
Abstract
Background:
The well-described morning peak in the onset of acute coronary syndromes has been partly attributed to increased platelet activity upon arising. It has been suggested that stent thrombosis (ST) exhibits a similar pattern. We assessed whether a diurnal variation in ST occurs, and whether more robust antiplatelet therapy with prasugrel (vs clopidogrel) can attenuate a morning excess.
Methods and Materials:
Patients from the Trial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet Inhibition with Prasugrel–Thrombolysis in Myocardial Infarction (TRITON-TIMI) 38 trial (N = 13 608) with adjudicated ST classified per the Academic Research Consortium definitions of definite (N = 135) and probable (N = 27) were grouped into prespecified 8-hour intervals by time of onset: early (6
Results:
A diurnal variation in definite/probable ST was observed with rates of 6.5, 3.7, and 2.1 for early, late-day, and overnight intervals, respectively (P < .001), per 1000 patients treated. A sensitivity analysis excluding periprocedural acute-ST (<24 hours after index percutaneous coronary intervention [PCI]) resulted in similar findings (5.2, 2.5, and 1.8 per 1000, P < .001). The circadian variation in ST was observed in patients on clopidogrel (9.7, 4.8, and 3.1 per 1000, P < .001) with the highest rate of ST early in the day. Patients on prasugrel also demonstrated a circadian variation with particularly low rates of overnight ST (3.4, 3.0, and 1.1 per 1000, P = .020).
Conclusions:
In TRITON-TIMI 38 trial, the timing of ST exhibited a significant diurnal variation similar to that seen with onset of other acute coronary syndromes. ST occurred less frequently among patients randomized to prasugrel compared to clopidogrel with the greatest absolute reduction (6.2 per 1000 patients) in events earlier in the day when platelet activity is known to be highest.
Introduction
Stent thrombosis (ST) is a feared complication of percutaneous coronary interventions (PCIs) which carries a high risk of mortality and is more common in patients treated with PCI for an acute coronary syndrome (ACS) than with stable coronary artery disease.1–3 Observational studies have suggested that ST exhibits a diurnal variation with a higher incidence during the morning hours, but these studies required angiographic confirmation of ST that potentially exclude a large number of events due to high mortality prior to angiography.4,5 If a circadian variation of ST does exist, identification of factors that alter the timing of ST may provide insight into the biological processes responsible for the triggering of these events and lead to more effective therapies. In other forms of ACS, aspirin and β-blockers have been shown to attenuate the morning excess of myocardial infarction (MI) and helped identify platelet activity and adrenergic tone as mediators of a circadian variation.6–8 Using data from the Trial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet Inhibition with Prasugrel–Thrombolysis in MI (TRITON-TIMI 38) trial,9,10 we sought both to confirm the presence of a circadian variation in ST and to assess the effects of more robust platelet inhibition on the timing of events.
