
Abstract
Background:
Atorvastatin has been demonstrated to reduce the incidence of postoperative atrial fibrillation (POAF) in patients undergoing cardiac surgery, but its effect on isolated heart valve surgery is unknown.
Methods:
In a randomized, double-blinded, placebo-controlled trial, 58 patients who underwent isolated heart valve surgery supported by on-pump cardiopulmonary bypass were randomly assigned to receive either placebo (n = 29) or 40 mg of atorvastatin once daily starting 3 days preoperatively and continuing within 5 days postoperatively (n = 29). A continuous monitoring tool and an electrocardiographic Holter monitoring were used for detecting the POAF (Clinical Trial Registration: www.clinicaltrials.gov; Unique Identifier: NTC02084069).
Results:
The patients’ median age was 49 years, and 67% were female. In all, 6 (21%) and 13 (45%) cases of POAF were observed in the atorvastatin and placebo groups, respectively (P = .050). The duration of AF before re-establishment of sinus rhythm was significantly lower in the atorvastatin group than in the placebo group (median of 70 vs 132 minutes, P = .026). The lengths of intensive care unit and hospital stay were comparable between the groups. The increase in postoperative white blood cell count was significantly lower in the atorvastatin group than in the placebo group (median of 1.5 vs 2.3 × 103/µL, respectively, P = .019). After adjustment, the atorvastatin treatment was associated with a decrease in the risk of developing POAF (odds ratio 0.122, 95% confidence interval 0.027-0.548, P = .006).
Conclusion:
Perioperative treatment with 40 mg of atorvastatin is useful to decrease the incidence of POAF in the statin-naive patients undergoing isolated heart valve surgery.
Introduction
Postoperative atrial fibrillation (POAF) is a common complication following cardiothoracic surgeries. 1 Using the different definitions of arrhythmia and methods of atrial fibrillation (AF) detection, it has been reported to be more than 20% in those undergoing noncardiac surgeries 1 and 10% to 65% in those undergoing cardiac surgeries. 2 Moreover, it has been shown to be roughly 30% following isolated coronary artery bypass graft (CABG) surgery, 3,4 40% after isolated valvular surgery, 5 and approximately 60% in cases undergoing combined CABG and valvular surgery. 6 The pathophysiologic mechanisms involved in the development of POAF are not precisely known, but some etiologies have been hypothesized. Several risk factors have been shown to predict POAF, including advanced age, mitral valve stenosis, left atrium enlargement, a previous history of AF, chronic obstructive pulmonary disease, left ventricular ejection fraction (LVEF) of <30%, and heart failure. In general, the development of POAF can be attributed to the predisposing factors stated earlier, that is, perioperative factors, inflammation, and oxidative stress. 5,7 Considering the risk of thromboembolic events, such as stroke, the POAF is a substantial cause of mortality and morbidity in patients undergoing cardiac surgeries and leads to increased length of hospitalization and cost of care. 5
Some observational studies have suggested the effect of statin therapy in reducing the incidence of POAF 7,8 and the risk of stroke 7 in patients undergoing CABG surgery. In addition, some randomized clinical trials have been conducted to evaluate the impact of perioperative statin therapy on POAF incidence and adverse outcomes in patients undergoing isolated CABG 9 –18 or combined CABG and valvular surgeries. 2 However, to date, no study has evaluated how perioperative statin treatment can impact on the development of POAF in patients undergoing isolated heart valve surgery. Hence, we sought to determine the effect of perioperative atorvastatin on the occurrence of POAF in patients who underwent isolated heart valve surgery supported by cardiopulmonary bypass.
Methods and Materials
Patients and Study Protocol
This randomized, double-blinded, placebo-controlled clinical trial was conducted in the Seyyed-al-Shohada Heart Center, Urmia University of Medical Sciences, Urmia, Iran. The study was approved by the local ethics committee in our university, and written informed consent was obtained from all the participants. The trial is registered at clinicaltrials.gov (Unique Identifier: NCT02084069).
