
Abstract
Background:
With the inflammatory model of atherosclerosis taking center stage, anti-inflammatory drugs hold a promising place in the therapy of cardiovascular disease (CVD). Recent studies showed that hydroxychloroquine (HCQ) was protective against thrombovascular events in lupus erythematosus and traditional cardiovascular risk factors in patients with rheumatoid arthritis. Some preliminary experimental data have shown that it may prevent platelet activation too.
Objective:
To evaluate the antiplatelet activity of HCQ when given alone and in combination with aspirin (ASA) and compare it with ASA alone and ASA plus clopidogrel (CLOP) in healthy human volunteers.
Methods:
In part 1 of the study, 8 volunteers were given HCQ for 7 days. In part 2, 12 volunteers were randomly assigned in a 1:1:1 ratio to the 3 groups in which 2 of the 3 treatments, ASA, ASA plus CLOP, and ASA plus HCQ, were given in the 2 treatment periods separated by a 14-day washout period using the incomplete block design. Inhibition of platelet aggregation (IPA) was measured by light transmission aggregometry.
Results:
When arachidonic acid (AA) was used as agonist, HCQ given alone showed a significant reduction in platelet aggregation (11.0% ± 4.2%, P = .03). The IPA was significantly increased when ASA plus HCQ was compared with ASA alone (31.2% ± 8.1%, P = .002). This synergistic effect was not seen with adenosine diphosphate and collagen as agonists. Levels of serum 11-dehydrothromboxane B2, a stable marker of thromboxane A2 production, were not significantly different between the groups. There was also a significant decrease in fibrinogen and erythrocyte sedimentation rate values when HCQ was used alone or in combination with ASA.
Conclusion:
This study suggests that HCQ has antiplatelet properties possibly through the AA pathway (downstream to thromboxane A2 production). With possible additional beneficial effects over the traditional CVD risk factors, larger studies in the future might explore HCQ’s potential as an antiplatelet agent.
Keywords
Introduction
Platelets play an important role in the pathogenesis of atherothrombosis. 1 By interacting with dysfunctional endothelial cells, they promote thrombus formation, inflammation, and create a microenvironment suitable for the development of atherosclerotic plaques and subsequently cardiovascular disease (CVD). So, antiplatelet medications are commonly used for the primary and secondary prevention of vascular disease caused by atherosclerosis. Even after antiplatelet therapy, recurrent vascular events remain common. 2 This has led to the impetus on optimizing individual platelet therapy and to search for newer antiplatelet agents with novel mechanisms that could be used in addition to or in place of the existing regimens.
In the search for new targets against atherosclerosis, recent evidence suggests that it is not only a disorder of lipid accumulation but also a disorder of inflammation. 3 This has led to some ongoing clinical trials with anti-inflammatory drugs like methotrexate 4 and canakinumab 5 for the prevention of cardiovascular events. But these drugs do not have any beneficial effect on the other risk factors of CVD like hyperglycemia and dyslipidemia. So, an anti-inflammatory drug with additional beneficial properties modifying the risk factors will be an ideal drug candidate for the treatment of CVD.
Hydroxychloroquine (HCQ), an antimalarial, has been tried in a myriad of diseases ranging from polymorphous light eruptions to anticancer treatment. Preclinical studies have suggested that HCQ prevents platelet activation, 6 and the mechanisms proposed ranged from membrane stabilization, prevention of platelet granular release, inactivation of phospholipase A2, and inhibition of membrane bound calcium. The results were varied, when HCQ was used for preventing venous thrombosis in patients undergoing abdominal and lower limb surgeries. 7,8 But, recent studies 9,10 showed that HCQ was cardioprotective and reduced thrombovascular events in patients with lupus having antiphospholipid syndrome, and this generated a renewed interest in the putative antiplatelet activity of HCQ. Further, patients with lupus under HCQ therapy have showed lower common carotid intimal medial thickening and presented reduced circulating proatherogenic effector memory T-cell subsets. 11 Hydroxychloroquine has also shown protection against metabolic syndrome, 12 increased insulin sensitivity, 13 reduction in blood glucose and cholesterol levels in type 2 diabetes, 14 reduction in the incidence of diabetes, 15 and cholesterol, triglyceride, and low-density lipoprotein (LDL) 16 levels in patients with rheumatoid arthritis when treated with it.
