrates, 17 (15.2%) developed CIN compared with 26 (29.9%) that did not receive nitrates (odds ratio [OR] = 0.42, 95% confidence interval [CI] 0.21-0.84, P = .014). Of the patients that developed acute kidney injury, most recovered to their baseline creatinine. Only 1 patient, in the nonnitrate group, developed renal impairment severe enough to require hemodialysis. Of the different modalities of nitrates used, intravenous infusion was shown to be the most efficacious route in preventing CIN, when compared with all other means of administering nitrates (OR = 0.42, 95% CI 0.20-0.80, P = .03; Table 2). Multivariable logistic regression analysis demonstrated that nitrates and intravenous fluids were both independent predictors of CIN (OR = 0.229, 95% CI 0.13-0.63, P = .002 and OR = 0.084, 95% CI 0.015-0.461, P = .004, respectively; Table 3).
Multivariable Association of Individual Variables With Contrast-Induced Nephropathy.
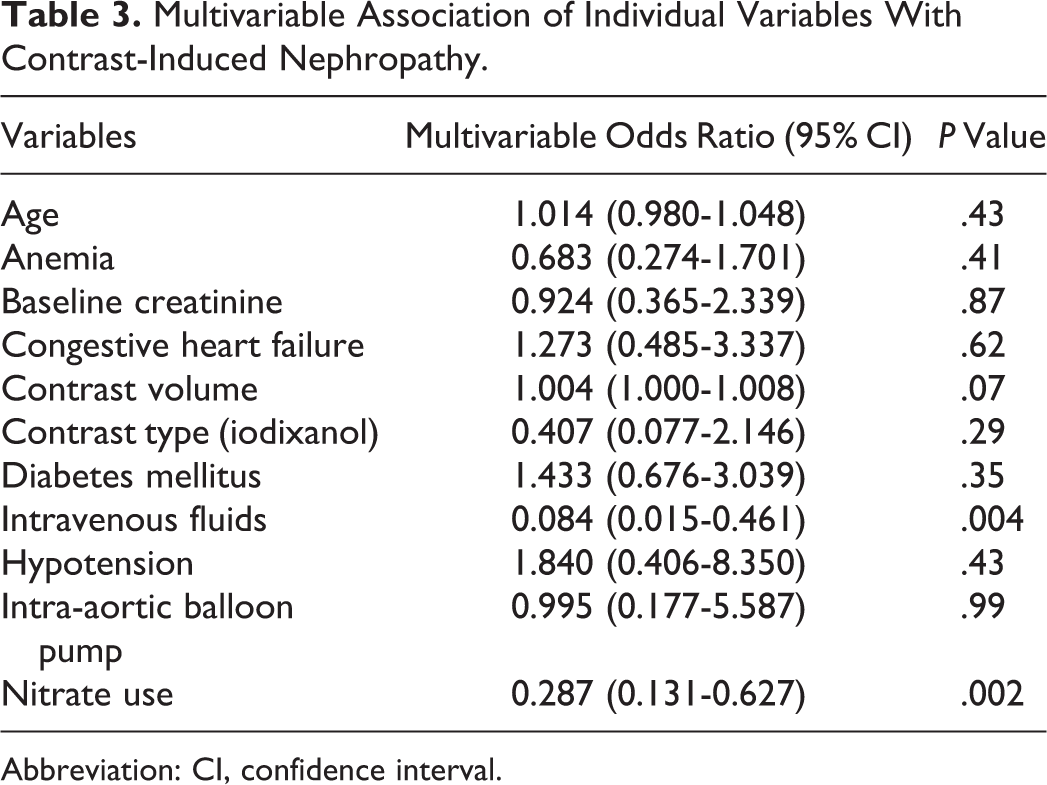
Abbreviation: CI, confidence interval.
After eliminating those patients who remained in the hospital for other elective procedures and 1 patient who developed cardiogenic shock, a comparison of the mean days of hospitalization was suggestive of longer hospitalizations on average in the patients that developed CIN when compared with patients that did not but was not statistically significant (7.3 ± 8.3 vs 5.4 ± 4.2 days, P = .16). The patients who developed CIN demonstrated a decreased 30-day survival when compared with patients without kidney impairment (88.4% vs 97.4%, P = .01; Figure 1). However, the use of nitrates did not appear to correlate with a survival benefit, P = .86 (Figure 2).

Kaplan-Meier survival curve comparing patients who developed CIN with those who did not. CIN indicates contrast-induced nephropathy.