Methods and Materials
The TRITON-TIMI 38 trial was an international double-blind, randomized clinical trial comparing the effectiveness of 2 platelet P2Y12 receptor antagonists in patients with ACS and a planned PCI. The details of this trial have been described previously.9,10 Briefly, the trial included 13 608 patients with ACS who were randomized to either prasugrel (60 mg loading dose, 10 mg/d maintenance dose) or clopidogrel (300 mg loading dose and 75 mg/d maintenance dose) at the time of PCI in a double-blind manner. The inclusion criteria for patients with unstable angina or non-ST-segment elevation MI were ischemic symptoms lasting ≥10 minutes within 72 hours of randomization, a TIMI risk score of ≥3, and 1 mm ST-segment deviation or cardiac biomarker elevation. Patients with ST-segment elevation MI could be enrolled within 12 hours after the onset of symptoms if primary PCI was planned or within 14 days after receiving medical treatment for ST-segment elevation MI. The major exclusion criteria included high baseline risk of bleeding, anemia, thrombocytopenia, known intracranial pathology, or recent P2Y12 receptor antagonist use. The primary efficacy reported in TRITON-TIMI 38 trial was a composite of cardiovascular death, nonfatal MI, or nonfatal stroke and was reduced with prasugrel versus clopidogrel (9.9% vs 12.1%, hazard ratio [HR] 0.81, 95% confidence interval [CI] 0.73-0.90, P <.001) as was the rate of ST (1.1% vs 2.4%, HR 0.48, 95% CI 0.36-0.64, P < .001). 10
ST was a prespecified end point in TRITON-TIMI 38 trial and was classified by the Academic Research Consortium (ARC) Definition as follows: (1) definite, angiographic, or pathological confirmation of coronary thrombus in the setting of ACS; (2) probable, any unexplained death within 30 days or ACS involving the target vessel territory without confirmation by angiography; and (3) possible, any unexplained death beyond 30 days. 11 Adverse events, including ST, other clinical cardiovascular events, and all deaths were adjudicated by an independent clinical end point committee that was blinded to treatment assignment. Event times were also determined by the end point committee as the time of symptom onset or time of sudden death. For patients with more than 1 occurrence of ST, only the first event was considered. Noncompliance with dual antiplatelet therapy was reported if a patient did not adhere to the study medication at any point during the clinical trial, but the timing of nonadherence in relation to the episode of ST was not recorded.
We included the 162 patients with ARC definite or probable ST in our analyses. Based on our prior work in patients with ST-segment elevation MI, we anticipated a late morning peak in events would occur and that 6
Results
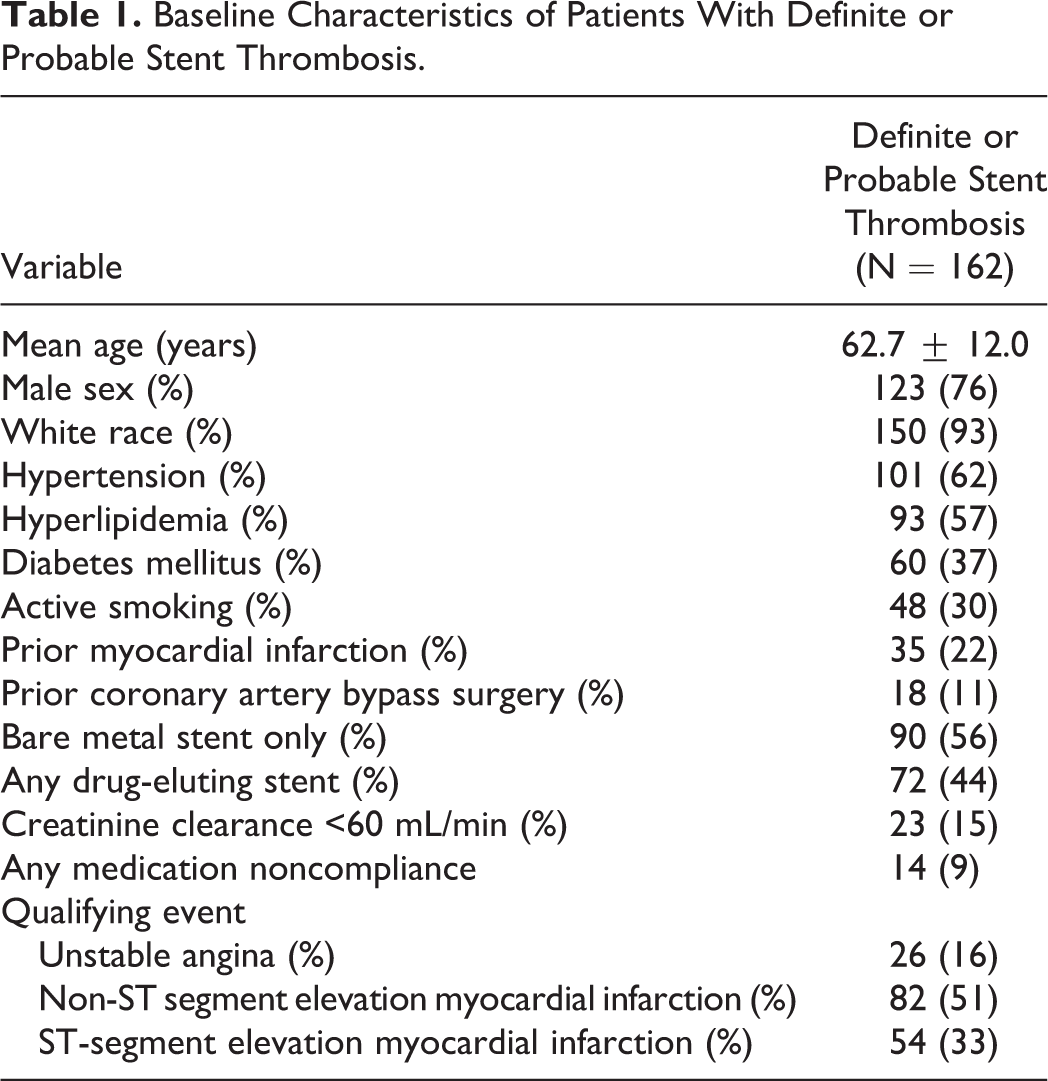