Therefore, with this presumed hypothesis of HCQ’s usefulness in CVD, in the present study, we planned to evaluate the antiplatelet effect of HCQ and compare it with that of aspirin (ASA) alone and ASA plus clopidogrel (CLOP) in healthy human volunteers. In addition, we also planned to study HCQ’s effect on plasma 11-dehydrothromboxane B2 levels, which is a marker for the arachidonic acid (AA) pathway activation, and plasma fibrinogen levels, which is a marker of inflammation and an emerging independent risk factor for CVD.
Methods
This was a proof of concept study done in 2 parts. The study was conducted in Post Graduate Institute of Medical Education and Research (PGIMER), Chandigarh, India, in accordance with the principles of the Helsinki Declaration and Good Clinical Practices, with the written approval from Institutional Ethics Committee (Reference no: MS/1661/RES/1118) and included in the clinical trial registry of India (CTRI/2013/03/003485). Major inclusion criteria were male; aged 18 to 45 years; body mass index <30; healthy, based on a comprehensive medical examination, including a detailed past history; blood pressure 90 to 130 mm Hg systolic/60 to 90 mm Hg diastolic; alcohol consumption <20 g/d; smoking <10 cigarettes/d, and agreeing to refrain from alcohol and smoking during the study period. Major exclusion criteria included hematological disorders, known intolerance to any of the study drug medications, previous history of hemorrhagic risk, regular use of any medication, history of participating in any investigational new drug (IND) study in last 6 months, history of participating in any non-IND study in the past 3 months, history of taking nonallopathic drug in the past 6 months for any illness, and intake of medication affecting coagulation, fibrinolysis, or platelet function during the 2 weeks prior to inclusion. Written informed consent was taken from all the participants in the study before any study-related procedures were performed.
Study Design
Part 1 was an open-label, single-arm, and 1-treatment study. Each patient was given HCQ 400 mg/d for 7 days, and blood samples were assessed before and after the treatment.
Part 2 was a randomized, controlled, open-label, single-center, 2-period, and 3-treatment crossover study using incomplete block design. Each patient was randomly allocated to 1 of the 3 possible treatment sequences (Table 1). With HCQ’s long half-life in mind, treatment with HCQ was always taken in the second part of the sequence. Treatment periods lasted 7 days and were separated by a 14-day washout period. Treatments were (1) ASA 75 mg/d; (2) ASA 75 mg/d plus HCQ 400 mg/d (ASA + HCQ); and (3) ASA 75 mg/d plus CLOP 75 mg/d (ASA + CLOP), and blood samples were assessed before and after each treatment period. Participants were followed up for another 14 days for any adverse events. All study medications were given as oral tablets. Hydroxychloroquine sulfate and CLOP (clopiact 75 mg) tablets were from Ipca Laboratories Ltd (Mumbai, India). Aspirin (Ecosprin 75 mg, extended release; USV Ltd, Mumbai, India) was supplied as tablets available commercially.
Randomization Sequences.