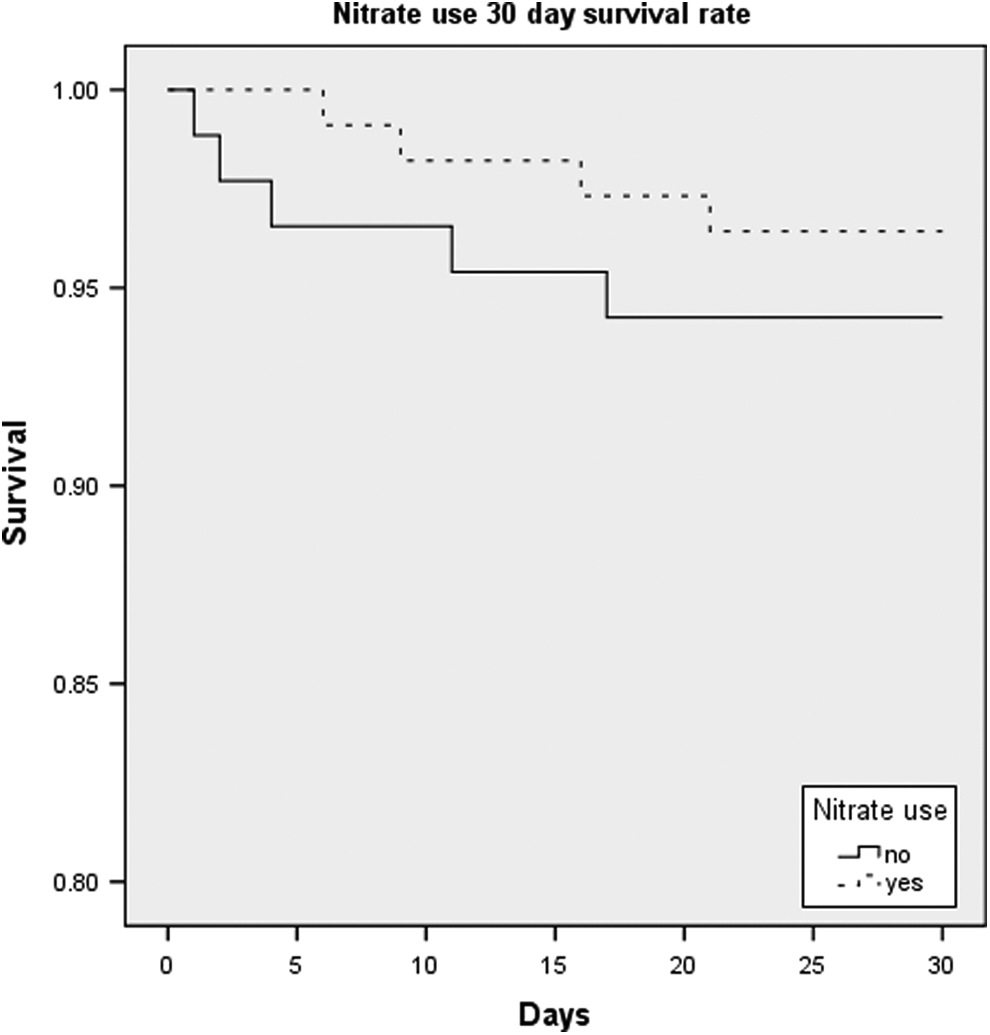
Kaplan-Meier survival curve comparing patients who received nitrates and those who did not.
Discussion
The principle finding of this study is that nitrate use, particularly, in the form of intravenous infusion may reduce the risk of development of CIN in patients undergoing PCI. The CIN remains one of the major complications of all procedures that require intravenous contrast use. To date, several prevention and treatment strategies have been proposed; however, only intravenous hydration has been proven to be effective. The positive effect of proper hydration was confirmed in the present study.
Previous studies have suggested that CIN may be caused by either renal vasoconstriction resulting in medullary hypoxemia or direct cytotoxic injury caused by the contrast agents. 14 –16 Both mechanisms are known to decrease nitric oxide synthesis and, therefore, may contribute to renal injury. 11,12 Patients with chronic renal failure, diabetes mellitus, and heart failure have already impaired nitric oxide metabolism that could account for their susceptibility to develop contrast media nephrotoxicity. 17 There have been multiple attempts to modify nitric oxide metabolism in order to prevent development of CIN. N-acetylcysteine was the most studied and the most promising compound in this regard. The proposed mechanism of action of N-acetylcysteine is stimulation of nitric oxide synthase and increased production of nitric oxide. 17 However, in patients with already impaired nitric oxide metabolism, activation of nitric oxide synthase may not generate amounts of nitric oxide sufficient for kidney protection. Nitrates bypass nitric oxide synthase, exerting their effects by direct formation of nitric oxide. We hypothesize that the protective effect of nitrates observed in this study may be related to increased levels of nitric oxide in the renal vasculature followed by vasodilation, resulting in decreased hypoxia and oxidative stress. 18,19 The increased effectiveness of intravenous infusion, when compared with other routes of administering nitrates, may be attributed to the fact that intravenous nitroglycerin infusion has the fastest onset of action and achieves higher blood levels when a continuous infusion is given. 12
The main limitation of this study is that it is a retrospective, single-center study. It did not have uniform dosing of the nitrates nor of the amount of iodinated contrast. The relationship between the timing of administration of the nitrates and its effect on renal function is not available, thus limiting the pharmacological analysis of the drug in its different preparations. There may also be significant patient selection biases that are uncontrollable confounders. This study only included those patients that were admitted to the hospital after PCI and had complete data available for analysis. Therefore, a large number of patients undergoing PCI during the study time interval were not included. Although one may speculate that those included in the study were sick enough to warrant in-patient follow-up and close monitoring, the admission criteria used by multiple physicians were nonuniform and limits the generalizability of the study. The majority of the patients were discharged the same day after PCI was performed; no follow-up was available for this population; therefore, the ability to translate the results of this study to this specific cohort is limited. The clinical care of patients selected to receive nitrates is also another confounder. Thus, the present study can only be interpreted as hypothesis generating.
Conclusions
The administration of nitrates, particularly intravenous nitroglycerin up to 24 hours prior to and during PCI, may decrease the incidence of CIN. A prospective, randomized-controlled trial using intravenous nitroglycerin closely before PCI is warranted to support or refute this hypothesis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.