The baseline characteristics for the 162 patients (135 definite, 27 probable ST) with event times are reported in Table 1. The 44 cases of ST without a reported time of onset were excluded from this analysis. There were 40 cases of acute ST, 79 cases of subacute ST, 34 cases of late ST, and 9 cases of very late ST.
Baseline Characteristics of Patients With Definite or Probable Stent Thrombosis.
A circadian variation in definite/probable ST was observed with the highest incidence in the early cohort compared to late day and overnight (Figure 1). Patients who received either of the 2 P2Y12 inhibitors exhibited a significant circadian variation when compared to the null hypothesis of a uniform distribution. There was a particularly pronounced peak in early events with those randomized to clopidogrel and a low number of overnight events with prasugrel (Figure 2). No significant difference was observed in the circadian distribution of patients on clopidogrel versus prasugrel (P = .51), but there were statistically significant decreases in ST from 6

Definite or probable stent thrombosis (ST) by time of event. Academic Research Consortium defined definite (N = 135) and probable (N = 27) ST were significantly more common from 6

Stent thrombosis (ST) by assigned P2Y12 receptor antagonist. In Trial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet Inhibition with Prasugrel–Thrombolysis in Myocardial Infarction 38 trial, fewer ST events were observed in patients randomized to prasugrel compared to clopidogrel with a circadian variation observed in both the groups. The greatest absolute reduction in events (6.2 per 1000 patient randomized) was observed when platelet activity is highest in the earlier part of the day (P < .001). The circadian distribution with clopidogrel versus prasugrel did not reach statistical significance (P = .51).

Stent thrombosis by assigned P2Y12 receptor antagonist, alternate time intervals. A sensitivity analysis was performed using alternate 6-hour time intervals to validate the arbitrary selection of the initial 8-hour cohorts. Similar findings were observed regardless of the chosen time intervals.
Subacute ST was the most common form of ST (48.8%, N = 79) and displayed a circadian variation (per 1000 patients randomized, early 7.3 [N = 47], late-day 2.5 [N = 16], and overnight 2.5 [N = 16], P < .001). Acute ST was less frequent overnight (per 1000 patients randomized, early 1.3 [N = 17], late-day 1.5 [N = 19], overnight 0.3 [N = 4], P = .007). No significant circadian variation was observed with late ST (early 2.2 [N = 14], late-day 2.0 [N = 13], overnight 1.1 [N = 7] per 1000 patients randomized, P = .28). Exclusion of the periprocedural acute events into nonacute (all ST >24 hours after index PCI) revealed a predominance of events early in the day (early 5.2 [N = 67], late-day 2.5 [N = 32], and overnight 1.8 [N = 23], per 1000 patients randomized, P < .001).