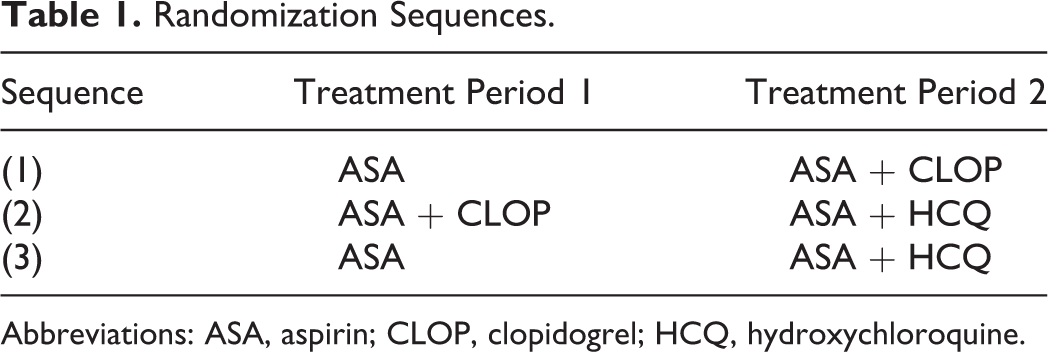
Abbreviations: ASA, aspirin; CLOP, clopidogrel; HCQ, hydroxychloroquine.
Platelet Aggregation
Fasting blood samples were collected in vials containing 3.2% (0.109 mol/L) trisodium citrate, with blood to anticoagulant ratio of 9:1. The samples were centrifuged at 800 rpm for 10 minutes at room temperature to prepare the platelet-rich plasma (PRP). The samples were further centrifuged at 3500 rpm for 15 minutes for platelet-poor plasma (PPP) and tests done within 3 hours of sample collection. Platelet aggregation was performed on the Chrono-Log platelet aggregometer (Model 700, Chrono-Log Corporations, USA) using light transmission aggregometry (LTA), with 0% light transmittance set with patient’s PRP and 100% transmittance set with patient’s PPP. The final concentration of the agonists used was adenosine diphosphate (ADP) 10 µmol/L, AA 0.5 mmol/L, and collagen (COLL) 2 µg/mL. All the agonists were from Chrono-par (Chrono-Log Corporations, USA).
For all the agonists, results were expressed as maximum aggregation intensity (%) in part 1 and inhibition of platelet aggregation (IPA) was given by the following formula in part 2: ([baseline − posttreatment]/baseline) × 100 in each patient.
Estimation of Plasma Fibrinogen Levels
The STA Fibrinogen Kit (Diagnostica Stago, France) was used on the STA Compact analyzer (Diagnostica Stago, France) for the quantitative determination of fibrinogen levels in plasma by the clotting method of Clauss, using the manufacturer’s instructions.
Estimation of 11-Dehydrothromboxane B2
Plasma 11-dehydrothromboxane B2 was measured by using specific enzyme-linked immunosorbent assay (ELISA) kit (Cusabio Life Sciences Ltd, Wuhan, PRChina) as per manufacturer’s instructions, in an ELISA reader (TECAN Mannedorf, Switzerland).
End Points
The primary end point was the mean percentage IPA with 0.5 mmol/L AA as agonist, after 7 days of treatment. The secondary end points were IPA with ADP (10 µmol/L) and COLL (2 µg/mL) as agonist and mean percentage changes in plasma 11-dehydrothromboxane B2 levels and plasma fibrinogen levels. Fasting blood glucose, lipid profile, renal function tests (urea and creatinine), and liver function tests (asparatate transaminase/alanine transaminase, serum bilirubin, serum protein and albumin) were the biochemical parameters and erythrocyte sedimentation rate (ESR), total leukocyte count (TLC), platelet, and red blood cell counts were the hematological parameters monitored before and after the treatment.
Statistical Analysis
For part 1 of the study, paired t test was used to evaluate the changes from baseline observed after the administration of HCQ. For part 2 of the study, assuming a true within patient standard deviation of 7% and a clinically important absolute difference of 10% in platelet aggregation between ASA + HCQ and ASA, a total of 12 patients was needed at an α level of .05 and a power of 80% for a 2 period by 3 treatment, incomplete block crossover design. Assuming there is no carryover effect between the 2 periods, the difference in the treatment effect between the treatment groups was evaluated using 1-way analysis of variance with Bonferroni correction and Kruskal-Wallis test based on the normality of the data. The data were expressed as mean ± standard error of the mean or median (interquartile range) according to the normality of the data. Statistical software SPSS 16.0 was used for all the analysis. A P value (2 sided) of <.05 was considered as significant.