Since January 2013 to April 2014, all patients undergoing heart valve surgery were evaluated for inclusion and exclusion criteria. Inclusion criteria were as follows: (1) being >25 years, (2) having no intra- or postoperative cardiopulmonary arrest, (3) having sinus rhythm preoperatively, and (4) undergoing isolated valvular surgery supported by on-pump cardiopulmonary bypass. Exclusion criteria included a history of AF, prior use of antiarrhythmic agents, implanted pacemaker, any degree of heart block, bradyarrythmia less than 50 beats per minutes, severe heart failure or LVEF of <35%, renal failure, hepatic failure, and severe chronic obstructive pulmonary disease. Among 109 consecutive patients scheduled to undergo cardiac valve surgery, a total of 58 patients (53% recruitment rate) met inclusion and exclusion criteria. They were allocated randomly to 2 study groups, including the atorvastatin group (n = 29) and the placebo group (n = 29). All patients were randomized in a 1:1 ratio using a randomization table, and either of them received an assignment number in a sealed envelope at the time of enrollment.
All surgeries were performed by a single experienced surgery team using the standard technique. First, the patients were anesthetized using weight-adjusted doses of fentanyl, midazolam, and sodium thiopental associated with atracurium. All underwent the same standard cardiopulmonary bypass surgery. After enrollment, the patients were randomly assigned to 2 groups to receive either 40 mg of atorvastatin once daily starting 3 days prior to surgery and continued within 5 days after surgery or placebo (with shape and taste similar to atorvastatin) with the same prescription order. Both patients and the staff providing the care were blinded to the group assignments. Patients also received β-blockers, angiotensin-converting enzyme inhibitors (ACEIs), and/or warfarin postoperatively when required, regardless of the group they’re in. All cases with POAF were treated using the same intravenous amiodarone loading dose during hospitalization and continued orally for a 6-week period after discharge. The blood samples were collected at 6 to 24 hours preoperatively and 6 hours postoperatively.
Electrocardiographic Monitoring
The patients were monitored using a wearable monitoring device up to 48 hours in the intensive care unit (ICU), and then they were evaluated in the ward by an electrocardiographic Holter monitoring (Model H3+, Mortara Instrument, Wisconsin) for 72 hours.
Echocardiographic Evaluation
Parameters measured at echocardiographic examination consisted of LVEF, type of valvular involvement, and left atrium diameter.
Primary and Secondary End Points
The primary end point was the detection of any POAF during hospitalization. Postoperative atrial fibrillation is diagnosed as the occurrence of at least 1 episode of changing sinus to fibrillation rhythm lasting ≥5 minutes; all monitoring records were assessed by a single electrophysiologist. Secondary end points were as follows: (1) the ICU length of stay (LOS), (2) the hospital LOS, (3) the alteration in postoperative white blood cell (WBC) count when compared to preoperative one, (4) postoperative bleeding defined as patients required blood transfusion, and (5) the duration of AF before re-establishment of sinus rhythm.
Statistical Analysis
Continuous and categorical variables were presented as median (25th-75th percentile) and number (percentage), respectively. All categorical variables were analyzed using either chi-square test or Fisher exact test, as appropriate. Nonnormally distributed continuous variables were analyzed using the Mann-Whitney U test. The Kaplan-Meier method was also used for comparing placebo and atorvastatin groups with regard to AF-free survival rate. In addition, a binary logistic regression model was used for detecting the independent predictors of POAF. Another model was developed after adjustment for the covariates demonstrated to be significant in our first model or demonstrated to be associated with an increased risk of POAF in the literature. 4,5,9,19,20 All P values less than .05 were considered statistically significant. All analyses were performed using SPSS Version 18.0 (SPSS Inc, Chicago, Illinois).
Results
Characteristics
All enrolled patients (58) completed the trial (Figure 1). The patients’ median age was 49 years (Q1: 41 years and Q3: 60 years), and 67% were female. Baseline characteristics were similar in the groups, as shown in Table 1. The median time of intubation after surgery was significantly higher in the atorvastatin group than in the placebo group (Table 2).