A circadian variation persisted regardless of stent type (any DES: early 6.3 [N = 40], late-day 3.3 [N = 21], and overnight 1.7 [N = 11] per 1000 patients randomized, P < .001; only BMS: early 6.9 (N = 44), late-day 4.7 (N = 30), and overnight 2.5 (N = 16) per 1000 patients randomized, P = .001).
Discussion
Our analysis demonstrates a diurnal variation in the incidence of ST in the TRITON-TIMI 38 trial with a peak from 6
When analyzing the circadian variation of an ACS related to coronary stent implantation, it is critical to consider the impact of logistical issues that may alter the time of events. It is well established that the majority of PCI for non-ST elevation MI or unstable angina occur during routine working hours
14
which may affect the time of onset of an acute ST, since ST occurring <24 hours after the index procedure is more likely due to procedural complications such as stent underexpansion.
15
After excluding these 40 periprocedural events in the TRITON-TIMI 38 trial, a prominent circadian rhythm remained with an approximately 3-fold increase in the incidence of ST from 6
ST has been attributed to a number of factors, including noncompliance with dual antiplatelet therapy, stent underexpansion, delayed neointimal strut coverage, positive remodeling leading to acquired strut exposure, and an augmented underlying inflammatory response. 18 Platelet activity has been implicated as an important trigger for converting a subclinical arterial abnormality into a ST. 19 The biological plausibility of a circadian variation is suggested by the observation that platelets are more active upon arising and assuming an upright position.20,21 In addition, the highest number of new active platelets appear in the blood stream shortly after waking. 22 Since the time to maximum platelet inhibition for clopidogrel is 2 to 4 hours and the active metabolite has a half-life of only 0.5 hours,23,24 we hypothesize that fresh platelets may be circulating for some of the day before being exposed to irreversible P2Y12 inhibition, even if clopidogrel is dosed in the morning. In contrast, prasugrel reaches peak platelet inhibition after 1 hour, and the active metabolite has a half-life of 3.7 hours,23,24 theoretically making it less susceptible to this effect. Although this offers some biological plausibility, we also acknowledge that the circadian effects of daily dosing may be rendered insignificant by the irreversible inhibition of the P2Y12 receptor with both the drugs, and the overall more robust platelet inhibition with prasugrel may be primarily responsible for our findings.
We acknowledge a number of limitations associated with this analysis. The timing of a ST relies on subjective findings such as symptom onset and can be limited by its susceptibility to recall bias. There were 44 (21%) events without a reported time of ST; however, had all these events occurred overnight, there still would have been an excess of morning ST. We acknowledge that some of the subgroup analyses have small numbers of events, and therefore cannot rule out type II error. We were also unable to fully quantify medication noncompliance at the time of ST; however, it was unlikely to be substantial given the low rates of overall noncompliance (<10%) reported in patients with ST during the clinical trial. Technical details of the index PCI were not available and may alter the risk of subsequent ST. We also cannot comment on the timing of ST after PCI is performed for stable disease, as the TRITON-TIMI 38 trial included only patients with acute coronary syndromes.
Summary
The incidence of ST in the TRITON-TIMI 38 trial exhibited a circadian variation with the highest number of events in the early day, between 6
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following conflicts of interest with respect to the research, authorship, and/or publication of this article: The TIMI Study Group (of which Dr. Mogabgab is a research fellow and remaining authors are current members) received research grant support for the TRITON-TIMI 38 trial from Daiichi-Sankyo and Lilly. Dr. Giugliano has received honorarium from Daiichi-Sankyo for consulting and CME lectures. Drs. Braunwald (CME lectures) and Sabatine (consulting and CME lectures) have received honoraria from Daiichi-Sankyo and Lilly.
Funding
The author(s) received no financial support for the research,authorship, and/or publication of this article.