Results
Patients
In part 1 of the study, 10 volunteers were screened and 8 enrolled in the study. They were given HCQ for 7 days and all completed the study. In part 2, 20 volunteers were screened, 6 met exclusion criteria, and 2 refused participation. In all, 12 were randomized; 4 each in 3 groups and the baseline characteristics were similar between the treatment groups.
Inhibition of Platelet Aggregation
In part 1 of the study, when AA was used as an agonist, difference in maximum aggregation was significant at 11.0% ± 4.2% (95% confidence interval [CI], 1.2-20.8, P = .03). It was not statistically significant when ADP (8.6% ± 4.1% [95% CI −1.0-18.3, P = .07]) and COLL (0.7% ± 1.6% [95% CI −3.2-4.6, P = .66]) were used as agonists (Figure 1).

Effect of hydroxychloroquine on platelet aggregation. # indicates P < .05. Error bars indicate standard error of the mean (SEM). HCQ indicates hydroxychloroquine.
In part 2, with AA as agonist, there was a significant difference in IPA between ASA + HCQ and ASA alone treated groups (31.2% ± 8.1% [95% CI 13.5-48.9, P = .002]) and between ASA + CLOP and ASA alone treated groups [22.0% ± 10.8% [95% CI 1.5-45.6, P = .01]). But there was no significant difference between ASA + HCQ and ASA + CLOP (9.2% ± 7.3% [95% CI −6.7-25.1, P = .23]). With ADP and COLL as agonists, there was a significant difference only between ASA + CLOP and ASA alone treated groups (P = .03 and P = .03, respectively; Figure 2).

Effect of different treatments on platelet aggregation. @ indicates P < .05 between groups 1 and 2, Δ, P < .05 between groups 1 and 3, and Ψ, P < .05 between groups 2 and 3 in the post hoc analysis. Error bars indicate standard error of the mean (SEM). IPA indicates inhibition of platelet aggregation; ASA, aspirin; ASA + CLOP, aspirin plus clopidogrel; ASA + HCQ, aspirin plus hydroxychloroquine; HCQ, hydroxychloroquine.
Plasma Fibrinogen Levels
In part 1, there was a significant fall of 21.4% ± 5.3% in the fibrinogen levels after the treatment with HCQ (Table 2). In part 2, there was a significant decrease in the fibrinogen levels when ASA + HCQ-treated group was compared with ASA alone and ASA + CLOP-treated group (Table 3).
Effect of HCQ on Various Parameters (Part 1).a

Abbreviations: ESR, erythrocyte sedimentation rate; S.11-DTBXB2, serum 11-dehydrothromboxane B2; TLC, total leukocyte count; HDL, high-density lipoprotein; LDLc, low-density lipoprotein calculated; AST, asparatate transaminase; ALT, alanine transaminase; HCQ, hydroxychloroquine; RBC, red blood cell; SEM, standard error of the mean.
aData given as mean (SEM).
b P value <.05 considered significant.
cData given as median (IQR).
Comparison of the Effects of 3 Different Treatments on Various Parameters (Part 2).a

Abbreviations: ESR, erythrocyte sedimentation rate; S.11-DTBXB2, serum 11-dehydrothromboxane B2; TLC, total leukocyte count; HDL, high-density lipoprotein; LDLc, low-density lipoprotein calculated; AST, asparatate transaminase; ALT, alanine transaminase; HCQ, hydroxychloroquine; ASA, aspirin; CLOP, clopidogrel; RBC, red blood cell; SEM, standard error of the mean.
aData given as mean (SEM). All parameters expressed as %c—percentage change from the baseline.
bBased on the normality of the data, One way ANOVA or Kruskal Wallis test was done.
c P value <.05 considered significant.
dTest significant between groups 1 and 2.
eTest significant between groups 2 and 3 in the post hoc analysis.
fData given as median (IQR).
gNo parameter had a significant difference between groups 1 and 3.