Trial flowchart.
Characteristics and Clinical Features of the Patients Based on the Study Groups.a

Abbreviations: ACE-I, angiotensin-converting enzyme inhibitors; LVEF, left ventricular ejection fraction; WBC, white blood cell count.
aValues are presented as median (interquartile range) and number (percentage).
Perioperative Features and Measured End Points of the Patients Based on the Study Groups.a

Abbreviations: POAF, postoperative atrial fibrillation; ICU, intensive care unit; LOS, length of stay.
aValues are presented as median (interquartile range) and number (percentage).
Perioperative Findings and End Points
There were 6 (21%) cases with POAF in the atorvastatin group and 13 (45%) cases in the placebo group (P = .050; Table 2). In both groups, the majority of cases with POAF occurred in ward rather than ICU (67% vs 61%, P = .829). The duration of AF before re-establishment of sinus rhythm was significantly lower in the atorvastatin-treated group than in the placebo group (median of 70 vs 132 minutes, P = .026). Other measurements are summarized in Table 2.
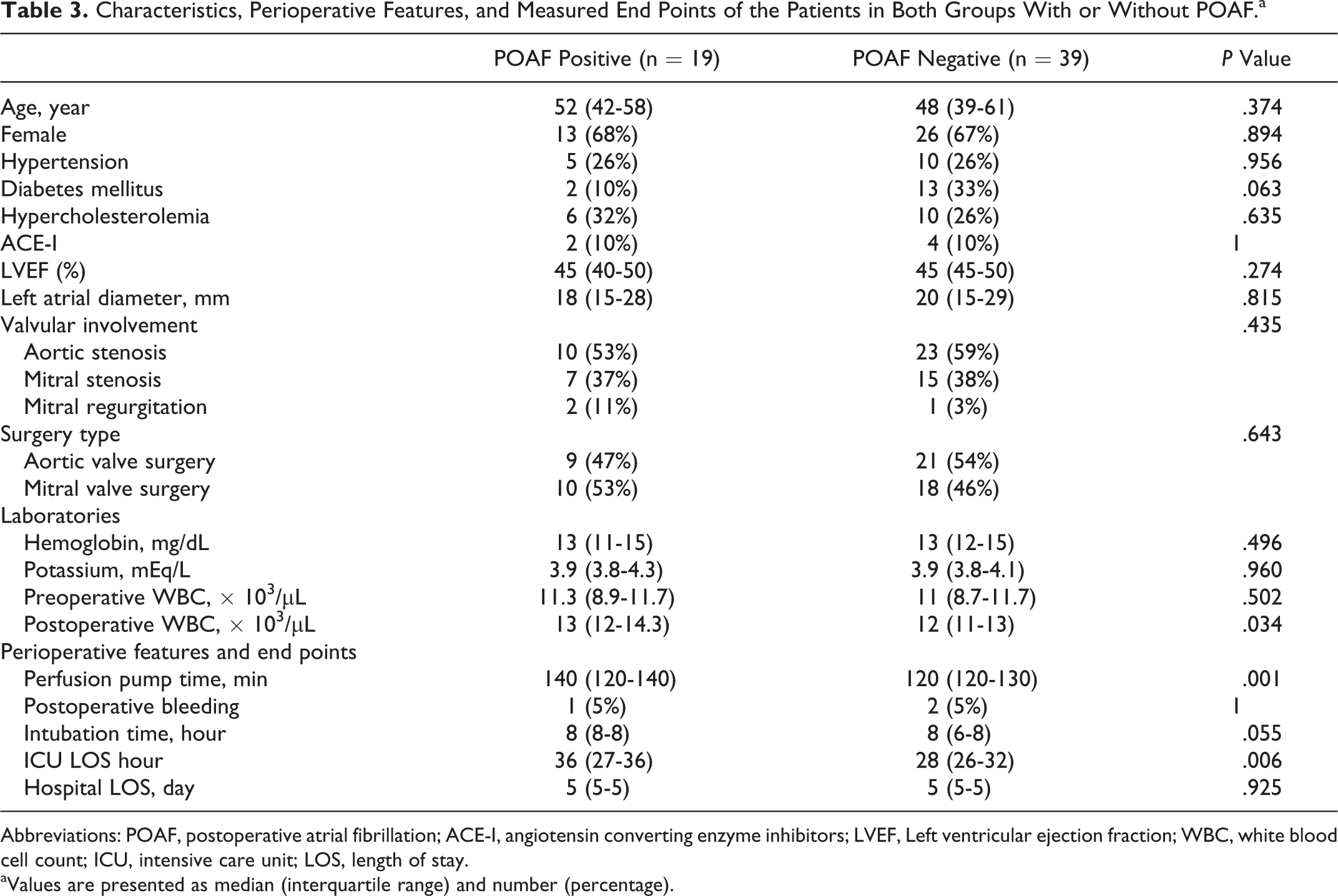
In subgroup analyses, baseline characteristics were similar in both groups (Table 3). There was a trend toward POAF-positive patients showing higher intubation time than POAF-negative ones (P = .055). The medians of perfusion time in both POAF-positive and -negative groups were 140 minutes (120-140) and 120 minutes (120-130), respectively (P = .001). The ICU LOS was significantly higher in the POAF-positive group than in the POAF-negative group (P = 0.006). The hospital LOS was comparable between patients with and without POAF (P = .925).
Characteristics, Perioperative Features, and Measured End Points of the Patients in Both Groups With or Without POAF.a
Abbreviations: POAF, postoperative atrial fibrillation; ACE-I, angiotensin converting enzyme inhibitors; LVEF, Left ventricular ejection fraction; WBC, white blood cell count; ICU, intensive care unit; LOS, length of stay.
aValues are presented as median (interquartile range) and number (percentage).
Evaluation of WBC
The preoperative WBCs were significantly lower in the atorvastatin group than in the placebo group (median of 8.9 vs 11.2 × 103/µL, respectively, P = .026); however, postoperative WBC was not significantly different (Table 1). Postoperative WBC was significantly higher in the POAF-positive group than in the POAF-negative group (median of 13 [12-14.3] vs 12 × 103/µL [11-13], respectively, P = .034). Among patients who received placebo, POAF-positive patients had higher postoperative WBC than POAF-negative patients (P = .004), while there was no such pattern in the atorvastatin group. Moreover, the amount of increase in the postoperative WBC was significantly lower in the atorvastatin group than in the placebo group (median of 1.5 vs 2.3 × 103/µL, respectively, P = .019; Figure 2).

Postoperative white blood cells (WBCs) and changes in WBC according to the study groups.
Survival Analysis
Kaplan-Meier curves were constructed to estimate the AF-free survival rate for patients receiving atorvastatin or placebo (Figure 3). According to the log-rank test, the proportion of patients remaining free of AF was significantly different between 2 groups, P = .039.

Kaplan-Meier curve showing the atrial fibrillation (AF)-free survival rate.
Multivariate Analysis
According to the multivariate analysis, the atorvastatin treatment was associated with a decrease in the POAF incidence (odds ratio = 0.109, 95% confidence interval [CI] = 0.013-0.899, P = .039). After adjustment for variables that were shown to have significant effect on the development of POAF, again the atorvastatin treatment was associated with a reduction in the incidence of POAF (odds ratio 0.122, 95% CI 0.027-0.548, P = .006; Table 4).
Logistic Regression Analysis Detecting the Predictors of POAF.

Abbreviations: ACE-I, angiotensin-converting enzyme inhibitor; CI, confidence interval; LVEF, left ventricular ejection fraction; OR, odds ratio; WBC, white blood cell count.
Discussion
In this study, we showed, for the first time, that the perioperative treatment with atorvastatin may reduce the incidence of POAF in patients who have undergone isolated cardiac valve surgery supported by cardiopulmonary bypass regardless of their baseline cholesterol levels (21% in the atorvastatin group when compared to 45% in the placebo group). Furthermore, the atorvastatin treatment was an independent factor in reducing the incidence of POAF, and we found that the perfusion pump and intubation times were also correlated with an increased risk of POAF.