Plasma 11-Dehydrothromboxane B2 Levels
In part 1, there was no significant change in the plasma 11-dehydrothromboxane B2 levels before and after the treatment with HCQ (Table 2). In part 2, when the percentage fall in plasma 11-dehydrothromboxane B2 levels for ASA alone, ASA + HCQ- and ASA + CLOP-treated groups were compared, there was no significant difference between them (Table 3).
Biochemical and Hematological Parameters
In part 1, ESR was significantly decreased after treatment with HCQ. There was a statistically significant difference in the platelet and TLC. The difference in all other parameters was not statistically significant (Table 2).
In part 2, there was a significant difference in the percentage change in the ESR values and total cholesterol levels between the groups. There was a statistically significant difference in the percentage change in the platelet count and the TLC between the groups. The difference in all other parameters evaluated was not statistically significant between the groups (Table 3).
Adverse Events
Headache was the main adverse event when HCQ was given either alone or in combination with ASA. Three volunteers (2 in HCQ and 1 in ASA + HCQ-treated group) had headache, which was mild in severity and seen only during the start of the therapy. It resolved spontaneously without any treatment. One volunteer had mild diarrhoea, which subsided within a day with only oral rehydration therapy. No serious adverse events were noted during the treatment period and in the follow-up period.
Discussion
To the best of our knowledge, this is the first study to evaluate HCQ’s antiplatelet effect and compare it head-on with the commonly prescribed antiplatelet therapies, ASA alone, and ASA plus CLOP in humans. To be as objective as possible in the comparisons, the dosage choices for the 3 drugs used were based on the current clinical recommendations. The AA-induced platelet aggregation measured by LTA was taken as the primary end point as it is commonly used for evaluating ASA’s pharmacological effects and is correlated well with clinical events. 17
In part 1 of the study, when AA was used as the agonist, IPA was significant after HCQ administration. But there was no statistically significant inhibition when ADP or COLL was used as agonist. Similarly in part 2, ASA + HCQ combination had a significant increase in IPA when compared with ASA alone and it was comparable with the ASA + CLOP combination when AA was used as the agonist (a synergistic increase in IPA was noted when HCQ was given along with ASA). The platelet inhibition with ASA was not complete as we had used an extended release formulation (a commonly used formulation of ASA in Indian patients) and it coincided well with the results of another study, which compared the platelet aggregation with different formulations of ASA. 18 When ADP and COLL were used, significant difference in IPA was noted only between ASA + CLOP and ASA alone treated groups. This probably signifies that HCQ acts specifically on the AA pathway.
Thromboxane A2 produced by the cyclooxygenase (COX) pathway is quickly converted into its hydration product, thromboxane B2. This is further degraded into the long-lived stable compound, 11-dehydrothromboxane B2, and other short-lived compounds (eg, 2,3-dinor thromboxane B2). Thromboxane B2 levels are substantially liable to ex vivo artifact. So, we measured plasma 11-dehydrothromboxane B2 levels because it gives an accurate measurement of the in vivo thromboxane A2 production and correlates well with clinical end points. 19 In our study, there was no significant reduction in its level when HCQ was given. This concurred with the results of another study, which showed no inhibition of COX enzymes with HCQ. 20 So we hypothesize that HCQ’s mechanisms of action should be downstream to the production of thromboxane A2 in the AA pathway. Further mechanistic studies are needed to confirm this hypothesis. Thromboxane A2-induced platelet aggregation depends upon the secretion of other agonists from the dense granules, 21 and HCQ’s accumulation in dense granule in platelets may inhibit aggregation by decreasing the secretion of aggregation-amplifying substances from platelet granules. 22 Also, in platelets, the acidic calcium stores, which are proposed to play an important role in the platelet activation cascade, are those in lysosomes and lysosome-related organelles 23 and HCQ may prevent their release by its action on lysosomes. 24,25
Fibrinogen, an inflammatory marker, is associated with cardiovascular events and the traditional risk factors. 26 It has been shown to be an independent risk factor associated with increased mortality. 27,28 Treatment with HCQ significantly reduced the levels of fibrinogen. Anti-inflammatory activity of HCQ is further established by the significant reduction in the ESR values associated with the administration of HCQ. There was a fall in platelet and TLC associated with HCQ use, but the levels were within normal limits in all the groups and were not clinically significant.