As the most common sustained arrhythmia after cardiac surgeries, AF usually occurs on the second or third postoperative days. It has been demonstrated that POAF can contribute to greater mortality and morbidity by increasing the risk of stroke or myocardial infarction, and it increases the cost of care by enhancing the ICU and hospital LOS. 6,19 Some potential mechanisms have been postulated to be involved in the development of POAF, but the exact pathogenesis is unknown. Electrical and structural remodeling of the atrium may be attributed to the oxidative stress and inflammatory processes occurring during the ischemia–reperfusion phase at cardiopulmonary bypass surgery. 21,22 The principle of primary prevention of AF focusing on the mechanisms involved in the AF incidence has resulted in the development of using nonantiarrhythmic agents. These potential new pharmacological approaches to AF, which have been named upstream therapy, inhibit the progression of substrate for AF by mechanism-based prevention. 23,24 Some agents, as upstream therapies, have been postulated to have a protective role against the development of POAF, including ACEIs, angiotensin II receptor blockers, statins, nonsteroidal anti-inflammatory drugs, and antioxidant vitamins. We lack the randomized controlled trials (RCTs) for some of these agents 25 ; an RCT failed to find any efficacy for vitamin E in reducing the incidence of POAF after cardiac surgery. 26 However, the results of a recent trial, which was conducted in our institution, revealed that the vitamin C can reduce the development of POAF after CABG. 3 Statins have been used before for the prevention of POAF, and it seems that atorvastatin might protect patients against POAF through its anti-inflammatory and anti-oxidative features and through stabilizing the ion channel in cell’s phospholipid membrane. 2,27
In an observational study, 28 patients who received statin before bypass surgery had lower incidence of POAF and shorter duration of AF episode. In contrast, Miceli et al 7 showed that preoperative treatment with statin was associated with higher incidence of POAF following CABG, compared to no statin group, rather than a lower one. Despite inconsistent results of observational studies, RCTs have consistently shown a beneficial effect of atorvastatin against POAF. 2,9,11,12 Preoperative administration of atorvastatin led to a decrease in the development of POAF after off-pump CABG surgery in previous studies. 9,11,12 These studies have found a lower incidence of POAF in atorvastatin-treated patients (13%-35%) than in controls (27%-57%), which is in agreement with our findings. 2,9,11,12 Patti et al showed that atorvastatin treatment was effective in reducing POAF incidence in patients undergoing on-pump CABG surgery but not in patients undergoing isolated valve surgery. 2 We believe that the lack of atorvastatin efficacy in patients undergoing valvular surgery in their study might be attributable to the small number of such cases. The ICU and hospital LOS are substantial factors leading to increased cost of care. Most previous studies failed to find any impact for atorvastatin in reducing the ICU or hospital LOS, 9,11,12,18 except the study of Patti et al, 2 in which they showed the hospital LOS to be significantly lower in the atorvastatin group than in controls. In our study, the ICU and hospital LOS were similar in the groups, although ICU LOS was found to be longer in the POAF-positive group than in the POAF-negative ones. We believe that besides the POAF, some other factors such as operation time, complications, and perfusion pump time may also influence the LOS. Moreover, all patients in this study underwent elective isolated cardiac valve surgery without significant complications and were discharged within 5 days after surgery.
The electrophysiological remodeling of atrium is probably the mechanism involved in POAF development, which is attributable to the ischemia–reperfusion and the consequent inflammatory responses in the setting of cardiopulmonary bypass surgeries. 29 We observed a trend in POAF-positive patients for higher perfusion pump time, which was also found to be an independent predictor of POAF in our cohort. Although evidence is lacking regarding the relationship between longer cardiopulmonary bypass and increased postoperative arrhythmia, 20 it seems reasonable to assume that the inflammatory pathways activated following ischemia–reperfusion may have a potential role in developing POAF. Moreover, the need for prolonged ventilation after surgery has been shown to predict the incidence of POAF. 30 The duration of intubation is longer in patients with POAF, and the intubation time continues to predict the incidence of POAF even after adjustment for known risk factors for POAF. Besides that, the atorvastatin-treated patients, whether POAF positive or POAF negative, endured longer intubation times compared to that in the placebo group. We might speculate that the effect of atorvastatin on systemic inflammatory response, which has been confirmed by significant reduction in the postoperative WBC in atorvastatin-treated patients, has led to the longer ventilation times. However, further large-scale clinical trials would be useful to study this issue.
Aging has been shown to be a risk factor for POAF, and its risk will double by each decade increase in age 20 ; however, we could find no significant difference regarding age between the groups, and it also failed to be a predictor of POAF. Our cohort included patients with cardiac valve diseases without coronary artery disease with a median age of 49 years (41-60 years). We believe that including patients with lower age when compared to previous studies might contribute to this specific finding.
The increase in WBC has been reported to be a marker of inflammatory processes and for the development of POAF after CABG or heart valve surgeries. 31,32 Postoperative increase in C-reactive protein was also shown to be associated with enhanced risk of POAF. 9,12 All these findings indicate the potential role of inflammation in the development of POAF. In this study, we found no significant difference regarding the postoperative WBC levels between the groups, while among patients who received placebo, it was higher in the POAF-positive patients, and increase in the postoperative WBC values was significantly lower in atorvastatin-treated ones. We believe that the slight rise in WBC level following surgery in the atorvastatin group and the significantly higher postoperative WBC in POAF-positive patients than in negative ones might indicate the anti-inflammatory effect of atorvastatin or the relationship between inflammation and the development of POAF. Given including only low- to moderate-risk statin-naive patients with heart valve disease and applying rigorous inclusion and exclusion criteria, we think that the benefits of present upstream therapy may be even greater in high-risk patients. More large-scale clinical trials are deemed indicated to clarify these notions.
Our study, however, had several limitations. First, the sample size of this study was small, which is influenced by both the small number of patients with isolated valvular diseases undergoing open surgery and having the single-center design of this trial. Using strict inclusion and exclusion criteria may be considered another limitation for this study. Although one might expect that mitral valve surgeries that involves direct manipulation/suturing of left atrial tissue may predispose a patient to more POAF when compared to aortic or right-sided valve surgery. In addition, as shown in Table 4, the type of valvular surgery (mitral vs aortic valve repair) was not a predictor of POAF in this trial (P = .333).
Conclusion
This study demonstrated that perioperative treatment with 40 mg of oral atorvastatin starting 3 days prior to surgery and continuing for 5 days after surgery significantly decreased the incidence of POAF in statin-naive patients undergoing isolated cardiac valve surgery supported by cardiopulmonary bypass. Moreover, atorvastatin treatment was associated with a marked decrease in the development of POAF.
Footnotes
Author Contributions
Mohammad Reza Dehghani contributed to conception and design, contributed to acquisition, drafted manuscript, critically revised manuscript, gave final approval and agrees to be accountable for all aspects of work ensuring itegrity and accuracy. Majid Kasianzadeh contributed to design, critically revised manuscript, gave final approval and agrees to be accountable for all aspects of work ensuring itegrity and accuracy. Yousef Rezaei contributed to design, contributed to acquisition, analysis, and interpretation, drafted manuscript, critically revised manuscript, gave final approval and agrees to be accountable for all aspects of work ensuring itegrity and accuracy. Nariman Sepehrvand contributed to acquisition, critically revised manuscript, gave final approval and agrees to be accountable for all aspects of work ensuring itegrity and accuracy.
Authors’ Note
This study had completely been performed, designed, and analyzed in the Seyyed-al-Shohada Heart Center of Urmia University of Medical Sciences (UMSU) Iran.
Acknowledgments
We greatly thank all nurses of intensive care unit and the wards of Seyyed-al-Shohada Heart Center for their helps with gathering the study data properly.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.