Many studies have previously shown HCQ has a clinically significant effect on blood glucose 13,15 and cholesterol levels. 16 But, in our study, there was no statistically significant reduction in the fasting blood glucose levels. The ASA + HCQ-treated group actually showed a significant reduction in the total cholesterol levels but not in LDL cholesterol (LDL-C) and high-density lipoprotein cholesterol when compared with the other 2 groups. The nonsignificance could be due to the fact that the study was not adequately powered to find the difference in those parameters.
Various studies on HCQ have showed properties like decrease in the levels of interleukin 6, tumor necrosis factor α, and C-reactive protein 29,30 (the inflammatory markers associated with CVD), decrease in ASA esterase levels, 31 attenuation of vascular damage by improving microcirculation, 32 improvement in vascular elasticity, 33 and reduction in blood viscosity, 34 apart from its action on blood glucose 13 -15 and cholesterol. 16 All these have been noted in patients with rheumatoid arthritis or lupus and could possibly be reflected in patients with CVD. When all these beneficial effects are coupled with the antiplatelet effects (alone and in synergism with ASA) as seen in this study, it is possible that HCQ might play an important role in the management of CVD in near future and provide clinically better outcomes.
Conclusion
The results of the present study revealed that HCQ has antiplatelet properties possibly through the AA pathway (downstream to thromboxane A2 production), potentiated the antiplatelet effect of ASA, and reduced fibrinogen levels. With possible additional beneficial effects over the traditional risk factors of CVD like hyperglycemia and hyperlipidemia, as shown in other studies, future studies might focus upon the potential of HCQ as an antiplatelet and anti-inflammatory agent for the treatment of CVD.
However, this study has its own limitations. (1) The sample size was small. (2) As the patients were healthy volunteers, we did not have any clinical end points. (3) Enteric-coated ASA was used in this study (as it is being used commonly in Indian patients with CVD). (4) We were not able to show HCQ’s effect on fasting glucose and cholesterol levels, unlike some previous studies (as this study was not adequately powered to find significant differences in those parameters). Hence, clinical end point trials of larger sample size and longer duration in patients with CVD will be needed before HCQ can be used as an antiplatelet agent in the therapeutic armament for the treatment of CVD.
Footnotes
Acknowledgments
I thank Mr Sunil Kumar Bose, MSc, MLT, Senior Lab Technician, Coagulation Lab, Department of Hematology, PGIMER, for his help with the platelet aggregation studies. We thank Ipca Laboratories Ltd for providing us with the study drugs.
Author Contributions
SA, JA, NS, and SM contributed to conception and design, acquisition, analysis, and interpretation, drafted the article, critically revised the article, gave final approval, and agree to be accountable for all aspects of work ensuring integrity and accuracy; AB contributed to design, acquisition, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy; AP contributed to conception, analysis, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy; and NC contributed to conception, analysis, gave final approval, and agrees to be accountable for all aspects of work ensuring integrity and accuracy. All the authors were responsible for the design and conduct of this study. SA undertook study procedures. SA, SM, JA, and NS drafted and edited the article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AP and NC are employees at Ipca Laboratories Ltd.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No support from any organization for the submitted work except for the study drugs provided by Ipca Laboratories Ltd. AP reports obtaining a research grant and a pending patent for a pharmaceutical combination with HCQ as a component, licensed to Ipca Laboratories Ltd.